Abstracts
BACKGROUND: Calculations of metabolic and physical activity are carried out from the active tissue in the body, known as lean body mass, which is the sum of fat-free lean mass to essential fat. Kinesiotherapy helps in weight strength and flexibility and can be applied in the patients recovery. AIM: In patients undergoing surgical treatment for morbid obesity are the objectives: 1) to evaluate the effect of physiotherapy counter resisted in lean mass; 2) to assess the factors associated with variations in lean body mass with physical therapy; 3) to compare the group of patients who lost lean mass to the one who won using physical therapy, analyzing the co-morbidities that interfered with these results. METHOD: The study included 100 patients operated on by Fobi-Capella technique divided into group A, patients who lost lean body mass measured in two periods (between 30 days and three months between three months and six months) and group B by the patients that gained lean body mass in at least period. Data collection was performed using the Electronic Multiprofessional Protocol of Metabolic and Bariatric Surgery with emphasis in Physical Therapy, identified as SINPE© (Integrated Electronic Protocols). The patients were evaluated pre-operatively and followed in the postoperative period in four phases: in the hospital, 30 days, three months and six months after the operation. RESULTS: There were significant differences between the three assessments (p <0.001). By comparing the 30 days to three months, there was loss of lean body mass with statistical significance (p <0.001). Similarly, between 30 days and six months (p <0.001). However, the period between three months and six months did not show results with significance level (p <0.612), showing a tendency to maintain lean body mass. CONCLUSIONS: Physical therapy counter resisted helped in maintaining lean body mass between the periods of three months and six months; 2) elderly men, diabetic and dyslipidemic lost more lean mass; duration of obesity, cardiovascular and orthopedic disease not changed the lean mass; 3) groups A and B showed no significant differences for both gain and loss lean mass in relation to cardiovascular and orthopedic comorbidities, but patients with diabetes mellitus and dyslipidemia were more prevalent in Group A.
Physical therapy; Obesity; Eletronic protocols
RACIONAL: Cálculos metabólicos e de atividade física são realizados a partir do tecido ativo presente no corpo, conhecido como massa corporal magra, que resulta da soma da massa magra isenta de gordura com a gordura essencial. A cinesioterapia é a musculação terapêutica que auxilia na força e flexibilidade. OBJETIVOS: No paciente submetido a tratamento cirúrgico para obesidade mórbida: 1) avaliar o efeito da fisioterapia contra-resistida na massa magra; 2) avaliar os fatores associados às variações de massa corporal magra com tratamento fisioterapêutico; 3) comparar o grupo de pacientes que perdeu com o que ganhou massa magra com o tratamento fisioterapêutico, analisando as co-morbidades que interferiram para esses resultados. MÉTODO: Foram incluídos 100 pacientes operados pela técnica de Fobi-Capella, ou derivação em Y-de-Roux, sem anel e divididos em grupo A composto por pacientes que perderam massa corporal magra nos dois períodos avaliados (entre 30 dias e três meses e entre três meses e seis meses) e o grupo B pelos demais pacientes que apresentaram ganho de massa corporal magra em pelo menos um dos períodos avaliados. A coleta de dados foi realizada através do Protocolo Eletrônico Multiprofissional em Cirurgia Bariátrica e Metabólica com Ênfase em Fisioterapia, identificado pela siga SINPE© (Sistema Integrado de Protocolos Eletrônicos). Os pacientes realizaram avaliação fisioterapêutica pré-operatória e foram acompanhados no período pós-operatório em quatro fases: na internação hospitalar, submetidos à musculação terapêutica em 30 dias após a operação, aos três meses e aos seis meses do pós-operatório. RESULTADOS: Houve diferença significativa entre as três avaliações (p<0,001). Ao comparar a de 30 dias com três meses, foi observada perda de massa corporal magra com significância estatística (p<0,001). Da mesma forma, entre 30 dias e seis meses (p<0,001). Entretanto, o período entre três meses e seis meses não apresentou resultado com significância (p<0,612), demonstrando tendência à manutenção de massa corporal magra. CONCLUSÕES: A fisioterapia contra-resistida auxiliou na manutenção da massa corporal magra entre os períodos de três meses e seis meses; 2) homens idosos, diabéticos e dislipidêmicos perderam mais massa magra, sendo que o tempo de obesidade, doenças cardiovasculares e ortopédicas não interferiram nas variações de massa magra; 3) os grupos A e B não apresentaram diferenças significativas tanto para ganho como para perda em relação às doenças cardiovasculares e ortopédicas; porém, pacientes com diabete melito e dislipidemias encontravam-se mais no Grupo A.
Fisioterapia; Obesidade Morbida; Protocolos eletrônicos
ORIGINAL ARTICLE
Correspondence
ABSTRACT
BACKGROUND: Calculations of metabolic and physical activity are carried out from the active tissue in the body, known as lean body mass, which is the sum of fat-free lean mass to essential fat. Kinesiotherapy helps in weight strength and flexibility and can be applied in the patients recovery.
AIM: In patients undergoing surgical treatment for morbid obesity are the objectives: 1) to evaluate the effect of physiotherapy counter resisted in lean mass; 2) to assess the factors associated with variations in lean body mass with physical therapy; 3) to compare the group of patients who lost lean mass to the one who won using physical therapy, analyzing the co-morbidities that interfered with these results.
METHOD: The study included 100 patients operated on by Fobi-Capella technique divided into group A, patients who lost lean body mass measured in two periods (between 30 days and three months between three months and six months) and group B by the patients that gained lean body mass in at least period. Data collection was performed using the Electronic Multiprofessional Protocol of Metabolic and Bariatric Surgery with emphasis in Physical Therapy, identified as SINPE© (Integrated Electronic Protocols). The patients were evaluated pre-operatively and followed in the postoperative period in four phases: in the hospital, 30 days, three months and six months after the operation.
RESULTS: There were significant differences between the three assessments (p <0.001). By comparing the 30 days to three months, there was loss of lean body mass with statistical significance (p <0.001). Similarly, between 30 days and six months (p <0.001). However, the period between three months and six months did not show results with significance level (p <0.612), showing a tendency to maintain lean body mass.
CONCLUSIONS: Physical therapy counter resisted helped in maintaining lean body mass between the periods of three months and six months; 2) elderly men, diabetic and dyslipidemic lost more lean mass; duration of obesity, cardiovascular and orthopedic disease not changed the lean mass; 3) groups A and B showed no significant differences for both gain and loss lean mass in relation to cardiovascular and orthopedic comorbidities, but patients with diabetes mellitus and dyslipidemia were more prevalent in Group A.
Headings: Physical therapy. Obesity, morbid. Eletronic protocols.
INTRODUCTION
Obesity is a chronic and multifactorial situation, characterized by excessive accumulation of body fat. It causes serious damage to health of the individual with prevalence increasing levels of global epidemic. According to the Brazilian Institute of Geography and Statistics, Brazil has also reached alarming data showing that 40.6% of the 95.5 million people over age 20 have excess body mass of which 10.5 million of them already are considered obese14.
The treatments for obesity can be divided into two categories: clinical and surgical6,7. In more severe cases, the consequences of exposure to risk is higher, and because of the failure in clinical treatments, surgery has now been considered a good alternative for the treatment of high obesity7.
Because it is commonly associated with disease complications and especially by its outcome directly linked to the change of the patient's life, it is necessary that the preparation for the surgical procedure be performed by a multi professional team to be successful10.
Among the specialties that are part of a multidisciplinary team, physiotherapy is involved before surgery, in hospitalization, in early and late postoperative period. Its main objective is to reduce the chances of complications of cardiopulmonary, musculoskeletal and metabolic system. Physical therapy requires evaluations and reevaluations, according to the phase of surgical treatment, being the professionals involved advised the multidisciplinary use of the clinical data collected12.
As the definition of obesity refers to increased body fat percentage, the determination of the quantity, evaluation of the fat distribution and its relationship to other components of body composition, is essential for the treatment of obesity. The component of the most important body composition, which classifies him as overweight, is the percentage of fat. With this finding, the therapist can estimate the body component characterized as lean body mass (LBM), which is actually the active tissue that matters11.
Because there is close relationship between function and body composition, it is necessary that the patient be submitted to body fractionation, so that the result demonstrates the active tissue. Calculations of metabolic and physical activity are conducted from the active tissue in the body, known as MCM, which is the sum of lean mass to fat-free essential fat.
This analysis is also important to measure the energy consumption of the patient, since it can not exceed the limit that triggers protein cannibalization, ie, especially common in post-operative bariatric surgery.
There are two sets of body composition analysis indicated for the morbidly obese, in a practical and continuous control, ie, the Weltman protocol and tetrapolar multifrequency bioimpedance8.
The equation methods seem more suitable for anthropometric assessment of body composition in obese because they are less expensive, easy to use and independent of the level of body fat.
The basic guidelines for planning and implementing the different stages of physical exercise programs should be individual, through personal training, defining the methodology and objectives of its application12.
The phase indicated for early exercise, normally happens around 30 days after the operation and allows the therapist to begin to use effectively metabolic parameters of evaluations performed in the preoperative period. This period is considered outpatient, and also kinesthetic stimulation therapy can be performed at home13.
Action inherent in the professional role is to determine the maximum heart rate (Max HR) for this phase as a barrier to physical stimulation. To do so, with the patients using abdominal belt or not, is required to hold at least three sets of voluntary forced cough, under monitoring of heart rate. The value of Max HR achieved (by the pressure of airway occlusion or transdiaphragmatic) should not be exceeded by the physical exercise done.
The importance of this phase is to maintain the volume of physical activity that is capable of monitoring the nutritional demands imposed without compromising the patient's MCM. Thus, physiotherapists elected kinesiotherapy counter-resisted to be used. This methodology allows to calculate the value of the minimum energy expenditure of exercise, facilitating control of MCM construction2.
The physical therapist trained in this technique performs exercises with the application of functional patterns, with continuous monitoring of heart rate, not allowing the patient to have, during the session, frequency values below 60% Max HR. This value can be found by use of the Tanaka equation represented the following formula: Max HR = 208 - (0.7 x age) in beats per minute (bpm)9.
It is important to consider that at this stage of treatment, the practitioner has the upper heart rate limit the amount in occlusion pressure, heart rate and lower limit at 60% Max HR
After this phase, which can extend for up to six months depending on comorbidities, the therapist is able to refer the performance physical education with well-defined parameters.
The objectives of this study in patients after bariatric surgery were: 1) to evaluate the effect of physiotherapy counter resisted in total body mass, body mass index, fat body mass and maintenance of lean body mass; 2) to evaluate factors associated with variations in lean body mass with physical therapy; 3) to compare the group of patients who lost and won lean mass with physical therapy, analyzing the comorbid conditions that interfered with these results.
METHOD
The study included 100 patients operated on by Fobi-Capella technique or Roux-en-Y deviation without a ring, done at Metabolic and Bariatric Surgery Service of Evangelic University Hospital in Curitiba, PR and Our Lady of Rocio of Campo Largo, PR from December 2008 to July 2010. All included patients of both genders agreed to participate and signed a term of consent. The study protocol number 3382/9 was approved by the Research Ethics Committee of the Evangelic Society of Paraná.
Inclusion criteria were: a) BMI greater than or equal to 40 kg/m2 or > 35 kg/m2 with comorbidities, aged between 18 and 60 years; b) patients who received the assent of all multi professional team of professionals consisting of digestive surgeon, endocrinologist, endoscopist, cardiologist, pulmonologist, psychologist, nutritionist and physiotherapist; c) patients who had follow-up physical therapy in the postoperative period of 180 days, conducting counter-resisted kinesiotherapy (bodybuilding therapy ) three times a week.
Exclusion criteria were: a) patients who had severe pulmonary diseases; b) history of recurrent thromboembolism without clinical control; c) advanced cardiomyopathy; d) serum positive for HIV; e) active neoplasia; f) severe liver failure; g) drug addiction; h) severe psychiatric disorders; i)severe alcoholism.
Data collection was performed using the Electronic Multiprofessional Protocol for Metabolic and Bariatric Surgery with emphasis in physical therapy identified by SINPE (Integrated Electronic Protocol System) registered in the Brazilian National Industrial Property Institute (INPI) under number RS06056-1, with intellectual property of Dr. Osvaldo Malafaia16.
Patients underwent preoperative physical therapy evaluation and were followed in the postoperative period in four stages: hospitalization and at the beginning of physical therapy within 30 days, three months and six months after surgery.
For analysis and follow-up after surgery in relation to resisted counter-kinesiotherapy was as follows: preoperative physical therapy evaluation with values of resting heart rate using frequency meter Polar FT2 model; chest cirtometry held with a flexible tape graduated up to 150 cm. For analysis of fat percentage and analysis of the MCM was used Weltman's equation parameters and abdominal circumference measured with flexible tape. To obtain the total body mass and height, was used digital electronic scale (Filizola®), with a capacity of 300 kg, divided in 100 g, and anthropometer with a capacity of 1.90 m.
As physiotherapy treatment was elected bodybuilding therapy (kinesiotherapy counter-resisted). Physical therapists trained in the technique performed exercises with application of functional patterns, continuous monitoring of heart rate, not allowing the patient to present during the session values of heart rate below 60% HR max
For comparison of patients with MCM in the evolution of physical therapy two groups were defined according to the MCM assessments conducted after 30 days, three months and six months of operation. Group A consisted of patients who lost MCM evaluated in two periods (between 30 days and three months and between three and six months) and Group B, patients with MCM gain in at least one of the periods.
Statistical analysis
Was performed to compare the three evaluation periods (30 days, three months and six months) in relation to quantitative variables, was considered the model of analysis of variance with repeated measures. In case of rejection of hypothesis of equality in the three times they were compared two by two by considering the test LSD (least significant difference). To evaluate the association between quantitative variables was used Pearson correlation coefficient. To compare the two groups regarding quantitative variables was considered the Student's t test for independent samples. P values <0.05 were considered statistically significant. Data were analyzed with the computer program Statistica v.8.0.
RESULTS
The total body mass achieved a statistically significant reduction in all periods evaluated (p <0.001). By comparing the average total body mass in 30 days in the evaluation with the evaluation of three months was a significant difference (p <0.001) in patients undergoing physiotherapy counter resisted. Likewise, significant difference happened between 30 days and six months (p <0.001) and between three and six months (p <0.001) in patients undergoing physiotherapy counter resisted. Table 1 presents descriptive statistics of total body mass in each moment of assessment and of variations between assessments. It is observed that between 30 days and three months the average loss of total body mass was 12.4 ± 3.1 kg between 30 days and six months this loss was 24.0 ± 4.0 kg.
In periods, BMI was significantly decreased (p <0.001). There was a difference between the 30-day trial and three months (p <0.001), between the 30-day trial and six months (p <0.001) and between the assessment of three months and six months (p <0.001) in patients undergoing physiotherapy counter resisted. The average loss in BMI within 30 days to three months was 4.2 ± 1.0 kg / m2 and within 30 days to six months was 8.2 ± 1.3 kg / m2 (Table 2).
The fat body mass has decreased with significant values ?in all evaluated periods (p <0.001).?In the comparison of assessments three months and 30 days was a significant difference (p <0.001) in patients undergoing physiotherapy counter resisted.?Also in the comparisons between 30 days and six months and between three and six months, there was evidence of significant difference in mean fat mass (p <0.001) in both comparisons in patients undergoing physiotherapy counter resisted.?Table 3 presents descriptive statistics of body fat mass at each time of evaluation and the variations between these times.
The results of lean body mass analysis indicated that there is significant difference between the three assessments (p <0.001).?By comparing the 30-day trial with three months, there was loss of lean body mass with statistical significance (p <0.001).?Similarly, between 30 days and six months (p <0.001).?However, the period between three months and six months shows no significant results (p <0.612), showing a tendency to maintain MCM (Table 4).
In view of the research be directed to the action of physiotherapy, it was considered important to assess factors that may be associated with variations in lean body mass after surgery and during physical therapy treatment.?Thus, the focus in the following analysis has direct relation to lean body mass.
Initially, was assessed the gender, diabetes mellitus, dyslipidemia, cardiovascular and orthopedic diseases.?In this analysis, was compared the groups defined by ratings of the factors evaluated in relation to the means of variations in lean body mass between 30 days and three months, between three and six months and between 30 days and six months.?Next, was assessed the correlation of changes in LBM in the periods analyzed with age and the duration of obesity.?These correlations were also assessed lean body mass with the assessments of total body mass, body mass index and fat body mass before the operation.
Analyzing the sample, it was found that on average there was a loss of lean body mass both in males as in females, but there was greater decrease in men with a significant difference in the periods between 30 days and three months and between 30 days and six months .
In the analysis of patients with diabetes mellitus, was found that between three and six months, on average, subjects lost 1.8 kg of lean body mass, while those who had not gained an average of 1.5 kg ( p = 0.001).?There was no significant difference between diabetic and nondiabetic variations in lean body mass in the other two periods.
There was loss of lean body mass increased in patients with dyslipidemia compared to those without it, showing significant loss of lean body mass in three to six months.?Between 30 days and three months there was no difference between patients with and without dyslipidemia.?Already, between 30 days and six months, there is a tendency that individuals with it ??lose more lean body mass than without it.
Patients with cardiovascular disease presented loss of MCM in periods of three to six months and 30 days to six months, without significant difference compared to those without cardiovascular disease.?In periods of 30 days to three months there was greater loss of lean body mass in patients without them.
There was greater loss of lean body mass during periods of three months and six months in patients with orthopedic diseases without significant differences.?In periods of 30 days and six months tended to gain in LBM in patients who had no skeletal disease.
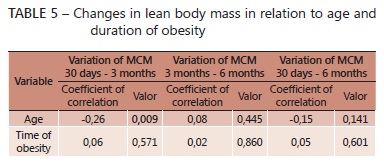
Regarding the quantitative variables in each assessment period (between 30 days and three months, between 30 days and six months and between three and six months), was estimated the coefficients of correlation between the change in LBM and age.?Similarly, variation between the MCM and the duration of obesity, taking into account the variable age and the variation in LBM between 30 days and three months, the correlation coefficient between age and this variation was equal to -0.26, with statistical significance (p = 0.009).?This indicates that there is a correlation between age and changes in LBM between 30 days and three months and that this correlation is inverse (negative).?Individuals with lower age have lower loss of MCM and older have higher losses (Table 5 and Figure 1).
The duration of obesity has not been shown to be associated with variations in MCM (Table 5).?
in all evaluated periods (p <0.001). In the comparison of assessments three months and 30 days was a significant difference (p <0.001) in patients undergoing physiotherapy counter resisted. Also in the comparisons between 30 days and six months and between three and six months, there was evidence of significant difference in mean fat mass (p <0.001) in both comparisons in patients undergoing physiotherapy counter resisted. Table 3 presents descriptive statistics of body fat mass at each time of evaluation and the variations between these times.
The results of lean body mass analysis indicated that there is significant difference between the three assessments (p <0.001). By comparing the 30-day trial with three months, there was loss of lean body mass with statistical significance (p <0.001). Similarly, between 30 days and six months (p <0.001). However, the period between three months and six months shows no significant results (p <0.612), showing a tendency to maintain MCM (Table 4).
In view of the research be directed to the action of physiotherapy, it was considered important to assess factors that may be associated with variations in lean body mass after surgery and during physical therapy treatment. Thus, the focus in the following analysis has direct relation to lean body mass.
Initially, was assessed the gender, diabetes mellitus, dyslipidemia, cardiovascular and orthopedic diseases. In this analysis, was compared the groups defined by ratings of the factors evaluated in relation to the means of variations in lean body mass between 30 days and three months, between three and six months and between 30 days and six months. Next, was assessed the correlation of changes in LBM in the periods analyzed with age and the duration of obesity. These correlations were also assessed lean body mass with the assessments of total body mass, body mass index and fat body mass before the operation.
Analyzing the sample, it was found that on average there was a loss of lean body mass both in males as in females, but there was greater decrease in men with a significant difference in the periods between 30 days and three months and between 30 days and six months .
In the analysis of patients with diabetes mellitus, was found that between three and six months, on average, subjects lost 1.8 kg of lean body mass, while those who had not gained an average of 1.5 kg ( p = 0.001). There was no significant difference between diabetic and nondiabetic variations in lean body mass in the other two periods.
There was loss of lean body mass increased in patients with dyslipidemia compared to those without it, showing significant loss of lean body mass in three to six months. Between 30 days and three months there was no difference between patients with and without dyslipidemia. Already, between 30 days and six months, there is a tendency that individuals with it lose more lean body mass than without it.
Patients with cardiovascular disease presented loss of MCM in periods of three to six months and 30 days to six months, without significant difference compared to those without cardiovascular disease. In periods of 30 days to three months there was greater loss of lean body mass in patients without them.
There was greater loss of lean body mass during periods of three months and six months in patients with orthopedic diseases without significant differences. In periods of 30 days and six months tended to gain in LBM in patients who had no skeletal disease.
Regarding the quantitative variables in each assessment period (between 30 days and three months, between 30 days and six months and between three and six months), was estimated the coefficients of correlation between the change in LBM and age. Similarly, variation between the MCM and the duration of obesity, taking into account the variable age and the variation in LBM between 30 days and three months, the correlation coefficient between age and this variation was equal to -0.26, with statistical significance (p = 0.009). This indicates that there is a correlation between age and changes in LBM between 30 days and three months and that this correlation is inverse (negative). Individuals with lower age have lower loss of MCM and older have higher losses (Table 5 and Figure 1).
The duration of obesity has not been shown to be associated with variations in MCM (Table 5).
Analytical studies
Of the 100 patients studied, 45 showed a reduction of MCM in the two periods (Group A) and 55 earned in at least one of the periods (Group B). This indicates that the estimated percentage of patients who gained lean body mass during the period of physical therapy was 55% (95% from 45% to 65%). Were compared regarding the variables: age, duration of obesity, gender, dyslipidemia, diabetes mellitus, cardiovascular diseases, orthopedic diseases.
Of the female patients were 58.82% in group B, ie, gained lean body mass in at least a period of physiotherapy. For men, this percentage was 46.88%, with no significant difference between groups (p = 0.288).
The patients with diabetes mellitus were mostly (67.27%) in group A, ie, lean body mass lost during the periods evaluated for physical therapy, statistical difference compared with nondiabetic patients (p <0.001) .
Most patients with dyslipidemia (63.93%) belonged to Group A, i.e, lost MCM during the periods evaluated with significant differences with respect to individuals who not had dyslipidemia (p <0.001).
Although it has been observed that a higher percentage of patients without cardiovascular disease belonged to Group B, no statistically significant difference was observed between patients with and without cardiovascular disease (p = 0.212). There was no significant difference (p = 0.100) between patients with and without orthopedic disease in relation to groups, but most of them that do not carried it(70.83%) belonged to Group B. With respect to mean age, no significant difference (p = 0.785) was found. Also in relation to the time of obesity, no difference was observed between the groups.
DISCUSSION
In the scenario of the exercise protocols applicable to health and rehabilitation, the resisted training have significant evidence for its use. But it is important to note that the variety of points of action does not permit effective balance on the results of various protocols. As an example, the program of Van Etten et al., cited by Bouchard3 in 18 weeks of resistance training - made in sedentary young men from 23 to 41 years (twice a week, three sets of 15 repetitions for the major muscle groups) -, obtained an average of 2.1 pounds of body fat and increased 2.1 kg of fat-free body mass. This program promoted an increase of 260 kcal per day of daily caloric expenditure.
Resistance exercise may represent a good alternative for increasing lean body mass and fat oxidation. According to Bouchard3 resistance exercises can help obese to increase this rate (MCM) or at least slow its loss. This statement was confirmed when is compared the study of Cunha et al.5, with the result of counter-kinesiotherapy resisted (this study), which gave an average loss of 43.86 kg of fat mass after the counter-resisted kinesiotherapy against an average of 39.8 kg, with a loss equivalent to 11% of MCM in the same time interval of six months.
The MCM is considered the most active tissue in the human body, being composed of fat-free mass, coupled with the lowest possible amount of fat (essential fat). Therefore, its maintenance is essential for reducing fat mass over14. Observed in this study that there was no evidence of significant reduction in weight profile of MCM in both female and male gender. It can be inferred that the metabolic profile of these individuals experienced no significant loss of active tissue.
Bean1 in preparation of the book "The Complete Guide to Strength Training", showed that the increase of 1.36 pounds of muscle increases the metabolic rate during periods of rest in 7% and the daily requirement of calories by 15%. Strength training also increases metabolism during exercise. At rest 0.45 kg of muscle requires 35 calories per day. During exercise, energy expenditure rises dramatically five to ten times more than resting levels. So the more muscle tissue there is, the greater the number of calories expended during exercise and at rest. Mônaco et al.15 showed the percentage loss of excess weight (% PEP) of 53.60. The results of this study valued 64% for the same item, corroborating with what says Bean1.
The results of Bean1 and Mônaco et al.15 justify the statement done by Bopp and Lucas2, when defend the use of strength training (kinesiotherapy synonymous with counter-resisted, resisted exercises, bodybuilding therapy) in pre-and postoperative metabolic and bariatric operations.
CONCLUSION
Physiotherapy counter-resisted: 1) helped the loss of total body mass, body mass index and fat body mass and maintained lean body mass between the periods of three months and six months; 2) older men, patients with diabetes and dyslipidemia lost more lean mass, and the duration of obesity, cardiovascular disease and orthopedic variations did not interfere in lean mass, 3) groups A and B showed no significant differences to gain or loss in relation to cardiovascular disease and orthopedic diseases; however, patients with diabetes mellitus and dyslipidemia were more in Group A.
REFERENCES
- 1. Bean A. O guia completo de treinamento de força. Editora Manole. Ed. 1, p. 233, 1999.
- 2. Bopp D, Lucas RW. As especialidades associadas à cirurgia barátrica. COESAS (Comissão das Especialidades Associadas), 2009
- 3. Bouchard C, Tremblay A. Genetic influences on the response of body fat distribution to positive and negative energy balances in human identical twins. J Nutr. v. 127, p. 943S-7S, 1997
- 4. Buchwald H, Williams SE. Bariatric surgery worldwide. Obes Surg 2004; 14(9):1157-64.
- 5. Cunha SFC, Sanches M, Faria A, Santos JE, Nonino-Borges C. Evolução da massa corporal magra após12 meses da cirurgia bariátrica. Rev Nutr. 2010; 23(4): 535-541
- 6. Fernández-López JA, Remesar X, Foz M, Alemany M. Pharmacological approaches for the treatment of obesity. Drugs 2002; 62(6):915-44.
- 7. Garrido Jr. AB, Matielli JD. Tratamento Cirúrgico do Paciente Obeso. Obesidade e Síndrome Metabólica para o Clínico. In: Halpern A, Mancini M. Ed. Roca, São Paulo, pp. 267-290, 2009.
- 8. Heyward V, Stolarczyk L. Avaliação da Composição Corporal Aplicada. São Paulo. Editora Manole, 2000.
- 9. Hirofumi T, Monahan KD, Seals DR. Age-Predicted Maximal Heart Rate Revisited. J Am Coll Cardiol. 2001; 37:153-156.
- 10. Lancha JR. Obesidade - Uma Abordagem Multidisciplinar, Rio de janeiro: Ganabara Koogan, 2006.
- 11. Lima CW, Lucas RWC. Índice de Massa Corporea (IMC) e predição de obesidade. Rev Bariátrica & Metabólica 2010; 1(1):14-29.
- 12. Lucas RWC, Bopp D. Fisioterapia - Fisioterapia bariátrica: procedimentos fisioterapêuticos aplicados no universo da cirurgia bariátrica. In: Franques ARM. As especialidades à cirurgia bariátrica. COESA. São Paulo, 2009.
- 13. Lucas RWC. Musculação Terapêutica - Aplicação de padrões de movimentos anatomo-funcionais, na Saúde, na recuperação físico-funcional e no desporto. Florianópolis: Sistema Wallace Consultoria Ltda, SC, 2010
- 14. Mancini MC. Tratado de Obesidade. Guanabara Koogan Ltda, 2010.
- 15. Mônaco DV, Merhi VAL, Aranha N, Brandalis A, Brandalise NA. Impacto da cirurgia bariátrica "tipo capella modificado" sobre a perda ponderal em pacientes com obesidade mórbida. Rev Ciênc Méd. 2006; 15(4): 289-298.
- 16. Nassif DSB, Malafaia O, Nassif PAN, Kuretzki CH, Lucas RWC, Pinto JSP. Protocolo eletrônico multiprofissional em cirurgia bariátrica. ABCD Arq Bras Cir Dig. 2011; 24(3):215-218.
Effect of counter resisted physiotherapy in relationship to the lean body mass after bariatric surgery
Publication Dates
-
Publication in this collection
15 Dec 2011 -
Date of issue
Sept 2011
History
-
Received
18 Jan 2011 -
Accepted
03 May 2011