ABSTRACT
BACKGROUND AND OBJECTIVES:
Aging adds to the prevalence of chronic diseases and functional impairment. Depressive symptoms and chronic low back pain affect an increasing number of elderly people and become important research topics. This study aimed to identify the relationship between chronic low back pain intensity, its generated disability, and the presence of depressive symptoms in independent elderly people for basic daily activities.
METHODS:
The study is descriptive, quantitative, and cross-sectional. A sample of independent elderly patients with chronic low back pain (n=46) enrolled in the Family Health Units of the city of São Carlos, SP, Brazil, was analyzed. For collection, we used the Characterization Sheet, Multidimensional Pain Rating Scale, Roland-Morris Disability Questionnaire, and the Geriatric Depression Scale. The data obtained were input in the Statistical Package for Social Sciences software (SPSS) for Windows to perform the descriptive and Spearman correlational analysis. The ethical precepts for research with humans of the National Health Council were respected.
RESULTS:
The most frequent pain intensity perceived by the elderly was intense (43.5%, n=20), preceded by moderate pain (41.3%, n=19). Most of the elderly describe low back pain as persistent, painful, and uncomfortable. The mean total depression score was 4.37 points (Md=4.00, SD=2.67, xmin = 0.00, xmax = 11.00).
CONCLUSION:
Correlational analyses showed that there is a significant directly proportional relationship between the intensity of low back pain and the number of weak depressive symptoms, and a significant directly proportional relationship between the number of disabilities/limitations caused by low back pain and the number of moderate depressive symptoms.
Keywords:
Chronic pain; Depression; Disability; Gerontology; Health of the elderly; Low back pain
RESUMO
JUSTIFICATIVA E OBJETIVOS:
O envelhecimento agrega em aumento da prevalência de doenças crônicas e prejuízo funcional. Os sintomas depressivos e a dor crônica lombar afetam um número crescente de idosos e se tornam temas importantes de investigação. Este estudo teve como objetivo identificar a relação entre a intensidade de dor lombar crônica, sua incapacidade gerada e a presença de sintomas depressivos em idosos independentes para as atividades básicas de vida diária.
MÉTODOS:
O estudo é de caráter descritivo, quantitativo e de corte transversal. Foi analisada uma amostra de idosos independentes com quadro de dor lombar crônica (n=46) cadastrados nas Unidades Saúde da Família do município de São Carlos, SP. Para a coleta foram utilizados: Ficha de Caracterização, Escala Multidimensional de Avaliação da Dor, Questionário de Incapacidade de Roland-Morris e a Escala de Depressão Geriátrica. Os dados obtidos foram digitados no programa Statistical Package for Social Sciences (SPSS) for Windows para realização de análises descritivas e análise correlacional de Spearman. Os preceitos éticos do Conselho Nacional de Saúde sobre pesquisas com seres humanos foram respeitados.
RESULTADOS:
A intensidade mais frequente de dor percebida pelos idosos foi a intensa (43,5%, n=20), precedida pela moderada (41,3%, n=19). A maioria dos idosos descreve a dor lombar como dolorosa, persistente e desconfortável. O escore total médio de depressão foi de 4,37 pontos (Md=4,00; DP =2,67, xmín =0,00, xmáx =11,00).
CONCLUSÃO:
As análises correlacionais evidenciaram que existe relação significativa e diretamente proporcional entre a intensidade da dor lombar e o número de sintomas depressivos de magnitude fraca, e uma relação significativa e diretamente proporcional entre o número de incapacidades/limitações provocadas pela dor lombar e o número de sintomas depressivos de magnitude moderada.
Descritores:
Depressão; Dor crônica; Dor lombar; Gerontologia; Incapacidade; Saúde do idoso
INTRODUCTION
The world population is in the process of demographic transition, leading to an inversion of the age pyramid11 Closs VE, Schwanke CH. A evolução do índice de envelhecimento no Brasil, nas suas regiões e unidades federativas no período de 1970 a 2010. Rev Bras Geriatr Gerontol. 2012;15(3):443-58.. Data show that this increase went from 62.57 years in 1980 to 73.17 years in 2009. It is estimated that this expectation can reach 81.29 years in 2050, causing a significant increase in the proportion of elderly in the population22 Santos CT. Envelhecimento no Brasil: da formulação de políticas à estruturação de serviços de saúde integrais. Tempus, Actas de Saúde Colet. 2014;8(1):65-70..
Although the aging process is not necessarily related to diseases and disabilities, chronic-degenerative diseases are often found among the elderly. Thus, there is a growing number of individuals who, despite living longer, present chronic conditions, leading to a greater need to improve the knowledge about the factors that affect the prevalence of age-related noncommunicable chronic diseases (NCDs)33 Leandro LA, Teive HA. Fatores associados ao desempenho funcional de idosos portadores da doença de Parkinson. Rev Kairós Gerontol. 2017;20(2):161-78..
Depression is a severe health problem in the general population and the elderly, and it is defined and diagnosed by the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) as a mental illness that can lead to the aggravation of chronic degenerative or disabling diseases and compromise the quality of life44 Vilela ALS. Manual prático de Geriatria. 2ª ed. Rio de Janeiro: Guanabara-Koogan; 2017. 57-76p.,55 World Health Organization. Dementia [acesso em 8 maio de 2019] disponível em: http://www.who.int/mediacentre/factsheets/fs362/en/;2016.
http://www.who.int/mediacentre/factsheet...
. Alexopoulos et al.66 Alexopoulos GS, Abrams RC, Young RC, Shamoian CA. Cornell Scale for Depression in Dementia. Biol Psychiatry. 1988;23(3):271-84. described the loss of interest in usual activities, loss of appetite, difficulty to fall asleep, increased irritability, anxiety, and suicidal ideation as the main depressive symptoms in the elderly.
Lawrence et al.77 Lawrence V, Murray J, Banerjee S, Turner S, Sangha K, Byng R, et al. Concepts and causation of depression: a cross-cultural study of the beliefs of older adults. Gerontologist. 2006;46(1):23-32. pointed out that the concept of depression varies in different ethnic and age groups and can be mistaken in the general population as bad mood, hopelessness, and state of concern. A review study conducted in 2011 found that depression in the elderly is associated with a higher incidence of cognitive impairment, which in turn may be a predictor of dementia88 Engmann B. Mild cognitive impairment in the elderly: a review of the influence of depression, possible other core symptoms, and diagnostic findings. GeroPsych: J Gerontopsychol Geriatr Psychiatry. 2011;24(2):71-6.. According to Hayde99 Hayde L. Examining the Association of Intergenerational Relationships and Living Arrangement on Depression Prevalence in Home Health and Hospice Patients Age 65 and Older. Thesis, Georgia: State University; 2019., although the elderly are more likely to develop depression, it is not a normal part of aging99 Hayde L. Examining the Association of Intergenerational Relationships and Living Arrangement on Depression Prevalence in Home Health and Hospice Patients Age 65 and Older. Thesis, Georgia: State University; 2019..
In addition to depression, pain is a common clinical condition in old age, often underestimated and undertreated1010 Gomes JC, Teixeira MJ. Dor no idoso. Rev Bras Med. 2007;63(11):45-54.. The International Association for the Study of Pain (IASP) defines pain as an unpleasant sensorial and emotional experience, associated with actual or potential tissue injury, and described as continuous or recurrent pain, lasting at least for three months. This symptom is an individual experience that interferes with the well-being and may directly compromise the functional capacity1111 Merskey H, Bogduk N. Classification of chronic pain: descriptions of chronic pain syndromes and definitions of pain terms. IASP Pain Terminology. 1994. 240p.,1212 Dellaroza MS, Pimenta CA, Lebrão ML, Duarte YA. [Association of chronic pain with the use of health care services by older adults in Sao Paulo]. Rev Saude Publica. 2013;47(5):914-22. Portuguese..
Considering the criteria established by the IASP - absence of an apparent biological basis and duration for three months or more, “the prevalence of chronic pain in the general population of developed countries indicates an average of 35.5%, varying from 11.5 to 55.5 %, being of intense characteristic in 11% of the adults”1313 de Figueiredo VF, Pereira LS, Ferreira PH, Pereira AM, de Amorim JS. Incapacidade funcional, sintomas depressivos e dor lombar em idosos. Fisioter Mov. 2013;26(3):549-57..
Low back pain (LBP) is defined as localized pain, tension, or stiffness in the region between the last ribs and the gluteal line1313 de Figueiredo VF, Pereira LS, Ferreira PH, Pereira AM, de Amorim JS. Incapacidade funcional, sintomas depressivos e dor lombar em idosos. Fisioter Mov. 2013;26(3):549-57.. It is classified as specific when the symptoms are caused by defined clinical conditions, or as non-specific, when the pain mechanism is not clearly defined.
The spine is one of the musculoskeletal structures that most undergo morphological changes, causing physical limitations with aging, and the lumbar region is referred to as the most frequent cause of musculoskeletal disorders1414 Pinheiro RC, Uchida RR, Mathias LA, Perez MV, Cordeiro Q. Prevalência de sintomas depressivos e ansiosos em pacientes com dor crônica. J Bras Psiquiatr. 2014;63(3):213-9..
In Brazil, it is estimated that around 30 to 40% of the population is affected by chronic pain1414 Pinheiro RC, Uchida RR, Mathias LA, Perez MV, Cordeiro Q. Prevalência de sintomas depressivos e ansiosos em pacientes com dor crônica. J Bras Psiquiatr. 2014;63(3):213-9., and the elderly complain twice as much of pain1414 Pinheiro RC, Uchida RR, Mathias LA, Perez MV, Cordeiro Q. Prevalência de sintomas depressivos e ansiosos em pacientes com dor crônica. J Bras Psiquiatr. 2014;63(3):213-9., making this symptom a challenge for the health professionals, especially because pain is a subjective factor1515 Bottega FH, Fontana RT. Pain as the fifth vital sign: use of the assessment scale by nurses in general hospital. Texto Contexto Enferm. 2010;19(2):283-90..
In the elderly, it is frequent that depressive and LBP symptoms lead to greater susceptibility to functional impairment, undermining body functions, difficulty in performing daily activities, and restriction of social participation1313 de Figueiredo VF, Pereira LS, Ferreira PH, Pereira AM, de Amorim JS. Incapacidade funcional, sintomas depressivos e dor lombar em idosos. Fisioter Mov. 2013;26(3):549-57.. However, studies have shown that 30 to 60% of individuals with LBP have depressive symptoms that directly influence recovery time1313 de Figueiredo VF, Pereira LS, Ferreira PH, Pereira AM, de Amorim JS. Incapacidade funcional, sintomas depressivos e dor lombar em idosos. Fisioter Mov. 2013;26(3):549-57..
Given the above, the objective of this study was to investigate whether the relationship between LBP and depressive symptoms remains in older people who do not have any impairment in their basic daily life activities (BDLA). Another interesting aspect would be to evaluate and characterize, using a specific and standardized methodology, the disability that chronic LBP brings to the elderly.
METHODS
A descriptive, quantitative, cross-sectional study conducted in the city of São Carlos, a mid-size municipality located in the interior of the state of São Paulo. According to the 2010 Demographic Census, the total number of inhabitants in this municipality was 221,950 and the total number of people aged 60 or over was 28,868, which was approximately 13% of the total population1616 Demografia e Saúde. Atlas do Desenvolvimento Humano no Brasil (Org.) [acesso em 25 janeiro de 2019] disponível em: (http://www.atlasbrasil.org.br/2013/).
http://www.atlasbrasil.org.br/2013/...
. The city had 14 Family Health Units (FHU) in the urban area and two units in the rural area, covering 39,768 inhabitants1717 Dados da Cidade. Prefeitura Municipal de São Carlos. [acesso em 30 novembro de 2018] disponível em: http://www.saocarlos.sp.gov.br/.
http://www.saocarlos.sp.gov.br/...
.
The survey of the possible participants was carried out at the FHU, and the members of a “Health and Aging” Research Group collected the data.
The participants in this study were 46 independent old people, according to the Katz Index, who reported chronic low back pain (CLBP) in regions 30 and 31 of the item “Location of pain” of the Multidimensional Pain Evaluation Scale (EMADOR).
The inclusion criteria for the elderly were aged 60 or older; be registered in one of the FHU of the city of São Carlos; live with another independent old person in the same house; be independent for the BDLA; have CLBP; be able to understand the interview questions; sign the Free and Informed Consent Term (FICT).
From the approximate total number of older people attended at the FHU of the city of São Carlos - 5130, it was estimated that 351 individuals would constitute a sample with a 95% confidence level and 5.0% margin of error. This calculation was performed by the Survey Monkey® platform, available at <https://en.surveymonkey.com/mp/sample-size-calculator/#>. Thus, the data from 351 elderly were analyzed, but only 46 had chronic LBP and met the inclusion criteria (Figure 1). The sample size corroborates the data from the literature since 13.11% of the elderly had CLBP.
Figure 1 shows the composition of the sample from the data collection conducted by the “Health and Aging” Research Group.
Each of the FHUs provided a list of the households with two or more older adults registered in the area of coverage with their respective names, age, and address. With this list, we visited the houses, and the residents were informed about the objectives of the study.
All participants were informed about the objectives of the study, consulted about their willingness to participate and assured about the confidentiality of the individual information. The instruments chosen for data collection were validated for the Brazilian culture and are widely used in the academic-scientific environment.
It is important to point out that the individuals were allowed to participate only after signing the FICT. No physical or psychic injury was observed in the procedures described in this study. During data collection, the participant was informed about the right to drop out of the study without the need for justification.
The data was collected during interviews conducted by members of the Research Group at the household of the elderly, or in places previously agreed at the participant’s convenience.
One of the data collection instruments used was the Elderly Characterization form. It is a questionnaire designed for this project to collect the demographic data of the participants.
The Multidimensional Pain Evaluation Scale (EMADOR), validated for the Portuguese language in 2010, was also used to legitimize, subjectively, and statistically, the pain evaluation. The instrument has descriptors that make it possible to analyze the sensorial, affective, and cognitive dimensions of pain. It is a fast, practical, reliable, sensitive, and valid instrument. The study by Sousa et al.1818 Sousa FF, Pereira LV, Cardoso R, Hortense P. Escala multidimensional de avaliação de dor (EMADOR). Rev Latino-Am Enfermagem. 2010;18(1):3-10. showed that measurements have the methodological rigor, replicability for scientific research, the possibility of monitoring and analysis of the mechanisms of action of different drugs and other therapeutic approaches.
It consists of four parts. The first tracks and characterize the pain (absence or presence of pain, type of pain: chronic or acute). The second is the Numeric Pain Rating Scale in which the participant indicates the intensity of his/her pain on a scale from zero to 10, zero indicating “no pain,” 10 “maximum pain.” There is a classification of pain derived from these scores: none (zero points), light (1 to 3 points), moderate (4 to 6 points), severe (7 to 9 points) and unbearable (10 points).
The third part classifies pain according to pre-established descriptors. In this study, only chronic pain descriptors were used: depressing, persistent, distressing, disastrous, harmful, painful, unbearable, frightening, cruel, and uncomfortable. The last part of the instrument refers to the site of the pain, used as inclusion criteria for sample selection. Only subjects with pain in the regions 30 and 31 participated in this study1818 Sousa FF, Pereira LV, Cardoso R, Hortense P. Escala multidimensional de avaliação de dor (EMADOR). Rev Latino-Am Enfermagem. 2010;18(1):3-10..
The Roland Morris Disability Questionnaire (RMDQ), was developed by Roland and Morris in 1983 to assess pain-related functional impairment in individuals with low back pain. The global interest in the instrument has been increasing, being validated in 17 countries1919 Monteiro J, Faísca L, Nunes O, Hipólito J. [Roland Morris disability questionnaire - adaptation and validation for the Portuguese speaking patients with back pain]. Acta Med Port. 2010;23(5):761-6. Portuguese..
The questionnaire consists of 24 dichotomous questions (yes or no), and the result corresponds to the sum of yes answers. This result can range from zero to 24, with zero indicating a person with “no limitations,” and 24 with “severe limitations”1919 Monteiro J, Faísca L, Nunes O, Hipólito J. [Roland Morris disability questionnaire - adaptation and validation for the Portuguese speaking patients with back pain]. Acta Med Port. 2010;23(5):761-6. Portuguese..
The Geriatric Depression Scale (GDS) is one of the most frequently used instruments for the detection of depressive symptoms in the elderly. Several studies have demonstrated that the GDS offers valid and reliable measures for the evaluation of depressive disorders. In addition, the use of the GDS short versions with 1, 4, 10, 15, and 20 questions (instead of the 30 questions of the original version) is increasing. The use of these short versions in clinical practice is even more attractive since the time spent with their application can be substantially reduced2020 Almeida OP, Almeida SA. [Reliability of the Brazilian version of the abbreviated form of Geriatric Depression Scale (GDS) short form]. Arq Neuropsiquiatr. 1999;57(2B):421-6. Portuguese..
This study used the 15-question scale. Score variations are considered: normal (from zero to 5), mild depression (6 to 10), and severe depression (11 to 15 points)2121 Ortiz BR, Wanderley KS. Reflexões sobre o uso da Escala de Depressão Geriátrica (GDS-15) em idosos hospitalizados. Rev Kairós Gerontol. 2013;16(3):307-16..
All the ethical precepts of Resolution No. 466/12 of the National Health Council on research with humans2222 Resolução 466/2012. Diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Conselho Nacional de Saúde. 2012. were respected.
The Research Ethics Committee approved the project with opinion number 711.592, and it is part of the activities of a Research Group in which the student and the advisor participate2323 Silveira MM, Pasqualotti A, Colussi EL, Vidmar MF, Wibelinger LM. Abordagem fisioterápica da dor lombar crônica no idoso. Rev Bras Ciên Saúde. 2011;8(25):56-61..
Statistical analysis
The data were input in a database in the Statistical Package for Social Sciences (SPSS) software for Windows for the descriptive analyses to characterize the profile of the elderly, the pain, the disabilities caused by the pain and their depressive symptoms. The Spearman´s correlation analysis was conducted to identify the relationship between pain intensity, disability generated by chronic LBP, and the number of depressive symptoms of the elderly.
RESULTS
The 46 senior citizens interviewed had family social support, another older adult living in the same house. This cutout was considered due to the importance of this type of support when studying variables with an affective component such as depression and pain perception. No senior person in this study lived alone, and all had an independent senior person to keep him company.
The sample was predominantly female (89.1%, n=41), white (78.3%, n=36), married (95.7%, n=44), retired (52.2%, n=24), catholic (63.0%, n=29), with low schooling (80.4% had the fourth grade of primary school, n=37, or a mean of 3.59 years of schooling - Md=4,00; SD=2.90, xmin = 0.xmax =12) and with no health insurance (84.8%, n=39).
The mean age was 67.02 years (Md=65.00; SD=5.54, xmin=60, xmax=81). The elderly had 4.56 children (Md=4.00; SD=2.62, xmin=0. xmax=4) and monthly income of R$577,24 (Md=558.50; SD=841.67, xmin =0.xmax=4500.00). Value of the minimum wage in 2014: R$724,00.
Table 1 shows the proportions of the categorical variables of the participants.
The most frequent pain intensity perceived by the elderly was intense (43.5%, n=20), preceded by moderate pain (41.3%, n=19). Table 2 shows the distribution of the elderly according to the intensity of the perceived pain.
Distribution of the elderly according to the intensity of the perceived pain. São Carlos, 2014
Regarding the characterization of pain, the most frequent descriptors were: uncomfortable (93.5%, n=43), painful (91.3%, n=42) and persistent (76.1%, n=35). Table 3 shows the distribution of the elderly according to the characterization of pain.
Of the 46 seniors interviewed, only 2.2% (n=1) had signs of severe depression, 28.3% (n=13) had mild depression, and 69.5% (n=32) obtained a score considered normal. The mean total score obtained by the GDS was 4.37 (Md=4.00; SD=2.67, xmin=0.00, xmax=11.00). It is worthy to note that the three most frequently items presented were: 11 (Do you feel good to be alive?), 7 (Do you feel happy most of the time?) and 1 (Are you satisfied with your life?), related to happiness and satisfaction with life.
Table 4 shows the distribution of the elderly according to the perception of depression.
The mean score of disability (limitations) related to LBP in regions 30 and 31, obtained by means of the RMDQ, was 11.391 points (Md=10.500; SD=7.188, xmin=0.00, xmax=24.00). It is worth to note that the three most frequent items related to the interruption of basic tasks due to pain were: 15 - my appetite is not very good because of my pain (82.6%, n=38); 19 - because of pain I need the help of other people to get dressed (80.4%, n=37), and 20 - I stay seated most of the day because of my pain (76.1%, n=35) (Table 5).
Descriptive data of disability/limitation related to lower back pain in the elderly. São Carlos, 2014
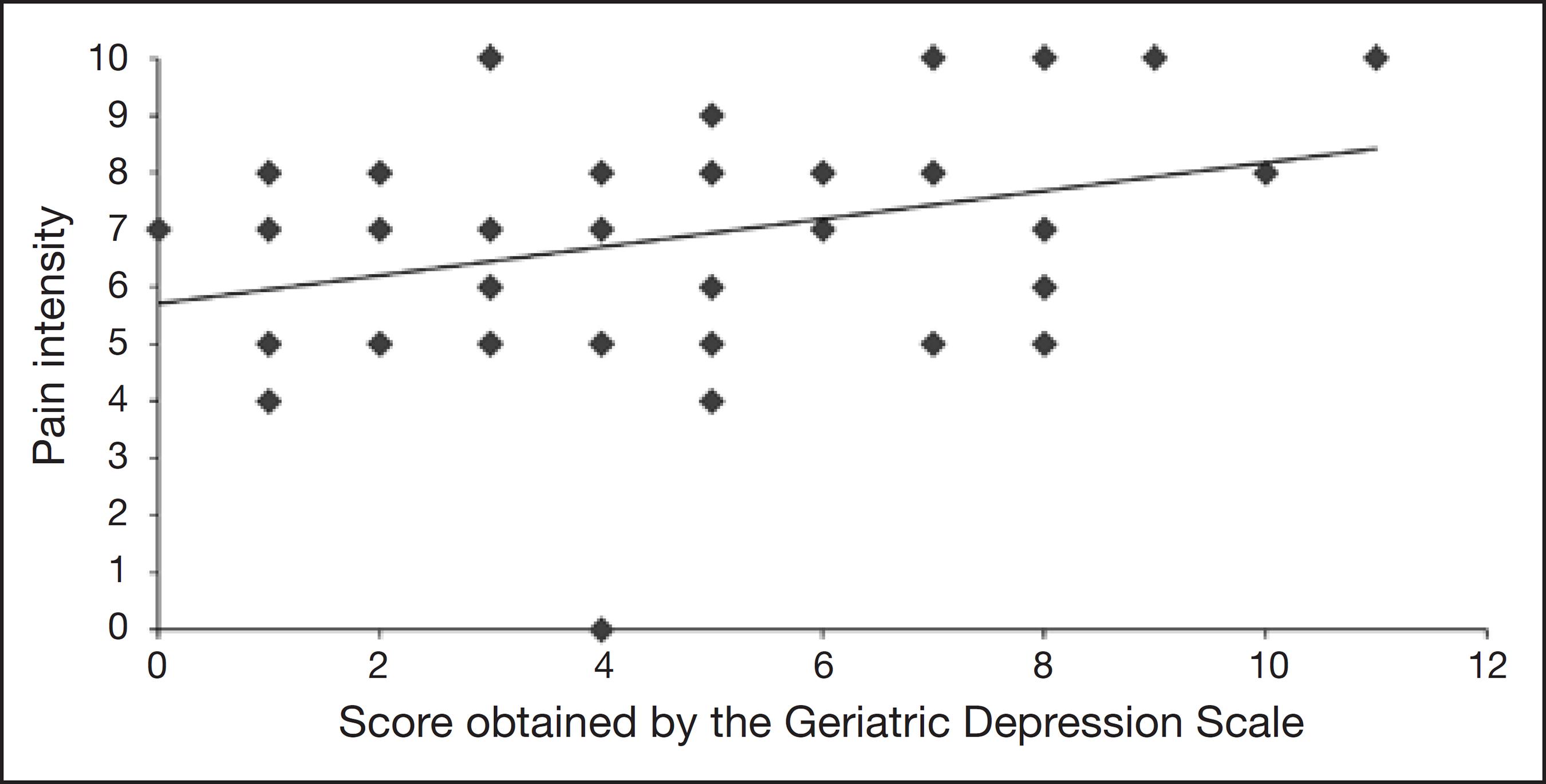
Correlational analyses showed that there is a significant and directly proportional relationship between the intensity of LBP and the number of depressive symptoms of weak magnitude (rho=0.302, p=0.041) (Figure 2).
Relationship between low back pain intensity and the number of depressive symptoms in the elderly
Correlational analyses showed that there is a significant and directly proportional relationship between the number of disabilities/limitations caused by LBP and the number of depressive symptoms of weak magnitude (rho=0.403, p=0.005) (Figure 3).
Relationship between the number of disabilities/limitations caused by low back pain and the number of depressive symptoms in the elderly
DISCUSSION
The female predominance in the sample was expected since the literature indicates that women tend to have a higher prevalence of pain when compared to men. Some authors assume that women have a higher predisposition to low back pain due to anatomic-functional particularities, such as shorter stature, low muscle mass; low bone density, joint fragility, and less adaptation to physical effort2323 Silveira MM, Pasqualotti A, Colussi EL, Vidmar MF, Wibelinger LM. Abordagem fisioterápica da dor lombar crônica no idoso. Rev Bras Ciên Saúde. 2011;8(25):56-61..
The meaning of pain can be influenced by cultural and social issues that eventually allow women to express or accept pain more openly while men are encouraged men to underestimate it2424 Zavarize SF, Wechsler SM. Perfil criativo e qualidade de vida: implicações em adultos e idosos com dor lombar crônica. Rev Bras Geriatr Gerontol. 2012;15(3):403-14..
Since the sample consisted of elderly with family social support in the figure of another elderly living in the same house, it was expected that the majority would be married. One can say that the profile of the elderly in the sample was typical of the literature: women under 75 years, married, with low income and little education. Recent studies on elderly assisted at FHU report this same profile2525 Poubel PB, Lemos EL, Araújo FC, Leite GG, Freitas IS, Silva RM, et al. Autopercepção de saúde e aspectos clínico-funcionais dos idosos atendidos em uma unidade básica de saúde no norte do Brasil. J Health Biol Sci. 2017;5(1):71-8.,2626 Ximenes MA, Vescovo RM, Manchini RF, Conti MH, Souza LC. Qualidade de vida dos idosos participantes do Projeto "Unidos da Melhor Idade" do Município de Fernão, SP, Brasil. Rev Kairós Gerontol. 2017;20(1):427-52..
The marked predominance of females is a consequence of male mortality, characterizing the feminization of aging. Low education, especially among women, is a reality since, in the past, female education focused on care and household chores2727 Alvarenga MR, Oliveira MA, Faccenda O. Sintomas depressivos em idosos: análise dos itens da Escala de Depressão Geriátrica. Acta Paul Enferm. 2012;25(4):497-503..
The predominant white ethnicity, retirement, and the Catholic religion are in line with the demographic data of the Brazilian elderly and literature characterization2828 Branco CO, Reis JF, Sarmento MS, Feitosa CD, Figueiredo ML, Sales JC. Elderly women assisted in primary healthcare: sociodemographic and economic analysis. Rev Enferm UFPI. 2017;6(2):44-50.,2929 Nunes MG, Leal MC, Marques AP, Mendonça SS. Idosos longevos: avaliação da qualidade de vida no domínio da espiritualidade, da religiosidade e de crenças pessoais. Saúde Debate. 2017;41(115):1102-15.. According to data from the Brazilian Institute of Geography and Statistics (IBGE) and the National Household Sample Survey (PNAD), in 2015, most Brazilians (45.22%) self-reported as white and among the elderly, 75.6% were retirees and/or pensioners11 Closs VE, Schwanke CH. A evolução do índice de envelhecimento no Brasil, nas suas regiões e unidades federativas no período de 1970 a 2010. Rev Bras Geriatr Gerontol. 2012;15(3):443-58..
Since the Catholic religion is prevalent in Brazil3030 Fernandes S. Interpretações Sobre o Censo da Igreja Católica e a Mudança. Rev Interd em Cult e Soc (RICS), São Luís. 2015;1(1)185-202., the sample was aligned with this data, and 97.80% of the elderly claimed to have a religion, a fact pointed out as positive in the literature. According to Nunes et al.2929 Nunes MG, Leal MC, Marques AP, Mendonça SS. Idosos longevos: avaliação da qualidade de vida no domínio da espiritualidade, da religiosidade e de crenças pessoais. Saúde Debate. 2017;41(115):1102-15., there is a relationship between religiosity, well-being, and quality of life. A systematic review conducted by Amorim et al.3131 Amorim DN, Silveira CM, Alves VP, Faleiros VP, Vilaça KH. Associação da religiosidade com a capacidade funcional em idosos: uma revisão sistemática. Rev Bras Geriatr Gerontol. 2017;20(5):721-35. shows that religiosity is significantly and positively associated with the functional capacity of the elderly.
The fact of not having health insurance, added to the income considered insufficient, reaffirm the importance of the Unified Health System, especially the primary care for the elderly with LBP complaints that need continuous monitoring3232 de Sousa Mata M, da Costa FA, de Souza TO, de Sousa Mata AN, Pontes JF. [Pain and functionality in primary health care]. Cien Saude Colet. 2011;16(1):221-30. Portuguese.,3333 Martinez JE, Macedo AC, Pinheiro DF, Novato FC, Jorge CM, Teixeira DT. Perfil clínico e demográfico dos pacientes com dor musculoesquelética crônica acompanhados nos três níveis de atendimento de saúde de Sorocaba. Acta Fisiátr. 2004;11(2):67-71..
Most of the elderly perceived their pain as intense or moderate. Data from the Health, Well-being and Aging study (SABE), which aimed to identify the living and health conditions of older adults living in Latin America and the Caribbean, showed similar results for elderly with chronic pain, 45.8% reported moderate pain and 27.55% severe pain1212 Dellaroza MS, Pimenta CA, Lebrão ML, Duarte YA. [Association of chronic pain with the use of health care services by older adults in Sao Paulo]. Rev Saude Publica. 2013;47(5):914-22. Portuguese..
It is well known that chronic LBP can lead to deficiencies in both functional performance and physical capacity, mainly restricting occupational and leisure activities, and undermining the independence of the elderly to perform their daily activities2323 Silveira MM, Pasqualotti A, Colussi EL, Vidmar MF, Wibelinger LM. Abordagem fisioterápica da dor lombar crônica no idoso. Rev Bras Ciên Saúde. 2011;8(25):56-61.. As the sample consisted entirely of older adults with LBP, a high prevalence of unbearable and severe pain was expected. However, the results showed that severe pain preceded by moderate pain was the most prevalent.
Few studies using EMADOR descriptors were found, which made it difficult to compare the data. In this study, the elderly classified the pain mainly as uncomfortable (93.5%), painful (91.3%) and persistent (76.1%)3434 Pelegrin AK, Moura Siqueira HB, Garbi MO, Saltareli S, Sousa FF. Evaluation and measurement of pain in the aging process. Psychol Neurosci. 2014;7(3):349-54., and 46 elderly residents in long-term care institutions were evaluated and classified the pain was severe (30.43%) with the most cited descriptor being “painful”.
Of the 46 seniors interviewed, only 2.2% had signs of severe depression, 28.3% had mild depression, and 69.5% had a score considered normal. The literature highlights the association of depressive symptoms with sociodemographic variables, indicating that social inequalities influence the living and health conditions and can contribute to the onset of these symptoms. Low education, age, and economic loss were the sociodemographic variables associated with depressive symptoms3535 Borges LJ, Benedetti TR, Xavier AJ, d'Orsi E. Associated factors of depressive symptoms in the elderly: EpiFloripa study. Rev Saude Publica. 2013;47(4):701-10. English, Portuguese.. Individuals with little education have a higher risk for depressive symptoms, indicating that high educational level is a protective factor. The educational level enables the individual to expand coping resources to stressful situations in life3535 Borges LJ, Benedetti TR, Xavier AJ, d'Orsi E. Associated factors of depressive symptoms in the elderly: EpiFloripa study. Rev Saude Publica. 2013;47(4):701-10. English, Portuguese..
In older individuals, there is a decrease in physical conditions, especially in those with spinal problems. Also, studies show that individuals over 60 years complain twice as much than individuals under 602424 Zavarize SF, Wechsler SM. Perfil criativo e qualidade de vida: implicações em adultos e idosos com dor lombar crônica. Rev Bras Geriatr Gerontol. 2012;15(3):403-14..
LBP is a very common problem. A study conducted in the Netherlands reported for sciatica an incidence of 11.6 per 1,000 people per year, and its occurrence is associated with age, physical fitness, smoking, overweight and back and abdominal muscle strength, psychological factors such as depression, occupational and psychosocial factors3636 Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81(9):646-56.. Another study with the purpose of analyzing the relationship between the presence and severity of depression and low back pain in the general population in Korea found that the prevalence of depression is significantly higher in Koreans with low back pain compared to individuals with no low back pain (20.3 and 4.5%, respectively) and that this type of pain can be considered a risk factor for depression3737 Park SM, Kim HJ, Jang S, Kim H, Chang BS, Lee C, et al. Depression is closely associated with chronic low back pain in patients over 50 years of age: a cross-sectional study using the Sixth Korea National Health and Nutrition Examination Survey (KNHANES VI-2). Spine. 2018;43(18):1281-8..
Regarding disabilities/limitations related to LBP, 82.6% of the elderly reported loss of appetite due to pain; 80.4% said that due to the pain they need the help of others to get dressed, and finally; 76.1% remain seated most of the time because of the pain. However, it was concluded that pain directly affects the life of the individual, and its intensity can make it difficult to perform daily activities and may lead to functional disability and depression1313 de Figueiredo VF, Pereira LS, Ferreira PH, Pereira AM, de Amorim JS. Incapacidade funcional, sintomas depressivos e dor lombar em idosos. Fisioter Mov. 2013;26(3):549-57.. Another study conducted with a heterogeneous sample with a mean age of 59.1 years showed that individuals with nonspecific LBP have a higher risk for disability with aging3838 Wettstein M, Eich W, Bieber C, Tesarz J. Pain intensity, disability, and quality of life in patients with chronic low Back pain: does age matter? Pain Med. 2018;20(3):464-75..
A meta-analysis carried out in 2004 aimed to identify the epidemiology of pain in depression. About 75% of the depressed individuals who constituted the samples complained of painful physical symptoms such as headache, epigastric, neck and back pain, and reported the presence of non-specific generalized pain. However, the presence of pain symptoms was more severe for depression outcomes3939 Lépine JP, Briley M. The epidemiology of pain in depression. Human Psychopharmacol. 2004;19(Suppl1):S3-7..
Studies that evaluated LBP-related disability through the RMDQ were not specific for the evaluation of the elderly population and showed lower disability scores. Nogueira and Navega4040 Nogueira HC, Navega MT. Influência da Escola de Postura na qualidade de vida, capacidade funcional, intensidade de dor e flexibilidade de trabalhadores administrativos. Fisioter Pesqui. 2011;18(4):353-8. evaluated 31 administrative workers with a mean age of 31.81±8.33 years and found that the disability scores were 1.06±1.65 points. Other authors, when studying individuals with nonspecific chronic LBP, aged between 18 and 75 years, showed disability indices of 7.77±5.5 points4141 Bento AA, Paiva AC, Siqueira FB. Correlação entre incapacidade, dor - Roland Morris, e capacidade funcional - SF-36 em indivíduos com dor lombar crônica não específica. E-scientia. 2009;2(1):1-18.. One study analyzed medical records of 244 patients with chronic low back pain with a mean age of 46.8±11.90 years, ranging from 18 to 73 years of age, and disability rates were 6.9±3.94242 Trivedi MH. The link between depression and physical symptoms. Prim Care Companion J Clin Psychiatry. 2004;6(Suppl1):12-6.. Since the disability scores of this research were significantly higher (M=11.39 points; SD=7.19), one can infer the burden of LBP on the elderly4343 Tsukimoto GR, Riberto M, Brito CA, Battistella LR. Avaliação longitudinal da Escola de Postura para dor lombar crônica através da aplicação dos questionários Roland Morris e Short Form Health Survey (SF-36). Acta Fisiátr. 2006;13(2):63-9..
The significant and directly proportional relationship between LBP, the number of disabilities/limitations caused, and the number of depressive symptoms corroborates the existence of a depression model in the elderly related to pain. Senior people who were not depressed before the condition started to present depressive symptoms due to chronic pain. In some cases, a bad/very bad report about one’s own health can be understood as a depressive symptom. Depression is an important marker of disability in the elderly since it affects the overall health and, consequently, the functional capacity3535 Borges LJ, Benedetti TR, Xavier AJ, d'Orsi E. Associated factors of depressive symptoms in the elderly: EpiFloripa study. Rev Saude Publica. 2013;47(4):701-10. English, Portuguese..
In turn, emotional components involved in the chronic pain process can, sometimes, be more significantly expressed than the sensory components. Emotions and symbolic values influence the perception of pain, nulling the proportionality between painful stimulus and pain perceived by the individual. Depression, anxiety, and stress, associated with changes in muscle tone and hormonal factors, lead to fatigue and, consequently, increased pain. This justifies the importance of investigating, beyond the merely physical and objective issues, the individual’s emotional aspects, and personality characteristics2424 Zavarize SF, Wechsler SM. Perfil criativo e qualidade de vida: implicações em adultos e idosos com dor lombar crônica. Rev Bras Geriatr Gerontol. 2012;15(3):403-14..
According to Trivedi4242 Trivedi MH. The link between depression and physical symptoms. Prim Care Companion J Clin Psychiatry. 2004;6(Suppl1):12-6. depression and pain share the same neurochemical pathway mediated by the serotonin and norepinephrine neurotransmitters, indicating that depression and painful physical symptoms should be treated together. The author, however, does not recommend a single approach that may result in incomplete remission and poor prognosis. It is necessary to choose effective interventions to promote the elimination of painful physical symptoms associated with depression to ensure the remission and return to full functioning.
Therefore, the family attention, the source of the main support network, and of qualified professionals in the process of monitoring chronic pain is extremely important, since the study shows a relationship between this variable and depression. Factors that, when not given proper attention, can affect the quality of life and even trigger other factors in a downward spiral.
In-depth studies on the subject would allow better rationalization of the therapeutic measures and the elaboration of strategies to prevent and control pain. Life extension maintaining functional capacity reduces healthcare costs and decreases the use of hospital and home care services4444 Braga IB, Santana RC, Ferreira DM. Depressão no idoso. Rev Multisciplinar Psicol. 2015;9(26):142-51..
This research did not allow generalizations and general extrapolations due to some methodological limitations. This is an ad hoc experience, with the participation of senior people of a single city in the interior of the state of São Paulo, specifically treated at the FHUs. The relatively small number of participants was due to the strictness of the inclusion and exclusion criteria that ensure bias minimization but reduce the sample size. It would be interesting to contemplate the senior citizens of the general community in sound samples and comparative analyses, in addition to the correlational ones presented. Moreover, the nonspecificity of the LBP needs to be considered, and future studies could address low back pain with specific pathological origins.
CONCLUSION
There was a significant and directly proportional relationship between the intensity of chronic low back pain and the number of depressive symptoms. Accordingly, there is also a significant relationship between the number of disabilities/limitations caused by pain and depressive symptoms.
Most of the elderly describe LBP as persistent, uncomfortable, and painful. The results indicate that higher pain intensities negatively affect the appetite, interpersonal relationships, and mobility.
REFERENCES
-
1Closs VE, Schwanke CH. A evolução do índice de envelhecimento no Brasil, nas suas regiões e unidades federativas no período de 1970 a 2010. Rev Bras Geriatr Gerontol. 2012;15(3):443-58.
-
2Santos CT. Envelhecimento no Brasil: da formulação de políticas à estruturação de serviços de saúde integrais. Tempus, Actas de Saúde Colet. 2014;8(1):65-70.
-
3Leandro LA, Teive HA. Fatores associados ao desempenho funcional de idosos portadores da doença de Parkinson. Rev Kairós Gerontol. 2017;20(2):161-78.
-
4Vilela ALS. Manual prático de Geriatria. 2ª ed. Rio de Janeiro: Guanabara-Koogan; 2017. 57-76p.
-
5World Health Organization. Dementia [acesso em 8 maio de 2019] disponível em: http://www.who.int/mediacentre/factsheets/fs362/en/;2016
» http://www.who.int/mediacentre/factsheets/fs362/en/;2016 -
6Alexopoulos GS, Abrams RC, Young RC, Shamoian CA. Cornell Scale for Depression in Dementia. Biol Psychiatry. 1988;23(3):271-84.
-
7Lawrence V, Murray J, Banerjee S, Turner S, Sangha K, Byng R, et al. Concepts and causation of depression: a cross-cultural study of the beliefs of older adults. Gerontologist. 2006;46(1):23-32.
-
8Engmann B. Mild cognitive impairment in the elderly: a review of the influence of depression, possible other core symptoms, and diagnostic findings. GeroPsych: J Gerontopsychol Geriatr Psychiatry. 2011;24(2):71-6.
-
9Hayde L. Examining the Association of Intergenerational Relationships and Living Arrangement on Depression Prevalence in Home Health and Hospice Patients Age 65 and Older. Thesis, Georgia: State University; 2019.
-
10Gomes JC, Teixeira MJ. Dor no idoso. Rev Bras Med. 2007;63(11):45-54.
-
11Merskey H, Bogduk N. Classification of chronic pain: descriptions of chronic pain syndromes and definitions of pain terms. IASP Pain Terminology. 1994. 240p.
-
12Dellaroza MS, Pimenta CA, Lebrão ML, Duarte YA. [Association of chronic pain with the use of health care services by older adults in Sao Paulo]. Rev Saude Publica. 2013;47(5):914-22. Portuguese.
-
13de Figueiredo VF, Pereira LS, Ferreira PH, Pereira AM, de Amorim JS. Incapacidade funcional, sintomas depressivos e dor lombar em idosos. Fisioter Mov. 2013;26(3):549-57.
-
14Pinheiro RC, Uchida RR, Mathias LA, Perez MV, Cordeiro Q. Prevalência de sintomas depressivos e ansiosos em pacientes com dor crônica. J Bras Psiquiatr. 2014;63(3):213-9.
-
15Bottega FH, Fontana RT. Pain as the fifth vital sign: use of the assessment scale by nurses in general hospital. Texto Contexto Enferm. 2010;19(2):283-90.
-
16Demografia e Saúde. Atlas do Desenvolvimento Humano no Brasil (Org.) [acesso em 25 janeiro de 2019] disponível em: (http://www.atlasbrasil.org.br/2013/).
» http://www.atlasbrasil.org.br/2013/ -
17Dados da Cidade. Prefeitura Municipal de São Carlos. [acesso em 30 novembro de 2018] disponível em: http://www.saocarlos.sp.gov.br/
» http://www.saocarlos.sp.gov.br/ -
18Sousa FF, Pereira LV, Cardoso R, Hortense P. Escala multidimensional de avaliação de dor (EMADOR). Rev Latino-Am Enfermagem. 2010;18(1):3-10.
-
19Monteiro J, Faísca L, Nunes O, Hipólito J. [Roland Morris disability questionnaire - adaptation and validation for the Portuguese speaking patients with back pain]. Acta Med Port. 2010;23(5):761-6. Portuguese.
-
20Almeida OP, Almeida SA. [Reliability of the Brazilian version of the abbreviated form of Geriatric Depression Scale (GDS) short form]. Arq Neuropsiquiatr. 1999;57(2B):421-6. Portuguese.
-
21Ortiz BR, Wanderley KS. Reflexões sobre o uso da Escala de Depressão Geriátrica (GDS-15) em idosos hospitalizados. Rev Kairós Gerontol. 2013;16(3):307-16.
-
22Resolução 466/2012. Diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Conselho Nacional de Saúde. 2012.
-
23Silveira MM, Pasqualotti A, Colussi EL, Vidmar MF, Wibelinger LM. Abordagem fisioterápica da dor lombar crônica no idoso. Rev Bras Ciên Saúde. 2011;8(25):56-61.
-
24Zavarize SF, Wechsler SM. Perfil criativo e qualidade de vida: implicações em adultos e idosos com dor lombar crônica. Rev Bras Geriatr Gerontol. 2012;15(3):403-14.
-
25Poubel PB, Lemos EL, Araújo FC, Leite GG, Freitas IS, Silva RM, et al. Autopercepção de saúde e aspectos clínico-funcionais dos idosos atendidos em uma unidade básica de saúde no norte do Brasil. J Health Biol Sci. 2017;5(1):71-8.
-
26Ximenes MA, Vescovo RM, Manchini RF, Conti MH, Souza LC. Qualidade de vida dos idosos participantes do Projeto "Unidos da Melhor Idade" do Município de Fernão, SP, Brasil. Rev Kairós Gerontol. 2017;20(1):427-52.
-
27Alvarenga MR, Oliveira MA, Faccenda O. Sintomas depressivos em idosos: análise dos itens da Escala de Depressão Geriátrica. Acta Paul Enferm. 2012;25(4):497-503.
-
28Branco CO, Reis JF, Sarmento MS, Feitosa CD, Figueiredo ML, Sales JC. Elderly women assisted in primary healthcare: sociodemographic and economic analysis. Rev Enferm UFPI. 2017;6(2):44-50.
-
29Nunes MG, Leal MC, Marques AP, Mendonça SS. Idosos longevos: avaliação da qualidade de vida no domínio da espiritualidade, da religiosidade e de crenças pessoais. Saúde Debate. 2017;41(115):1102-15.
-
30Fernandes S. Interpretações Sobre o Censo da Igreja Católica e a Mudança. Rev Interd em Cult e Soc (RICS), São Luís. 2015;1(1)185-202.
-
31Amorim DN, Silveira CM, Alves VP, Faleiros VP, Vilaça KH. Associação da religiosidade com a capacidade funcional em idosos: uma revisão sistemática. Rev Bras Geriatr Gerontol. 2017;20(5):721-35.
-
32de Sousa Mata M, da Costa FA, de Souza TO, de Sousa Mata AN, Pontes JF. [Pain and functionality in primary health care]. Cien Saude Colet. 2011;16(1):221-30. Portuguese.
-
33Martinez JE, Macedo AC, Pinheiro DF, Novato FC, Jorge CM, Teixeira DT. Perfil clínico e demográfico dos pacientes com dor musculoesquelética crônica acompanhados nos três níveis de atendimento de saúde de Sorocaba. Acta Fisiátr. 2004;11(2):67-71.
-
34Pelegrin AK, Moura Siqueira HB, Garbi MO, Saltareli S, Sousa FF. Evaluation and measurement of pain in the aging process. Psychol Neurosci. 2014;7(3):349-54.
-
35Borges LJ, Benedetti TR, Xavier AJ, d'Orsi E. Associated factors of depressive symptoms in the elderly: EpiFloripa study. Rev Saude Publica. 2013;47(4):701-10. English, Portuguese.
-
36Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81(9):646-56.
-
37Park SM, Kim HJ, Jang S, Kim H, Chang BS, Lee C, et al. Depression is closely associated with chronic low back pain in patients over 50 years of age: a cross-sectional study using the Sixth Korea National Health and Nutrition Examination Survey (KNHANES VI-2). Spine. 2018;43(18):1281-8.
-
38Wettstein M, Eich W, Bieber C, Tesarz J. Pain intensity, disability, and quality of life in patients with chronic low Back pain: does age matter? Pain Med. 2018;20(3):464-75.
-
39Lépine JP, Briley M. The epidemiology of pain in depression. Human Psychopharmacol. 2004;19(Suppl1):S3-7.
-
40Nogueira HC, Navega MT. Influência da Escola de Postura na qualidade de vida, capacidade funcional, intensidade de dor e flexibilidade de trabalhadores administrativos. Fisioter Pesqui. 2011;18(4):353-8.
-
41Bento AA, Paiva AC, Siqueira FB. Correlação entre incapacidade, dor - Roland Morris, e capacidade funcional - SF-36 em indivíduos com dor lombar crônica não específica. E-scientia. 2009;2(1):1-18.
-
42Trivedi MH. The link between depression and physical symptoms. Prim Care Companion J Clin Psychiatry. 2004;6(Suppl1):12-6.
-
43Tsukimoto GR, Riberto M, Brito CA, Battistella LR. Avaliação longitudinal da Escola de Postura para dor lombar crônica através da aplicação dos questionários Roland Morris e Short Form Health Survey (SF-36). Acta Fisiátr. 2006;13(2):63-9.
-
44Braga IB, Santana RC, Ferreira DM. Depressão no idoso. Rev Multisciplinar Psicol. 2015;9(26):142-51.
Publication Dates
-
Publication in this collection
23 Sept 2019 -
Date of issue
Jul-Sep 2019
History
-
Received
08 Feb 2019 -
Accepted
21 May 2019