
Abstracts
BACKGROUND: Sexually transmitted diseases in children remain a public health concern that is relatively ignored. Further data are required on the management of these diseases and their association with child sexual abuse. OBJECTIVES: To describe the clinical and epidemiological profile of sexually transmitted diseases in children receiving care at a referral center in the city of Manaus, Amazonas, Brazil. METHODS: A descriptive, exploratory study was conducted to evaluate the clinical, epidemiological and laboratory characteristics of the sexually transmitted diseases (STD) found in children who received care at this clinic between January 2003 and December 2007. RESULTS: A total of 182 children with STDs were included in the study. The majority were female (65.4%), dark-skinned and with a mean age of 8.5 years. Furthermore, 89% were from the city of Manaus and their parents were usually responsible for having brought them to the clinic. Genital warts constituted the principal diagnosis in children of both sexes and 90.1% of the children had only one STD. CONCLUSIONS: The frequencies and clinical characteristics of the STDs in the children in this study were similar to data reported in the literature. Although the signs and symptoms of the STDs found in these children do not, in themselves, constitute reliable parameters by which to confirm abuse, professionals should always be alert to this possibility, since these diseases may represent a sign of sexual offenses that may be dissimulated and repetitive.
Child; Epidemiology; Sexually transmitted diseases
FUNDAMENTOS: Doenças Sexualmente Transmissíveis em crianças permanecem um problema de saúde pública pouco estudado, sendo ainda necessários esclarecimentos sobre seu manejo e a relação destas com o abuso sexual infantil. OBJETIVOS: Descrever o perfil clínico-epidemiológico das Doenças Sexualmente Transmissíveis em crianças atendidas em centro de referência na cidade de Manaus. MÉTODOS: Realizou-se estudo descritivo exploratório para verificar características clínicas, epidemiológicas e laboratoriais das Doenças Sexualmente Transmissíveis em crianças atendidas durante o período de janeiro/2003 a dezembro/2007. RESULTADOS: Foram incluídas no estudo 182 crianças que apresentavam DST. A maioria era do sexo feminino (65,4%) e de cor parda; a média de idade foi de 8,5 anos; 89% eram procedentes da cidade de Manaus; os pais foram os principais acompanhantes na consulta; verruga genital foi o principal diagnóstico em ambos os sexos; e, 90,1% apresentavam apenas uma DST. CONCLUSÃO: As frequências e características clínicas das DST nas crianças do estudo não diferiram do encontrado na literatura. Embora, com base em sinais e sintomas referentes tão somente às DST nas crianças, não se tenham parâmetros fidedignos de confirmação de abuso, deve-se sempre estar alerta para esta possibilidade, visto que estas doenças podem ser sinalizadoras de ofensas sexuais, por vezes, dissimuladas e repetidas.
Criança; Doenças sexualmente transmissíveis; Epidemiologia
INVESTIGATION
Clinical and epidemiological profile of sexually transmitted diseases in children attending a referral center in the city of Manaus, Amazonas, Brazil*
Carla Barros da Rocha RibasI; Maria da Graça Souza CunhaII; Antônio Pedro Mendes SchettiniIII; Jonas RibasIV; Josie Eiras Bisi dos SantosV
IMaster's degree. Dermatologist. Coordinator of the Medical Residency Program, Alfredo da Matta Foundation of Tropical Dermatology and Venereology, Manaus, Amazonas, Brazil
IIDoctorate degree in dermatology. Alfredo da Matta Foundation of Tropical Dermatology and Venereology, Manaus, Amazonas, Brazil
IIIMaster's degree. Dermatologist, Alfredo da Matta Foundation of Tropical Dermatology and Venereology, Manaus, Amazonas, Brazil
IVMaster's degree. Head, Dermatology Department, and Professor of Dermatology, Federal University of Amazonas, Manaus, Amazonas, Brazil
VDermatologist at the Belém General Hospital, Belém, Pará, Brazil
Mailing address
ABSTRACT
BACKGROUND: Sexually transmitted diseases in children remain a public health concern that is relatively ignored. Further data are required on the management of these diseases and their association with child sexual abuse.
OBJECTIVES: To describe the clinical and epidemiological profile of sexually transmitted diseases in children receiving care at a referral center in the city of Manaus, Amazonas, Brazil.
METHODS: A descriptive, exploratory study was conducted to evaluate the clinical, epidemiological and laboratory characteristics of the sexually transmitted diseases (STD) found in children who received care at this clinic between January 2003 and December 2007.
RESULTS: A total of 182 children with STDs were included in the study. The majority were female (65.4%), dark-skinned and with a mean age of 8.5 years. Furthermore, 89% were from the city of Manaus and their parents were usually responsible for having brought them to the clinic. Genital warts constituted the principal diagnosis in children of both sexes and 90.1% of the children had only one STD.
CONCLUSIONS: The frequencies and clinical characteristics of the STDs in the children in this study were similar to data reported in the literature. Although the signs and symptoms of the STDs found in these children do not, in themselves, constitute reliable parameters by which to confirm abuse, professionals should always be alert to this possibility, since these diseases may represent a sign of sexual offenses that may be dissimulated and repetitive.
Keywords: Child; Epidemiology; Sexually transmitted diseases
INTRODUCTION
Sexually transmitted diseases (STD) consist of a group of endemic diseases of varying clinical presentation, characterized epidemiologically as sexually transmitted infections.
Few studies have been conducted on STDs in children and most have emphasized sexual abuse in detriment to the STDs themselves. A study conducted by Pitché et al. (2001) in Togo reported 33 cases of STDs in children up to 11 years of age, emphasizing the role of sexual abuse within this context. 1 In a retrospective study conducted in a specialist clinic in Nigeria, Olayinka & Olayinka (2002) described 102 cases of STDs in children up to 13 years of age who attended consultations within a 12-year period, highlighting the real problem of these diseases in the pediatric population. 2
Likewise, in 2003 Pandhi et al. conducted a study in New Delhi, India and reported 127 cases of STDs in children under 15 years of age, showing that children represent a significant subgroup of the population affected by STDs. 3 In the city of Rio de Janeiro, Brazil, Figueiredo et al. (1997) performed a review study referring to the 1988 to 1996 period and identified STDs in 77% of the 22 children attending consultations at the STD clinic of a university teaching hospital. 4 In a cross-sectional study conducted with 1,182 patients seen during the year of 1995 at the STD clinic of the Fluminense Federal University in Rio de Janeiro, Tibúrcio et al. (2000) highlighted the importance of a descriptive epidemiological study to identify factors capable of interfering with the dynamics of these infections in the population. 5 In another similar study conducted with 1,333 patients with STDs attending a healthcare center at the school of public health, São Paulo University, Fagundes et al. (2001) evaluated the epidemiological, clinical and laboratory characteristics of patients, and reported cases in children from the age of two years upwards. 6
Sexually transmitted diseases in children may result from a congenital infection, perinatal transmission or from a postnatal infection acquired by selfinoculation, heteroinoculation or from sexual intercourse, the latter generally occurring within the context of sexual abuse.
A careful interpretation of STDs, based on the etiological agent, the incubation period, the age of the child and the site of the infection, may corroborate towards an evidence of sexual abuse, particularly in infections that occur outside the perinatal period; however, they are rarely conclusive. 7
Accidental transmission, either by fomites, physical contact or self-inoculation, is rare in children, as reported by Neinstein et al. (1984) and Estreich & Foster (1992). 8,9 Therefore, two factors are essential in the management of STDs in children: early and accurate diagnosis and investigation into the mode of transmission to evaluate the possibility of sexual abuse.
The objective of the present study was to evaluate the epidemiological, clinical and laboratory characteristics of children with STDs who were receiving care at the Alfredo da Matta Foundation of Tropical Dermatology and Venereology, a referral center situated in the city of Manaus, Amazonas, Brazil.
Material and Methods
Following approval by the Internal Review Board of the Alfredo da Matta Foundation, an epidemiological study with a descriptive, exploratory approach was conducted by reviewing patients' charts and notification records, verifying the clinical, epidemiological and laboratory characteristics of sexually transmitted diseases in children and the patients' characteristics, including data on gender, age, race and place of birth.
Children between 0-12 years old with a confirmed STD or suspected of having an STD, who had been referred by other units within the healthcare network or had attended the clinic spontaneously for consultation with a specialist in a referral center between January 2003 and December 2007 were included in the study.
The data were collected, stored and consolidated for analysis using the Epi-Info software program, version 3.4.3 for Windows. Variables used in the descriptive analysis included data regarding the presence of an adult accompanying the child during consultation and the etiological agent involved. Etiological and syndromic diagnoses of the STDs were made. The mean age of the children with an STD who had been referred by the child protection authorities and the age of the children with an STD who had arrived at the clinic through other means were compared.
Results
Over the 5-year period evaluated, 12,770 patients were seen at the STD clinic of this institute and 296 (2.3%) of whom were children between 0-12 years age group. Among this group, 182 children with STD (61.5%) were included in the study (Table 1).
In the study group, 119 of the children were girls (65.4%) and 63 (34.6%) were boys. The mean age of the children included in the study was 8.5 ± 3.3 years [mean ± standard deviation (SD)] and the mean age at initiation of sexual activity reported as voluntary was 11 ± 1.1 years.
With respect to skin color/ethnicity, the majority of children were brown-skinned (59.3%), followed by white (15.4%), African-Brazilian (4.9%), of native Indian descent (3.3%) and Asians (1.1%). In 15.9% of the patients' records, information on ethnicity was missing.
Most of the patients (89%) were from the city of Manaus; however, 9.9% were from other towns in the state of Amazonas and 1.1% of patients were from towns in other states.
The number of patients attending the clinic was classified as follows: 43.3% of patients arrived spontaneously seeking specialist attention, 21.4% were referred from other basic healthcare units, 19.2% were referred by the child protection authorities and 3.8% through other types of referral. In 12.1% of cases, this information was missing.
With respect to the presence of an accompanying adult during the consultation, 63 children were accompanied by their parents, 17 by other family members and two with known friends. This information were not confirmed in a 100 cases.
The syndromic diagnoses of the STDs are listed in Table 2 in accordance to the gender of the child. As shown in the referred table, 51.6% of the boys had anogenital warts, 37.1% had urethral discharge syndrome and 11.3% had genital ulcer syndrome. Of the girls, 43.7% had anogenital warts, 40.8% had vaginal discharge, 10.6% had cervical discharge and 4.9% had genital ulcer.
Table 3 shows the distribution of cases based on the etiological agent in accordance to the gender of the child. Among the boys, 50.8% had condyloma acuminata, 19% had gonorrhea, 17.5% had other types of urethritis, 6.3% had genital herpes, 3.2% had syphilis and 1.6% had candidiasis. Among the girls, 47% had condyloma acuminata, 14.4% bacterial vaginosis, 11.4% candidiasis, 10.6% other types of cervicitis, 5.3% genital herpes, 5.3% gonorrhea and 3.8% trichomoniasis, while 1.5% tested positive for HIV and 0.8% had syphilis.
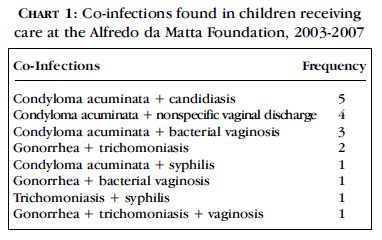
Among the 182 patients diagnosed with a STD in this population sample, 164 (90.1%) had only one condition, while 18 (9.9%) had more than one STD. Table 4 shows the co-infections found in the study group.
Follow-up by the child protection authorities was provided in cases in which sexual abuse was suspected or confirmed. Among the 59 patients followed up by the authorities, 16 girls and 8 boys had been referred by the clinic. Of the 35 patients referred to this clinic by the child protection authorities, 33 were girls and 2 were boys.
The patients with STDs who were being followed-up by the child protection authorities, 14 cases had condyloma acuminata, 13 patients had other types of cervicitis, 11 cases had bacterial vaginosis, 10 had gonorrhea, 7 had candidiasis, 4 had trichomoniasis, 3 had syphilis, 2 had genital herpes and 1 had another form of urethritis.
The mean age of the children with a diagnosis of STD who had been referred by the child protection authorities with a suspicion of sexual abuse was 10.8 ± 1.6 years. The mean age of the patients with a STD who were attended at the clinic by other referrals was 7.9 ± 3.4 years.
Discussion
The frequency of STD found in this study (2.3%) was higher than rates reported in Niterói, Brazil (0.51%) and in New Delhi, India (0.82%). 10,3 The majority of studies on this subject is used as a helpful sample, the rate found here does not necessarily mean that the problem is more severe in this region; nevertheless, the need to perform further studies about of STDs in children in this region should be emphasized.
With respect to the demographic characteristics found in this sample population, there was a predominance of brown-skinned individuals (59.3%), which is the most common skin color in the region. 11 Of the STDs diagnosed, 3.3% were detected in individuals of native Indian descent. The identification of STDs in this specific population is a concern and was reported in a recent prevalence study conducted in six state capital cities in Brazil. 12
It is important to mention that there was a predominance of males among the patients seen during this study period, a finding that is in agreement with data reported in a study conducted by Fagundes et al. (2001). 6 On the other hand, the prevalence of females among the children attended, which has also been reported by other authors, raises the hypothesis that girls are probably more often the targets of enticement/pedophilia. 13-15
The finding that the great majority of children were consulted at the clinic were from the capital city of the state of Amazonas is in agreement with data on the overall demand of patients receiving care at the STD clinic, thus reproducing the daily routine of the service in which the study was conducted.
With respect to the way in which the patient arrived at the clinic, 44.5% were found to have been referred, while 43.4% consulted spontaneously, indicating a need to improve the referral and counterreferral process with the public healthcare network.
Among the patients who had been referred to the clinic, 43.2% had been referred by the child protection authorities in the region, highlighting the important role of this department in the management of cases in which there is suspicion or confirmation of mistreatment.
The mean age of the children diagnosed with STD and referred by the child protection authorities was 10.8 years. On the other hand, the mean age of the children who arrived at the clinic by other means was 7.9 years.
The higher mean age of the children who had been referred by the child protection authorities may be related to the work carried out by this department, particularly in the form of programs to help combat the sexual and commercial abuse of children and adolescents.
With respect to the presence of an accompanying person during the consultation, this information was found to be missing in a high proportion of cases, justified by the absence of any specific field on the form in which to register this information. Nevertheless, this information is obligatory on the records of patients in this age group. The accompanying persons mentioned, the majority consisted of parents, showing that in this study population the family was already aware of the possibility that the child had a disease.
Information about the age which is voluntary sexual activity that initiated was recorded on the charts of 34 patients (18.7%), mean age at initiation was 11 years old. Regardless the possibility of children acquiring a STD from sexual partners with whom they had sexual intercourse referred to as "voluntary", sexual activity with individuals under 14 years old is classified and presumed violence in accordance and the Brazilian penal code (article 224), and the sexual partner is subject to prosecution. 16,17
Based on a syndromic approach, 204 diagnoses were made in the 182 patients in this group. With the exception of anogenital warts, findings in the group of patients attending this clinic were similar to those found in patients attending STD clinics evaluated in a study on the prevalence and frequency of STDs in six Brazilian state capital cities. 12
Genital infections caused by candidiasis and bacterial vaginosis, although not strictly considered as STD, were considered in the syndromic diagnosis as vaginal/cervical discharge.
Cases of genital ulcers in which there was a history or evidence of vesiculous lesions has been diagnosed as genital herpes.
HPV infections are expressed clinically as condyloma acuminata, or genital warts. Nevertheless, these infections may be asymptomatic or may even take on a subclinical form, visible only under magnification, which is rarely performed in children.
With respect to the etiological diagnoses of the STDS of bacterial origin (11.8%), the most common was gonococcal infections (82.6%), which were found predominantly in boys. As for the STDs of viral origin (54.9%), condyloma acuminata was the most common (87.9%), occurring principally in girls.
In comparison, the study on the prevalence of STDs in men and women attending STD clinics in six Brazilian state capital cities found bacterial STDs in 14.4% of patients and viral STDs in 41.9%, similar proportions to those found in the present study. 12
It should be emphasized that, although the majority of children had only one STD, 9.9% were affected by more than one disease, showing that an association of STDs is often present, even in children, and reinforcing the importance of testing for other infections whenever an STD is diagnosed.
Data on the prevalence of gonococcal infection in children are sparse in the literature. According to Rawstron et al. (1993), studies carried out in the United States reported gonorrhea in 3% to 12% of sexually active adolescents of both genders. Around 25% of pre-adolescents affected were asymptomatic. 18
The risk of acquiring gonorrhea through sexual abuse depends on various factors, including the prevalence of this infection in the adult population. With the exception of perinatal infections, a diagnosis of gonorrhea in children is highly suggestive of sexual abuse, since there are no convincing data on any nonsexual forms of transmission. 8,18,19
With respect to the non-gonococcal infections found in this group, the possibility of Chlamydia trachomatis infection was considered. Data in the literature based on children who have suffered sexual abuse refer to the presence of this pathogen in around 3.3% of generally asymptomatic children. This diagnosis in children, albeit uncommon, may be a marker of sexual abuse once the possibility of perinatal transmission, in which the most common manifestations are conjunctivitis and pneumonia, has been eliminated. 13,20,21
Trichomoniasis is a common cause of vaginitis in adults and one of the most commonly acquired infections resulting from sexual abuse. Data in children are limited; however, the presence of this pathogen in this population is highly suggestive of sexual abuse. In the metaanalysis carried out by Beck-Sagué & Solomon (1999), trichomoniasis was found in approximately 9.4% of children following sexual abuse. Perinatal infection is probable and nonsexual transmission is theoretically possible. 13,15,22
Bacterial vaginosis (BV) in adult women is not classified as an STD; however, it may be triggered by sexual intercourse, through contact with semen with a high pH. It is one of the most common causes of vaginal discharge in adults and probably in children, and in this age group may be a sign of the initiation of sexual activity or abuse. Although data in children are limited, BV may be present in approximately 15-18.3% of victims of sexual abuse. 3,13,15 According to Argent & Lachman (1995), sexual abuse should be investigated following this diagnosis in prepuberal girls. 23
In cases of vulvovaginitis caused by Candida sp., sexual intercourse is not the principal form of transmission, since these organisms may form part of the endogenous flora in up to 50% of asymptomatic women. 5 There is controversy regarding its occurrence in children; however, according to Fischer (2001), since it is an estrogen-dependent condition, it is rare in childhood and may be classified merely as a contaminant in diaper dermatitis. 24 Nevertheless, it constituted the most common gynecological problem in children/adolescents in a large study conducted by Koumantakis et al. (1997). 25
Chancroid is an infection of exclusively sexual transmission. Its prevalence in adults is difficult to estimate and, although rare in children, may occur following sexual abuse. Pandhi et al. (2003) found chancroids in both boys and girls between the ages of 1014 group. 3
Acquired syphilis should be suspected in symptomatic or seropositive children in whom no evidence of congenital syphilis was documented. Almost always associated with sexual abuse, it therefore reflects the epidemiology of syphilis in adults. 18,26 In a study conducted by Beck-Sagué & Solomon (1999), 3.3% of patients were found to be infected following sexual abuse. 13 Nonsexual, perinatal or accidental transmission may occur; however, it is extremely rare. Condyloma planum was the clinical presentation found in the patient with secondary syphilis in the present study.
HIV infection may occur following sexual abuse and this form of transmission may be underestimated. 27 In a study conducted by Lindegren et al. (1998) with 9,136 HIV-positive children under 13 years of age, 26 had suffered sexual abuse. 28 It should be emphasized that the risk of transmission associated with ulcerated genital lesions highlights the importance of HIV testing in these cases. In the present study, two children were HIV-positive and in one of these cases the child's mother was also seropositive.
Genital herpes is a virus predominantly transmitted by sexual contact, the prevalence of which is increasing among adults. Transmission may also occur through direct contact with contaminated lesions or objects. Although the risk is unknown, children may become infected following sexual abuse, irrespective of viral type, and even by self-inoculation in the case of gingivostomatitis. 3,15
In cases of HPV infection in children, according to Reis et al. (2001), there is considerable evidence that lesions acquired after infancy are the result of sexual abuse. 27 On the other hand, although reports in the literature on cases of anogenital warts as a result of sexual abuse in children have cited prevalence rates ranging from 8% to 80%, the metaanalysis conducted by Beck-Sagué & Solomon (1999) considered that in the many studies published, only a minority of children presented warts following sexual abuse. In the majority of cases, HPV typing was not performed, although this would have reduced or even eliminated the possibility of sexual transmission if the presence of type 2 (cutaneous) HPV were found. 13 On the other hand, Hornor (2004) noted that viral typing may be inconclusive since types 1 and 2 (cutaneous) may be transmitted to the genitalia by selfinoculation, accidental inoculation or even by abusive manipulation. 29
Therefore, the presence of condyloma in children is not always a consequence of sexual abuse, since different forms of transmission have to be taken into account as well as the age of the child, the incubation period, the site of the lesion, the parents' history of genital warts, the presence of nongenital warts on the child and/or family members, the type of HPV and evidence of any changes in the psychosocial behavior of the child. 9,30
Diseases that are currently rare such as venereal lymphogranuloma and donovanosis were not found in this study population.
Conclusion
The importance of this initial, descriptive, epidemiological study should be emphasized. Although the findings cannot be extrapolated to the entire city of Manaus, they contribute to increasing knowledge on STDs in this age group. The frequencies and clinical characteristics of the STDs in the children in this study are similar to those found in the literature and, although the diagnosis of STD does not necessarily signal abuse, this possibility should always be taken into consideration. Other analytical studies are necessary to identify possible factors related to the vulnerability of the population in this age group to acquiring STD, correlating these factors with the possibility of sexual abuse. The results of these studies would aid in the planning, monitoring and evaluation of healthcare actions that may interfere in the dynamics of these infections.

REFERENCES
-
1Pitché P, Kombaté K, Gbadoé AD, Tchangaï-Walla K. Sexually transmitted diseases in young children in Lomé (Togo). Role of sexual abuse. Arch Pediatr. 2001;8:25-31.
-
2Olayinka AT, Olayinka BO. Sexually transmitted diseases in children, a cause for concern. J Trop Pediatr. 2002;48:316.
-
3Pandhi D, Kumar S, Reddy BSN. Sexually transmitted diseases in children. J Dermatol. 2003;30:314-20.
-
4Figueiredo PAL, Passos MRL, Pinheiro VMS, Barreto NA, Carvalho AVV, Bravo RS. Doenças sexualmente transmissíveis na infância: análise dos casos atendidos no Setor de DST/UFF no período de 1988 a 1996. DST J Bras Doenças Sex Transm. 1997;9:17-23.
-
5Tiburcio AS, Passos MRL, Pinheiro VMS. Epidemiologia das DST: perfis dos pacientes atendidos num centro Nacional de Treinamento. DST J Bras Doenças Sex Transm. 2000;12:4-39.
-
6Fagundes LJ, Patriota RCR, Gotlieb SLD. Avaliação da demanda no ambulatório de Doenças Sexualmente Transmissíveis do C. S. Geraldo de Paula Souza - Faculdade de Saúde Publica - USP, Brasil, no período de 1994 a 1998. An Bras Dermatol. 2001;76:223-32.
-
7Thomas A, Forster G, Robinson A, Rogstad K; Clinical Effectiveness Group Association of Genitourinary Medicine; Medical Society for the Study of Venereal Diseases. National guideline for the management of suspected sexually transmitted infections in children and young people. Arch Dis Child. 2003;88:303-11.
-
8Neinstein LS, Goldenring J, Carpenter S. Non sexual transmission of sexually transmitted diseases: an infrequent occurrence. Pediatrics. 1984;74:67-76.
-
9Estreich S, Foster GE. Sexually transmitted diseases in children: Introduction. Genitourin Med. 1992;68:2-8.
-
10Carvalho AVV, Passos MRL, Oliveira LHS, Lopes VGS, Herdy GVH, Pinheiro VMS. Sífilis adquirida na infância: estudo clínico, laboratorial e abuso sexual. DST J Bras Doenças Sex Transm. 1999;11:4-20.
-
11Sidra.ibge.gov [Internet]. Instituto Brasileiro de Geografia e Estatística. Censos Demográficos, 2000 [Acesso: 10 Ago. 2008]. Disponível em: http://www.sidra.ibge.gov.br/bda/tabela/protabl.asp?z=t&o=21&i=P
-
12Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Programa Nacional de DST e Aids. Prevalências e freqüências relativas de Doenças Sexualmente Transmissíveis (DST) em populações selecionadas de seis capitais brasileiras, 2005 / Ministério da Saúde, Secretaria de Vigilância em Saúde, Programa Nacional de DST e Aids. - Brasília: Ministério da Saúde, 2008.
-
13Beck-Sagué CM, Solomon F. Sexually transmitted diseases in abused children and adolescent and adult victims of rape: review of selected literature. Clin Infect Dis. 1999;28:S74-83.
-
14Williams O, Foster G, Robinson A. Screening for sexually transmitted infections in children and adolescents in the United Kingdom: British Co-operative Clinical Group. Int J STD AIDS. 2001;12:487-92.
-
15Hammerschlag MR. Sexually transmitted diseases in sexually abused children: medical and legal implications. Sex Transm Infect. 1998;74:167-74.
-
16Dispõe sobre o Estatuto da Criança e do Adolescente e dá outras providências. Lei nº. 8.069 (13 de julho de 1990). In: Diário Oficial da União. Brasília; 1990. p. 6054.
-
17Drezett J, Caballero M, Juliano Y, Prieto ET, Marques JA, Fernandes CE. Estudo de mecanismos e fatores relacionados com o abuso sexual em crianças e adolescentes do sexo feminino. J Pediatr (Rio J). 2001;77:413-9.
-
18Rawstron SA, Bromberg K, Hammerschlag MR. STD in children: syphilis and gonorrhoea. Genitourin Med. 1993;69:66-75.
-
19Goodyear-Smith F. What is the evidence for non-sexual transmission oh gonorrhoea in children after the neonatal period? A systematic review. J Forensic Leg Med. 2007;14:489-502.
-
20Hammerschlag MR. Chlamydial infection. J Pediatr. 1989;114:727-34.
-
21Darville T. Chlamydia trachomatis infections in neonates and young children. Seminar Pediatr Infect Dis. 2005;16:235-44.
-
22Thomason JL, Gelbart SM. Trichomonas vaginalis. Obstet Gynecol. 1989;74:536-41.
-
23Argent AC, Lachman PI, Hanslo D, Bass D. Sexually transmitted diseases in children and evidence of sexual abuse. Child Abuse Negl. 1995;19:1303-10.
-
24Fischer GO. Vulval disease in pre-pubertal girls. Australas J Dermatol. 2001;42:225-36.
-
25Koumantakis EE, Hassan EA, Deligeoroglou EK, Creatsas GK. Vulvovaginitis during childhood and adolescence. J Pediatr Adolesc Gynecol. 1997;10:39-43.
-
26Woods CR. Syphilis in children: congenital and acquired. Semin Pediatr Infect Dis. 2005;16:245-57.
-
27Reis JN, Martin CCS, Bueno SMV. Violência sexual, vulnerabilidade e doenças sexualmente transmissíveis. DST - J bras Doenças Sex Transm. 2001;13:40-5.
-
28Lindegren ML, Hanson IC, Hammet TA, Fleming PL, Ward JW. Sexual abuse of children: intersection with the HIV epidemic. Pediatrics. 1998;102:E46.
-
29Hornor G. Ano-genital warts in children: Sexual abuse or not? J Pediatr Health Care. 2004;18:165-70.
-
30Jones V, Smith SJ, Omar HA. Nonsexual transmission of anogenital warts in children: a retrospective analysis. Scientific World Journal. 2007;7:1896-9.
Publication Dates
-
Publication in this collection
21 Mar 2011 -
Date of issue
Feb 2011
History
-
Accepted
28 Feb 2010 -
Received
30 Sept 2009



