INTRODUCTION
Abdominal cocoon is a rare disease which causes small-bowel obstruction that is characterized by a thick, fibrotic and cocoon-like membrane encapsulating total or partially the small bowel11. Serafimidis C, Katsarolis I, Vernadakis S, Rallis G, Giannopoulos G, Legakis N, Peros G: Idiopathic sclerosing encapsulating peritonitis(or abdominal cocoon). BMC surgery J 2006, 6:3.,22. Tombak MC, Apaydin FD, Colak T, Duce MN, Balci Y, Yazici M, Kara E: An unusual cause of intestinal obstruction: Abdominal Cocoon. AJR Am J Roentgenol 2010; 194:W176-W178.,33. Xu p, Chen LH, Li YM: Idiopathic scleroting encapsulating peritonitis (or abdominal cocoon): A report of 5 Cases. World J Gastroenterol 2007; 13(26): 3649-3651.. Its etiology remains unknown44. Tannoury JN, Abboud BN: Idiopathic sclerosing encapsulating peritonitis: Abdominal cocoon. World J Gastroenterol 2012; 18(17):A.,55. Wei B, Wei HB, Guo WP, Zheng ZH, Huang Y, Hu BG, Huang JL: Diagnosis and treatment of abdominal cocoon: a report of 24 cases. Am J Surg. 2009 Sep;198(3):348-53. Surgical management is the treatment of choice11. Serafimidis C, Katsarolis I, Vernadakis S, Rallis G, Giannopoulos G, Legakis N, Peros G: Idiopathic sclerosing encapsulating peritonitis(or abdominal cocoon). BMC surgery J 2006, 6:3.. In this report, it is described a young patient with abdominal cocoon who presented clinical signs and paraclinical findings of intestinal obstruction.
CASE REPORT
In July 2010 a 25 year-old man was admitted with 2-month history of intermittent colicky abdominal pain and bilious vomiting and abdominal distension. He also complained from chronic constipation, anorexia and 14 kg weight loss during the previous two months. He had no surgical or other medical history except using of a body building supplement drugs which contain creatin.
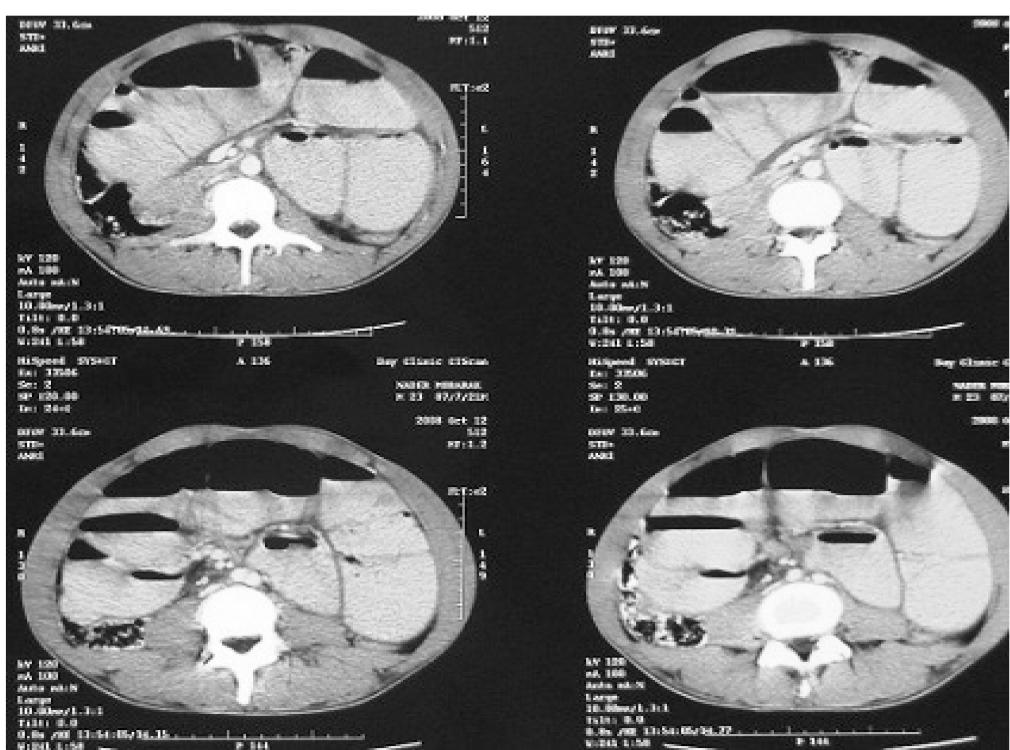
On physical examination he was anxious. Vital signs were normal (blood pressure 110/75, pulse rate 85/min, temperature 37.3º C). Abdominal distention with hyperactive bowel sounds and mild tenderness in the whole of the abdomen especially in left upper quadrant were detected at physical examination. There were no abdominal scars, palpable abdominal mass or organomegaly. Digital rectal examination was normal. Laboratory blood analysis ascertained a total leukocyte count 8500 cell/ml, hemoglobin 16 mg/dl, normal serum chemistry and normal urine analysis. Up right plain abdominal X-ray showed multiple air-fluid levels without free gas under the diaphragm. The barium X-ray showed jejunal and ileal loops dilatation with the contrast medium passing slowly (Figure 1). Contrast-enhanced abdominal computed tomography showed small bowel loops and dilatation (Figure 2).
Due to signs of mechanical small bowel obstruction an emergency laparotomy was performed through a midline incision. During surgery the small bowel dilatation was observed; its mesentery was edematous and the whole small bowel covered by a dense whitish membrane which gave the appearance of a cocoon (Figure 3). Careful sharp and blunt dissection with excision of the membrane enveloping the small bowel was performed and the whole small intestine was freed and followed from duodenojejunal angle to ileocecal junction. The histopathology of the peeled off membrane revealed a chronic non-specific inflammatory reaction with proliferation of fibroconnective tissue.
Intraoperative photograph showing small intestine encapsulated in white, thickened cocoon-like membrane
The patient was discharged from the hospital on the 8th postoperative day. After 24 months regular follow-up he was in satisfactory condition and the abdominal plain showed normal appearance.
DISCUSSION
Sclerosing encapsulating peritonitis can be classified as idiopathic and secondary. The idiopathic class or abdominal cocoon was first described by Foo et al in 197866. Foo KT, Ng KC, Rauff A, Foong WC, Sinniah R: Unusual small intestinal obstruction in adolescent girls: the abdominal cocoon. Br J Surg 1978, 65:427-430.. The idiopathic type primarily affects young females from tropical and subtropical countries11. Serafimidis C, Katsarolis I, Vernadakis S, Rallis G, Giannopoulos G, Legakis N, Peros G: Idiopathic sclerosing encapsulating peritonitis(or abdominal cocoon). BMC surgery J 2006, 6:3..The cause of this rare condition is unknown22. Tombak MC, Apaydin FD, Colak T, Duce MN, Balci Y, Yazici M, Kara E: An unusual cause of intestinal obstruction: Abdominal Cocoon. AJR Am J Roentgenol 2010; 194:W176-W178.,33. Xu p, Chen LH, Li YM: Idiopathic scleroting encapsulating peritonitis (or abdominal cocoon): A report of 5 Cases. World J Gastroenterol 2007; 13(26): 3649-3651. although a number of hypotheses have been mentioned44. Tannoury JN, Abboud BN: Idiopathic sclerosing encapsulating peritonitis: Abdominal cocoon. World J Gastroenterol 2012; 18(17):A.,77. Devay AO, Gomceli I, Korukluoglu B, Kusdemir A: An unusual and difficult diagnosis of intestinal obstruction: The abdominal cocoon. Case report and review of the literature. World J Emerg Surg 2006, 1:8.. Abdominal cocoon is characterized by a thick shiny fibrotic membrane, with total or partial encasement of the small intestine55. Wei B, Wei HB, Guo WP, Zheng ZH, Huang Y, Hu BG, Huang JL: Diagnosis and treatment of abdominal cocoon: a report of 24 cases. Am J Surg. 2009 Sep;198(3):348-53.
In clinical presentation, abdominal cocoon is presented by recurrent attacks of acute or subacute small bowel obstruction, nausea, weight loss and anorexia and sometimes with palpable abdominal mass. Most patients are diagnosed incidentally at laparotomy and preoperative diagnosis requires a high index of clinical suspicion88. Kawaguchi Y, Kawanishi H, Mujais S, Topley N, Oreopoulos DG: Encapsulating peritoneal sclerosis: definition, etiology, diagnosis, and treatment. International society for peritoneal dialysis ad hoc committee on ultradiltration management in peritoneal dialysis: Perit Dial Int. 2000, 20 supple 4: 543-55..
This patient had used some supplements for body buildings such as creatin for four years. No reference was found in the literature any association between medication given and abdominal cocoon.
WBC count, C-reactive protein level, hypoalbuminemia and anemia are common findings in SPE cases but no significant sign was observed in this case22. Tombak MC, Apaydin FD, Colak T, Duce MN, Balci Y, Yazici M, Kara E: An unusual cause of intestinal obstruction: Abdominal Cocoon. AJR Am J Roentgenol 2010; 194:W176-W178.. Imaging has an important role in the diagnosis of abdominal99. Hur j, Kim KW, Park MS, Yu JS: Abdominal cocoon preoperative diagnostic clues from radiologic imaging with pathologic correlation. AJR Am J Roentgenol 2004, 182:639-641.. Barium X-ray and contrast CT are useful for the diagnosis of abdominal cocoon preoperatively55. Wei B, Wei HB, Guo WP, Zheng ZH, Huang Y, Hu BG, Huang JL: Diagnosis and treatment of abdominal cocoon: a report of 24 cases. Am J Surg. 2009 Sep;198(3):348-53. Dilated bowel loops with multiple air-fluid level may be shown in conventional abdominal X-ray but they are nonspecific55. Wei B, Wei HB, Guo WP, Zheng ZH, Huang Y, Hu BG, Huang JL: Diagnosis and treatment of abdominal cocoon: a report of 24 cases. Am J Surg. 2009 Sep;198(3):348-53,77. Devay AO, Gomceli I, Korukluoglu B, Kusdemir A: An unusual and difficult diagnosis of intestinal obstruction: The abdominal cocoon. Case report and review of the literature. World J Emerg Surg 2006, 1:8.. The classic findings of abdominal CT consist of small bowel loops congregation in the center of abdomen with a non-enhancement fibrous membrane surrounding the bowl loops that is best visualized on computed axial tomography scan33. Xu p, Chen LH, Li YM: Idiopathic scleroting encapsulating peritonitis (or abdominal cocoon): A report of 5 Cases. World J Gastroenterol 2007; 13(26): 3649-3651.,55. Wei B, Wei HB, Guo WP, Zheng ZH, Huang Y, Hu BG, Huang JL: Diagnosis and treatment of abdominal cocoon: a report of 24 cases. Am J Surg. 2009 Sep;198(3):348-53,1010. Wig JD, Gupta SK: Computed tomography in abdominal cocoon. J Clin Gastreoenterol 1998, 26:156-157.. Surgical dissection and excision of the membrane and adhesionlysis remain the cornerstone in the treatment of abdominal cocoon22. Tombak MC, Apaydin FD, Colak T, Duce MN, Balci Y, Yazici M, Kara E: An unusual cause of intestinal obstruction: Abdominal Cocoon. AJR Am J Roentgenol 2010; 194:W176-W178.,55. Wei B, Wei HB, Guo WP, Zheng ZH, Huang Y, Hu BG, Huang JL: Diagnosis and treatment of abdominal cocoon: a report of 24 cases. Am J Surg. 2009 Sep;198(3):348-53. In reported case with an insignificant history, a dilated small bowel with an edematous mesentery and a dense whitish membrane coverage on bowel observed in operation which advised idiopathic sclerosing peritonitis
Because of increasing morbidity and mortality following bowel resection, only if it is nonviable, resection of the bowel is indicated77. Devay AO, Gomceli I, Korukluoglu B, Kusdemir A: An unusual and difficult diagnosis of intestinal obstruction: The abdominal cocoon. Case report and review of the literature. World J Emerg Surg 2006, 1:8.. In this case an emergency laparotomy was performed and an edematous mesentery covered by a dense whitish membrane wasd observed and incised carefully, separated from the intestinal serosa by sharp and blunt dissection.
In general, prognosis of abdominal cocoon after surgery is satisfactory and excision of the thick membrane and release of the small intestine leads to complete recovery.
In conclusion sclerosing encapsulating peritonitis is not common and definite preoperative diagnosis is difficult. The recurrent episodes of small bowel obstruction combined with relevant preoperative findings at imaging studies and lack of other causes can facilitate preoperative diagnosis of abdominal cocoon.
REFERENCES
-
1Serafimidis C, Katsarolis I, Vernadakis S, Rallis G, Giannopoulos G, Legakis N, Peros G: Idiopathic sclerosing encapsulating peritonitis(or abdominal cocoon). BMC surgery J 2006, 6:3.
-
2Tombak MC, Apaydin FD, Colak T, Duce MN, Balci Y, Yazici M, Kara E: An unusual cause of intestinal obstruction: Abdominal Cocoon. AJR Am J Roentgenol 2010; 194:W176-W178.
-
3Xu p, Chen LH, Li YM: Idiopathic scleroting encapsulating peritonitis (or abdominal cocoon): A report of 5 Cases. World J Gastroenterol 2007; 13(26): 3649-3651.
-
4Tannoury JN, Abboud BN: Idiopathic sclerosing encapsulating peritonitis: Abdominal cocoon. World J Gastroenterol 2012; 18(17):A.
-
5Wei B, Wei HB, Guo WP, Zheng ZH, Huang Y, Hu BG, Huang JL: Diagnosis and treatment of abdominal cocoon: a report of 24 cases. Am J Surg. 2009 Sep;198(3):348-53
-
6Foo KT, Ng KC, Rauff A, Foong WC, Sinniah R: Unusual small intestinal obstruction in adolescent girls: the abdominal cocoon. Br J Surg 1978, 65:427-430.
-
7Devay AO, Gomceli I, Korukluoglu B, Kusdemir A: An unusual and difficult diagnosis of intestinal obstruction: The abdominal cocoon. Case report and review of the literature. World J Emerg Surg 2006, 1:8.
-
8Kawaguchi Y, Kawanishi H, Mujais S, Topley N, Oreopoulos DG: Encapsulating peritoneal sclerosis: definition, etiology, diagnosis, and treatment. International society for peritoneal dialysis ad hoc committee on ultradiltration management in peritoneal dialysis: Perit Dial Int. 2000, 20 supple 4: 543-55.
-
9Hur j, Kim KW, Park MS, Yu JS: Abdominal cocoon preoperative diagnostic clues from radiologic imaging with pathologic correlation. AJR Am J Roentgenol 2004, 182:639-641.
-
10Wig JD, Gupta SK: Computed tomography in abdominal cocoon. J Clin Gastreoenterol 1998, 26:156-157.
Publication Dates
-
Publication in this collection
Jan-Mar 2014
History
-
Received
13 Aug 2012 -
Accepted
16 Apr 2013