Abstracts
We report a patient admitted to our hospital with aortic valve rupture due to blunt chest trauma. The aortic rupture was accurately identified by the transesophageal echocardiogram, allowing a better surgical approach.
Relatamos o caso de paciente internado em nossa instituição com ruptura da válvula coronariana direita da valva aórtica, secundária a trauma torácico fechado. O ecocardiograma transesofágico identificou o local da ruptura, permitindo melhor planejamento cirúrgico.
Insuficiência valvar aórtica; trauma torácico fechado; ecocardiograma transesofágico
CASE REPORT
A case of aortic valve rupture due to blunt chest trauma
José Eduardo Theodoro; Maria do Socorro Alves Oliveira; Henry Abensur; Gustavo Chiarello; Raphael Azevedo Barreto; Januário Manuel de Souza; Sérgio Almeida de Oliveira
Hospital São Joaquim da Real e Benemérita Beneficência Portuguesa de São Paulo, São Paulo, SP, Brazil
Mailing Address Mailing Address: José Eduardo Theodoro Rua Vitório Zague, 30 13171-550 São Paulo, SP, Brazil E-mail: theodoro@cardiol.br
ABSTRACT
We report a patient admitted to our hospital with aortic valve rupture due to blunt chest trauma. The aortic rupture was accurately identified by the transesophageal echocardiogram, allowing a better surgical approach.
Key words: Aortica valve regurgitation, blunt chest trauma, transesophageal echocardiogram.
Aortic valve regurgitation due to cusp rupture is a rare complication of blunt chest trauma, and one of the first reports in literature is that by Penderleath, in 18301. We present a case of laceration of the right coronary cusp of the aortic valve that resulted from a 12-meter fall during climbing practice.
Transesophageal echocardiogram accurately showed the lacerated cusp, allowing the patient to receive the best treatment.
Case Report
In March 2005, a 25-year-old male patient was admitted to our institution with a history of a 12-meter fall that had taken place in December 2005, during mountain climbing. At the time of the fall, he was admitted to another hospital due to a fracture in the right humerus and slight spinal column trauma. During the hospital stay, a cardiac murmur was detected and a thoracic echocardiogram was performed, demonstrating the presence of aortic reflux, which prompted his referral to our institution.
At admission, the patient was eupneic, oriented, afebrile; blood pressure was 150 x 60 mmHg, radial pulse was 62 bpm with ample pulses, palpable ictus in the fifth left intercostal space with increased amplitude, diastolic murmur audible in the left sternum border, vesicular murmur present and symmetrical without adventitious sounds, flaccid abdomen that was painless to palpation and lower limbs without edema, with free calves.
The electrocardiogram showed sinusal rhythm, with a cardiac frequency of 60 bpm, QRS axis at +90º, within the range of normality. The plain chest radiography showed that the cardiac area was within the maximum limit of normality, with normal pulmonary vascularity.
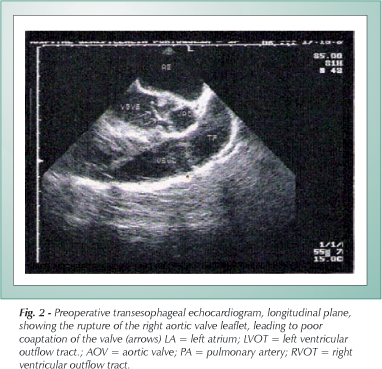
The bidimensional Doppler echocardiogram showed a left ventricle diastolic diameter of 58 mm and systolic diameter of 38 mm, with an ejection fraction by M-mode cube method of 71% with a shortening percentage of 34%. The atriums and the right ventricle were normal. The Doppler showed a moderate to significant aortic valve reflux and minimal mitral valve reflux. The pericardium was normal. The transesophageal echocardiogram showed an abnormal movement of the right coronary cusp with leaflet rupture, leading to poor coaptation and causing moderate to significant valve failure (Figs. 1 and 2).
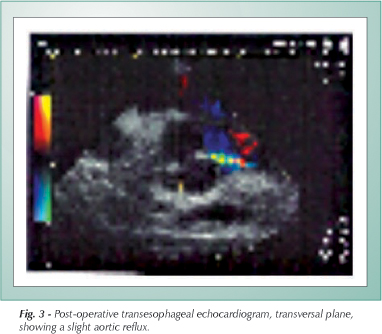
The patient underwent surgery on the following day, being submitted to right cusp-plasty, under deep hypothermic total circulatory arrest for 14 minutes; a slight aortic reflux shown by the intra-operative transesophageal echocardiogram persisted (Fig. 3).
The bidimensional control echocardiogram performed on the day after the surgery confirmed the slight aortic valve reflux (Fig. 4).
The post-operative evolution was considered good and complication-free, with decrease of the parasternal murmur and normalization of the peripheral pulses and arterial pressure, and the patient was discharged on the sixth day post-surgery.
Discussion
Cardiac valve injuries due to blunt chest trauma are rare; however, when they do occur, they pose a high risk for the patient2. Necropsy studies have demonstrated that, in cases of blunt chest trauma that died, less than 5% of the patients presented this finding2. Among the affected valves, the most common one is the aorta, alone or in association with myocardial contusion, atrial septum rupture, aortic rupture or rupture of the common carotid artery2. The most commonly observed injury in blunt chest trauma is myocardial contusion3. The right ventricle is the cardiac chamber that most commonly presents rupture, and the coronary artery rupture is unusual.
Aortic ruptures are more commonly observed, and are more often located in the isthmus, where the mobile thoracic aorta joins the more fixed portion of the remaining aortic arch. Fifteen to 20% of car accident victims present aortic rupture due to such mechanism.
Aortic valve failure caused by chest trauma has two main reasons: due to a sudden increase in the intrathoracic pressure during diastole, when the pressure gradient in the aortic valve is at the maximum and the valve is closed3; or when the sub-adventitial rupture of the ascending aorta causes the prolapse of the corresponding valve cusp4.
The clinical picture of acute aortic regurgitation usually deteriorates very fast, and the diagnosis of aortic valve rupture must be promptly achieved4. Chest pain and dyspnea associated to a new diastolic murmur are the most common symptoms, and are highly suggestive of the presence of the injury5. These injuries are usually associated to multiple chest injuries (rib fractures, sternum fractures, pulmonary contusion), which makes the valve injury diagnosis and treatment a challenge.
Several reports have stressed the importance of the echocardiogram in detecting a valve injury caused by chest trauma6-11. Every patient with no previous history of cardiac disease that presents cardiac murmur after chest trauma is strongly suspected of presenting aortic valve injury12, and must be submitted to an echocardiogram. When the diagnosis is confirmed, the surgical exploration of the valve is necessary.
In the present case, the patient had a fracture in the right humerus, but no thoracic injury; he presented an isolate occurrence of aortic valve rupture, which is rare in literature.
The patient's subacute evolution is also noteworthy, which allowed the surgical repair to be carried out three months after the accident.
Finally, we emphasize the importance of the echocardiogram, especially the transesophageal one, as a diagnostic means to direct the surgical approach, to be performed during surgery, and in the postoperative period, for adequate patient's follow-up.
References
Manuscript received December 3, 2005; revised manuscript December 8, 2005; accepted December 8, 2005.
- 1. Penderleath D. Case of death from rupture of one the semilunar valves of the aorta. London Medical Gazette. 1830; 7: 109.
- 2. Vidmar J, Brilej D, Voga G, et al. Aortic valve insufficiency due to rupture of the cusp in a patient with multiple trauma. Unfallchirurg. 2003; 106(6): 514-8.
- 3. Unal M, Demirsoy E, Gogus A, et al. Acute aortic valve regurgitation secondary to blunt chest trauma. Tex Heart Inst J. 2001; 28(4): 312-4.
- 4. Obadia JF, Tatou E, David M, et al. Aortic valve regurgitation caused by blunt chest injury. Br Heart J. 1995; 74(5): 545-7.
- 5. Ten Berg JM, Jaarsma W, Hamerlynck RP, et al. Rupture of the left coronary cusp of the aortic valve caused by blunt chest trauma: early diagnosis by transesophageal echocardiography. J Am Soc Echocardiogr. 1995; 8(5 Pt 1): 766-9.
- 6. Iryama T, Sugimura S, Hattori Y, et al. A case of aortic valve rupture due to blunt chest trauma. Kyoboku Geka. 1995; 48(13): 1118-21.
- 7. Pearson GD, Trachiotis GD, Midgley FM, et al. A retrospective review of the role of transeophageal echocardiography in aortic and cardiac trauma in a level I Pediatric Trauma Center. J Am Soc Echocardiogr. 1997;10(9): 946-55.
- 8. Ussia GP, Rapezzi C, Ferlito M, et al. Valvular lesions in the course of nonpenetrating thoracic trauma: their diagnosis by transesophageal echocardiography. Cardiologia. 1996; 41 (11): 1107-11.
- 9. Gay JA, Gottdiener JS, Gomes MN, et al. Echocardiography features of traumatic disruption of the aortic valve. Chest. 1983; 83(1): 150-1.
- 10. McIlduff JB, Foster ED. Disruption of a normal aortic valve as a result of blunt chest trauma. J Trauma. 1978; 18(5): 373-5.
- 11. Reiland-Smith J, Weintraub RM, Sellke FW, et al. Traumatic aortic valve injury sustained despite the deployment of an automobile air bag. J Chest .1993; 103(5): 1603.
- 12. Chi S, Blair TC, Gonzalez-Lavin L. Rupture of normal aortic valve after blunt chest trauma. Thorax .1977; 32(5): 619-22.

Publication Dates
-
Publication in this collection
06 Mar 2007 -
Date of issue
Nov 2006
History
-
Accepted
08 Dec 2005 -
Reviewed
08 Dec 2005 -
Received
03 Dec 2005