Abstract
PURPOSE:
To study racemic bupivacaine, non-racemic bupivacaine and ropivacaine on myocardial contractility.
METHODS:
Isolated Wistar papillary muscles were submitted to 50 and 100 mM racemic bupivacaine (B50 and B100), non-racemic bupivacaine (NR50 and NR100) and ropivacaine (R50 and R100) intoxication. Isometric contraction data were obtained in basal condition (0.2 Hz), after increasing the frequency of stimulation to 1.0 Hz and after 5, 10 and 15 min of local anesthetic intoxication. Data were analyzed as relative changes of variation.
RESULTS:
Developed tension was higher with R100 than B100 at D1 (4.3 ± 41.1 vs -57.9 ± 48.1). Resting tension was altered with B50 (-10.6 ± 23.8 vs -4.7 ± 5.0) and R50 (-14.0 ± 20.5 vs -0.5 ± 7.1) between D1 and D3. Maximum rate of tension development was lower with B100 (-56.6 ± 38.0) than R50 (-6.3 ± 37.9) and R100 (-1.9 ± 37.2) in D1. B50, B100 and NR100 modified the maximum rate of tension decline from D1 through D2. Time to peak tension was changed with NR50 between D1 and D2.
CONCLUSIONS:
Racemic bupivacaine depressed myocardial contractile force more than non-racemic bupivacaine and ropivacaine. Non-racemic and racemic bupivacaine caused myocardial relaxation impairment more than ropivacaine.
Anesthetics; Local; Cardiotoxicity; Papillary Muscles; Rats
Introduction
Local anesthetics (LA) cardiotoxicity has been one of the greatest concerns among
anesthesiologists since Albright's reports on cardiac arrest following regional
anesthesia11 Albright GA. Cardiac arrest following regional anesthesia with
etidocaine or bupivacaine. Anesthesiology. 1979 Oct;51(4):285-7. PMID:
484889.. LA cardiotoxic manifestations
include electrocardiographic (ECG) changes, hypotension and myocardial contractile
impairment22 Groban L, Dolinski SY. Differences in cardiac toxicity among
ropivacaine, levobupivacaine, bupivacaine and lidocaine. Tech Reg Anesth Pain Manag.
2001;5(2):48-55. doi: 10.1053/trap.2001.2379.
https://doi.org/10.1053/trap.2001.2379...
3 David JS, Amour J, Duracher C, Ferretti C, Precloux P, Petit P, Riou B,
Gueugniaud PY. Comparison of the effects of mepivacaine and lidocaine on rat
myocardium. Eur J Anaesthesiol. 2007 Feb;24(2):190-7. doi:
10.1017/S0265021506001359.
https://doi.org/10.1017/S026502150600135...
-
44 Butterworth JFt. Models and mechanisms of local anesthetic cardiac
toxicity: a review. Reg Anesth Pain Med. 2010 Mar-Apr;35(2):167-76. doi:
10.1097/AAP0b013e3181d231b9.
https://doi.org/10.1097/AAP0b013e3181d23...
. Many mechanisms have been described as LA
cardiotoxic effects like sodium channel blockade22 Groban L, Dolinski SY. Differences in cardiac toxicity among
ropivacaine, levobupivacaine, bupivacaine and lidocaine. Tech Reg Anesth Pain Manag.
2001;5(2):48-55. doi: 10.1053/trap.2001.2379.
https://doi.org/10.1053/trap.2001.2379...
, mitochondrial disfunction55 Hiller N, Mirtschink P, Merkel C, Knels L, Oertel R, Christ T, Deussen
A, Koch T, Stehr SN. Myocardial accumulation of bupivacaine and ropivacaine is
associated with reversible effects on mitochondria and reduced myocardial function.
Anesth Analg. 2013 Jan;116(1):83-92. doi:
10.1213/ANE.0b013e31826c8095.
https://doi.org/10.1213/ANE.0b013e31826c...
,
sarcolemmal injuries66 Tsuchiya H, Mizogami M. R(+)-, Rac-, and S(-)-bupivacaine
stereostructure-specifically interact with membrane lipids at cardiotoxically
relevant concentrations. Anesth Analg. 2012 Feb;114(2):310-2. doi:
10.1213/ANE.0b013e31823ed410.
https://doi.org/10.1213/ANE.0b013e31823e...
and calcium handling
impairment77 Chedid NG, Sudo RT, Aguiar MI, Trachez MM, Masuda MO, Zapata-Sudo G.
Regulation of intracellular calcium by bupivacaine isomers in cardiac myocytes from
Wistar rats. Anesth Analg. 2006 Mar;102(3):792-8. doi:
10.1213/01.ane.0000195341.65260.87.
https://doi.org/10.1213/01.ane.000019534...
.
LA chemical properties, such as lipid solubility and isomerism, have also been related
to LA cardiotoxic potential22 Groban L, Dolinski SY. Differences in cardiac toxicity among
ropivacaine, levobupivacaine, bupivacaine and lidocaine. Tech Reg Anesth Pain Manag.
2001;5(2):48-55. doi: 10.1053/trap.2001.2379.
https://doi.org/10.1053/trap.2001.2379...
,
88 David JS, Ferreti C, Amour J, Vivien B, Eve O, Petit P, Riou B,
Gueugniaud PY. Effects of bupivacaine, levobupivacaine and ropivacaine on myocardial
relaxation. Can J Anaesth. 2007 Mar;54(3):208-17. doi:
10.1007/BF03022642.
https://doi.org/10.1007/BF03022642...
. Isomerism is the phenomenon in which certain
compounds with the same molecular formula are different because of their atoms
organization. In optical isomerism, R and S enantiomers are the mirror image from each
other. Racemic bupivacaine is a solution composed by 50% R isomers and 50% S isomers.
Non-racemic bupivacaine has R and S isomers in a ration different from 1:1. It is well
known that bupivacaine R isomer has greater sodium channel affinity and induces ECG
changes more frequently than S(-)bupivacaine99 Vladimirov M, Nau C, Mok WM, Strichartz G. Potency of bupivacaine
stereoisomers tested in vitro and in vivo: biochemical, electrophysiological, and
neurobehavioral studies. Anesthesiology. 2000 Sep;93(3):744-55. PMID:
10969308.
,
1010 Valenzuela C, Snyders DJ, Bennett PB, Tamargo J, Hondeghem LM.
Stereoselective block of cardiac sodium channels by bupivacaine in guinea pig
ventricular myocytes. Circulation. 1995 Nov;92(10):3014-24. doi:
10.1161/01.CIR.92.10.3014. PMID: 7586272.. In addition, QRS time was increased with
racemic bupivacaine compared to ropivacaine and S(-)bupivacaine1111 Morrison SG, Dominguez JJ, Frascarolo P, Reiz S. A comparison of the
electrocardiographic cardiotoxic effects of racemic bupivacaine, levobupivacaine, and
ropivacaine in anesthetized swine. Anesth Analg. 2000 Jun;90(6):1308-14. PMID:
10825311..
LA isomers also have different effects on myocardial contractile function. Racemic
bupivacaine was more potent than ropivacaine in reducing guinea pig isolated heart
inotropism55 Hiller N, Mirtschink P, Merkel C, Knels L, Oertel R, Christ T, Deussen
A, Koch T, Stehr SN. Myocardial accumulation of bupivacaine and ropivacaine is
associated with reversible effects on mitochondria and reduced myocardial function.
Anesth Analg. 2013 Jan;116(1):83-92. doi:
10.1213/ANE.0b013e31826c8095.
https://doi.org/10.1213/ANE.0b013e31826c...
. Bupivacaine had greater negative
inotropic effects than ropivacaine in isolated guinea pig heart, besides no differences
between R and S isomers were noted1212 Graf BM, Abraham I, Eberbach N, Kunst G, Stowe DF, Martin E. Differences
in cardiotoxicity of bupivacaine and ropivacaine are the result of physicochemical
and stereoselective properties. Anesthesiology. 2002 Jun;96(6):1427-34. PMID:
12170056..
S(-)bupivacaine depressed rat papillary muscle relaxation more than racemic bupivacaine
and ropivacaine88 David JS, Ferreti C, Amour J, Vivien B, Eve O, Petit P, Riou B,
Gueugniaud PY. Effects of bupivacaine, levobupivacaine and ropivacaine on myocardial
relaxation. Can J Anaesth. 2007 Mar;54(3):208-17. doi:
10.1007/BF03022642.
https://doi.org/10.1007/BF03022642...
.
Different LA enantiomeric preparations have been studied as a way to improve clinical
outcomes without cardiotoxic effects. Adding 25% of the R isomer to S(-)bupivacaine
(S75/R25) promoted stronger muscle relaxation and motor nerve blockade than bupivacaine
isomers alone1313 Trachez MM, Zapata-Sudo G, Moreira OR, Chedid NG, Russo VF, Russo EM,
Sudo RT. Motor nerve blockade potency and toxicity of non-racemic bupivacaine in
rats. Acta Anaesthesiol Scand. 2005 Jan;49(1):66-71. doi:
10.1111/j.1399-6576.2004.00536.x.
https://doi.org/10.1111/j.1399-6576.2004...
. However, the effects of
non-racemic bupivacaine (S75/R25) on myocardial contractile function remain
understudied. Thus, the aim of this investigation was to compare the effects of
non-racemic bupivacaine, racemic bupivacaine and ropivacaine at equimolar concentrations
on the rat myocardial contractile function. The hypothesis was non-racemic bupivacaine
had an intermediary cardiotoxic potential compared to racemic bupivacaine and
ropivacaine.
Methods
This investigation was performed in accordance with the Guide for the Care and Use of Laboratory Animals, issued by the United States National Institutes of Health and was approved by the institutional Animal Care and use Committee (Protocol number 754/2009).
Sixty-day-old male Wistar rats weighing 280-300g were used. Forty two animals were randomly and equally distributed in six groups: intoxication with racemic bupivacaine 50 mM (B50), intoxication with racemic bupivacaine 100 mM (B100), intoxication with non-racemic bupivacaine 50 mM (NR50), intoxication with non-racemic bupivacaine 100 mM (NR100), intoxication with ropivacaine 50 mM (R50), and intoxication with ropivacaine 100 mM (R100). LA were provided by Cristália Produtos Químicos e Farmacêuticos LTDA, Itapira-SP, Brazil. Cristália was not involved in the study design neither its results and conclusions.
Papillary muscle mechanical study
At the time of the study, rats were anesthetized with sodium penthobarbital 50 mg.kg-1 intraperitoneally and killed by decapitation. Their hearts were quickly removed and placed in oxygenated Krebs-Henseleit solution (118.5 mM NaCl, 4.69 mM KCl, 2.5 mM CaCl2, 1.16 mM MgSO4, 1.18 mM KH2PO4, 24.88 mM NaCO3 and 5.5 mM glucose) at 28°C. Papillary muscles from the left ventricle were carefully dissected, mounted between two spring clips and placed vertically in a chamber containing 50 mL Krebs-Henseleit solution. The perfusate PO2 was maintained between 550 and 600 mmHg by passing 95% O2 and 5% CO2 through sintered glass discs located at the bottom of the chamber. Temperature was maintained at 28°C with a recirculating bath (Refrigerating/Heating -20°C to 150°C, PolyScience Division of Peston Industries, Niles, IL, USA). The lower spring clip was attached to a force transducer (Grass FT03 Force Displacement Transducer, GRASS Technologies, West Warwick, RI, USA), which passed through a mercury seal at the bottom of the chamber, avoiding friction between the transducer and the chamber. The upper spring clip was connected by a thin steel wire to a rigid lever arm above which a micrometer stop (L.S. Starret Company, Athol, MA, USA) was mounted for the adjustment of muscle strength. The lever arm was made of magnesium with a ball-bearing fulcrum and a lever arm ratio of 4:1. A 5g preload was mounted at the lever to promote initial papillary muscle stretch. Preparations were stimulated 12 times/min (0.2 Hz) with a 5 ms square wave pulses through parallel platinum electrodes at voltages that were 10% greater than the minimum required to produce a maximal mechanical response.
After 60 min stabilizing period, during which preparations were allowed to shorten while carrying light loads, the 5g load was increased to 50g load, which allowed muscles to contract isometrically. After 15 min, papillary muscles were gradually stretched using the micrometer, until maximum tension development. Papillary muscle length relative to maximum tension development (Lmax) was measured between spring clips with a cathetometer (Gartner, Gartner Scientific Corporation, Chicago, IL, USA). Papillary muscles were maintained in isometric contraction and mechanical data were initially obtained (basal condition). Frequency of stimulation was progressively increased to 60 times/min (1.0 Hz) and mechanical data were obtained from papillary muscles in isometric contraction at Lmax after 30 min (M0). Local anesthetic was added to the papillary muscle preparations and posterior mechanical data were obtained in isometric contraction at Lmax after 5, 10 and 15 min (M1, M2 and M3, respectively).
At the end of each experiment, papillary muscles between both spring clips were blotted, dried and weighed. Cross-sectional area (CSA) was calculated from muscle weigh (MW) and length at Lmax by assuming cylindrical uniformity and specific gravity of 1.0 (CSA = MW. Lmax -1).
Functional study
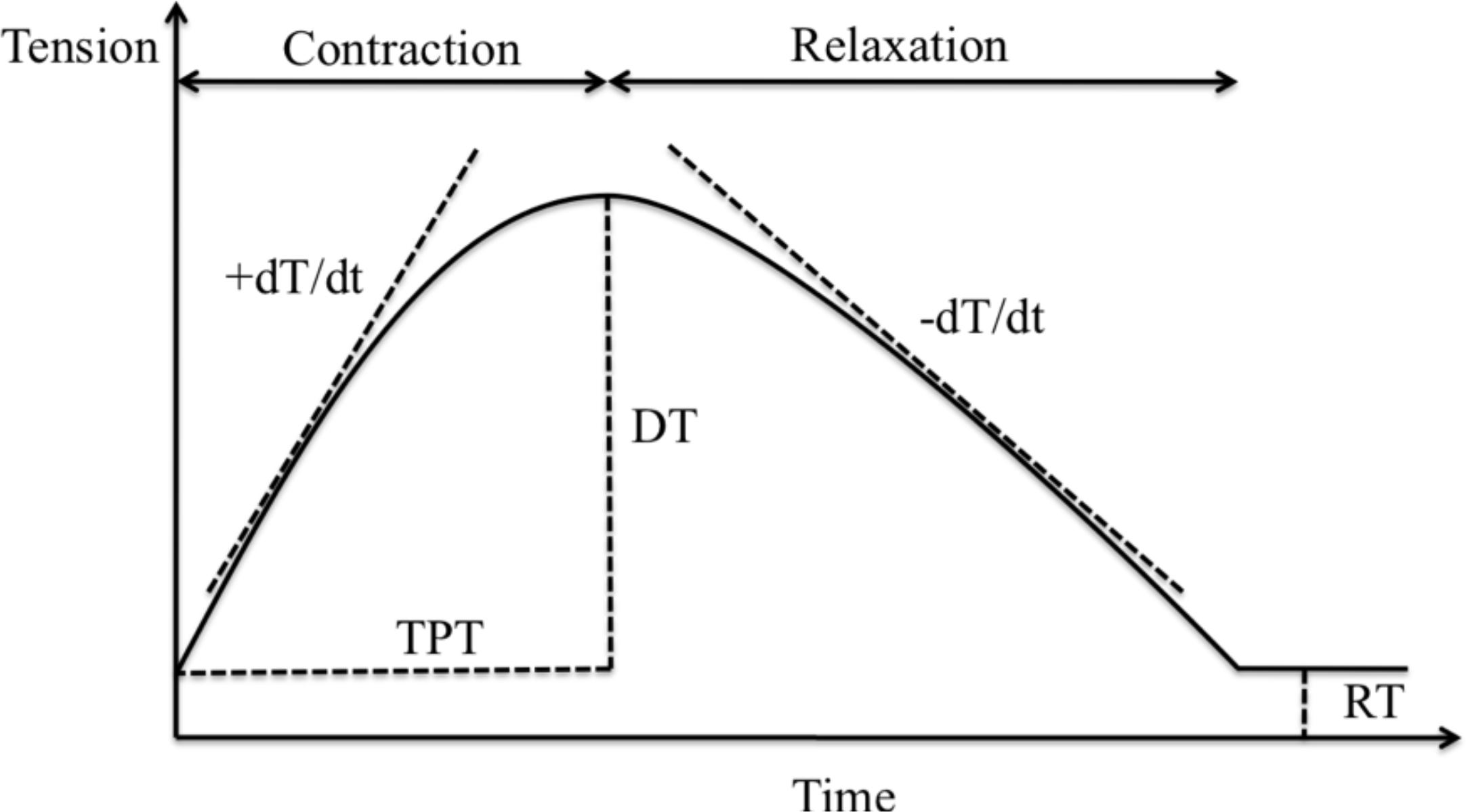
Mechanical parameters were measured in isometric contraction at Lmax and were registered in a computer system (AcqKnowledgeTM MP 100, Biopac Systems Inc., Santa Barbara, CA, USA). Isometric contraction curves (Figure 1) were analyzed to determine the mechanical parameters: developed tension (DT, g.mm-2), resting tension (RT, g.mm-2), maximum rate of tension development (+dT/dt, g.mm-2.s-1), maximum rate of tension decline (-dT/dt, g.mm-2.s-1) and time to peak tension (TPT, ms). Data were obtained with a frequency of stimulation of 0.2 Hz (basal condition) and 1.0 Hz (M0) without local anesthetics and after 5 (M1), 10 (M2) and 15 min (M3) of LA addition. All mechanical data were normalized for the muscle CSA to compare the performance of different muscles.
Papillary muscle isometric contraction curve. DT: developed tension; RT: resting tension; +dT/dt: maximum rate of tension development; -dT/dt: maximum rate of tension decline; TPT: time to peak tension.
LA effects were better evaluated using the percentage of variation (%) in relation to the preceding measure for all mechanical parameters calculated as follows: D1 = (M1 - M0) x M0-1 x 100; D2 = (M2 - M1) x M1-1 x 100 and D3 = (M3 - M2) x M2-1 x 100.
Statistical analysis
Values are shown as mean ± standard deviation for normal distribution and median ± interquartile-range for non-normal distribution. Mechanical data in basal conditions (0.2 Hz) and after increasing the frequency of stimulation to 1.0 Hz (M0) were compared using two-way analysis of variance (ANOVA) followed by Tukey test. LA effects were presented as relative change (%) from the previous measure (D1, D2 and D3) and were compared using the Kruskal-Wallis one way analysis of variance followed by Dunn's test if p<0.05. The level of significance considered was 5% (p<0.05).
Results
Two papillary muscles stopped beating at M3 with racemic bupivacaine 50 mM and one papillary muscle stopped beating at M4 with racemic bupivacaine 100 mM; non-racemic bupivacaine 50 mM induced one papillary muscle arrest at M3. One papillary muscle stopped beating after adding ropivacaine 50 mM at M2. Data from papillary muscles that stopped beating anytime during the experiment were discarded. Data from 38 papillary muscles in isometric contraction were analyzed according to the group distribution as follows: B50 (n=5), B100 (n=6), NR50 (n=7), NR100 (n=7), R50 (n=6), and R100 (n=7). Mechanical data with frequency of stimulation of 0.2 Hz and 1.0 Hz were not different among groups (ANOVA, Tukey test).
Figure 2 shows DT oscillation with LA effect. DT variation was different between D1 and D3 in B100 (-57.9 ± 48.1 vs -2.3 ± 13.8, p=0.04) and between D1 and D2 in R50 (-6.6 ± 27.6 vs 4.4 ± 6.9, p=0.03).
Developed tension (DT) percentage of variation in different groups and moments. Values are median ± semi-range. B50: papillary muscles intoxicated with racemic bupivacaine 50 mM; B100: papillary muscles intoxicated with racemic bupivacaine 100 mM; NR50: papillary muscles intoxicated with non-racemic bupivacaine 50 mM; NR100: papillary muscles intoxicated with non-racemic bupivacaine 100 mM; R50: papillary muscles intoxicated with ropivacaine 50 mM; R100: papillary muscles intoxicated with ropivacaine 100 mM. D1: variation from M1 in relation to M0; D2: variation from M2 in relation to M1; D3: variation from M3 in relation to M2. * B100 vs R100 (p=0.02); # D1 vs D3 (p=0.04); § D1 vs D2 (p=0.03). Kruskal-Wallis and Dunn's test.
There were no differences among moments in B50, NR50, NR100 and R100. B100 caused a higher oscillation in DT than R100 in D1 (-57.9 ± 48.1 vs 4.3 ± 41.1, p=0.02). There were no differences among groups in D2 and D3.
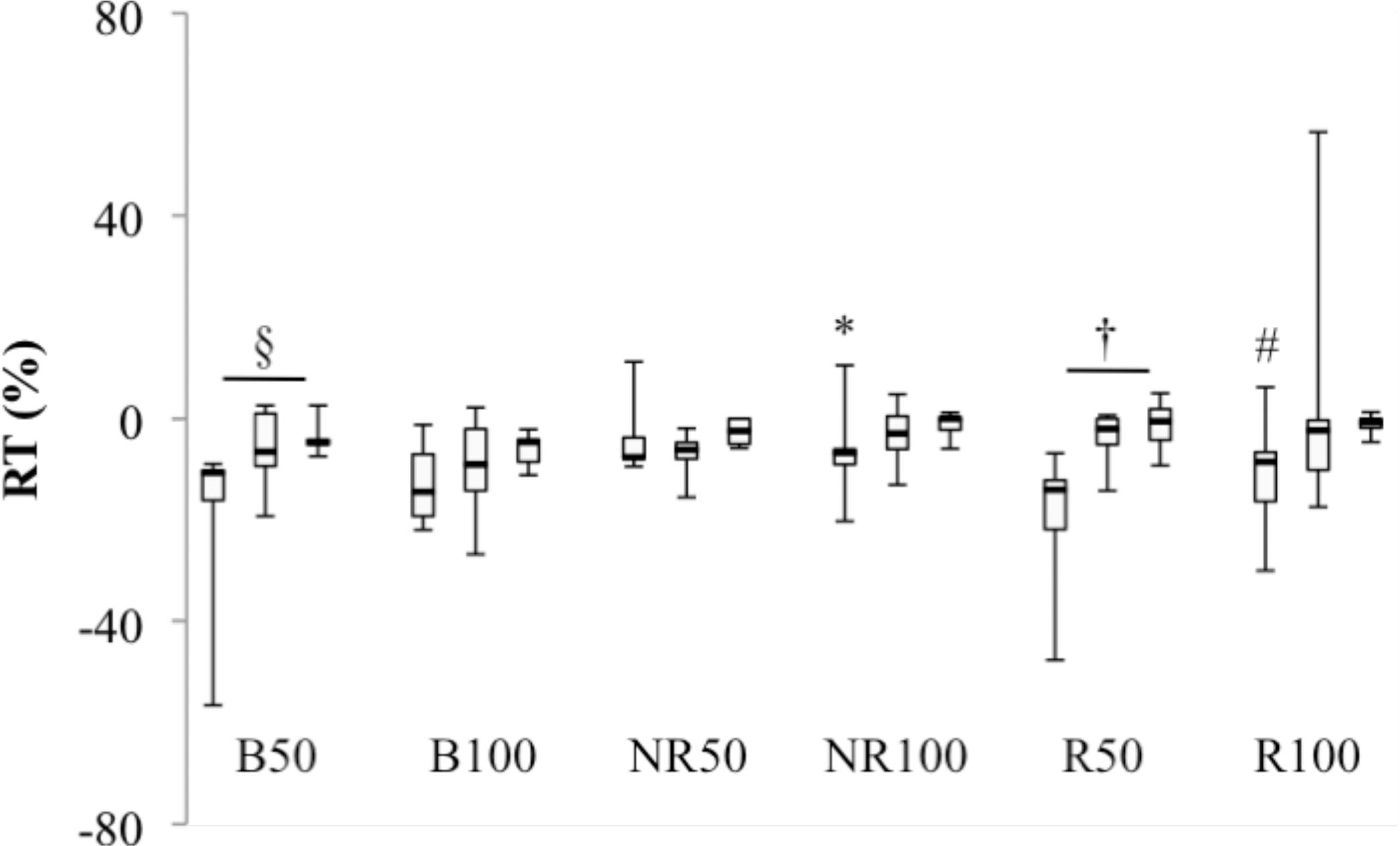
Figure 3 shows RT variation with LA. RT decrease was higher in D1 compared to D3 in B50 (-10.6 ± 23.8 vs -4.7 ± 5.0, p=0.03) and R50 (-14.0 ± 20.5 vs -0.5 ± 7.1, p=0.009).
Resting tension (RT) percentage of variation in different groups and moments. Values are median ± semi-range. B50: papillary muscles intoxicated with racemic bupivacaine 50 mM; B100: papillary muscles intoxicated with racemic bupivacaine 100 mM; NR50: papillary muscles intoxicated with non-racemic bupivacaine 50 mM; NR100: papillary muscles intoxicated with non-racemic bupivacaine 100 mM; R50: papillary muscles intoxicated with ropivacaine 50 mM; R100: papillary muscles intoxicated with ropivacaine 100 mM. D1: variation from M1 in relation to M0; D2: variation from M2 in relation to M1; D3: variation from M3 in relation to M2. * NR100 vs B50, B100, NR50 and R50 (p=0.02); # R100 vs B50, B100 and NR50 (p=0.02); § D1 vs D3 (p=0.03); † D1 vs D3 (p=0.009). Kruskal-Wallis and Dunn's test.
There were no differences among moments in B100, NR50, NR100 and R100. RT varied less with NR100 (-6.7 ± 15.4) in relation to B50 (-10.6 ± 23.8), B100 (-14.4 ± 10.3), NR50 (-7.5 ± 10.3) and R50 (-14.0 ± 20.5) in D1 (p=0.02). The same situation is observed with R100 (-8.5 ± 18.1) compared to B50 (-10.6 ± 23.8), B100 (-14.4 ± 10.3) and NR50 (-7.5 ± 10.3) in D1 (p=0.02). There were no differences among groups in D2 and D3.
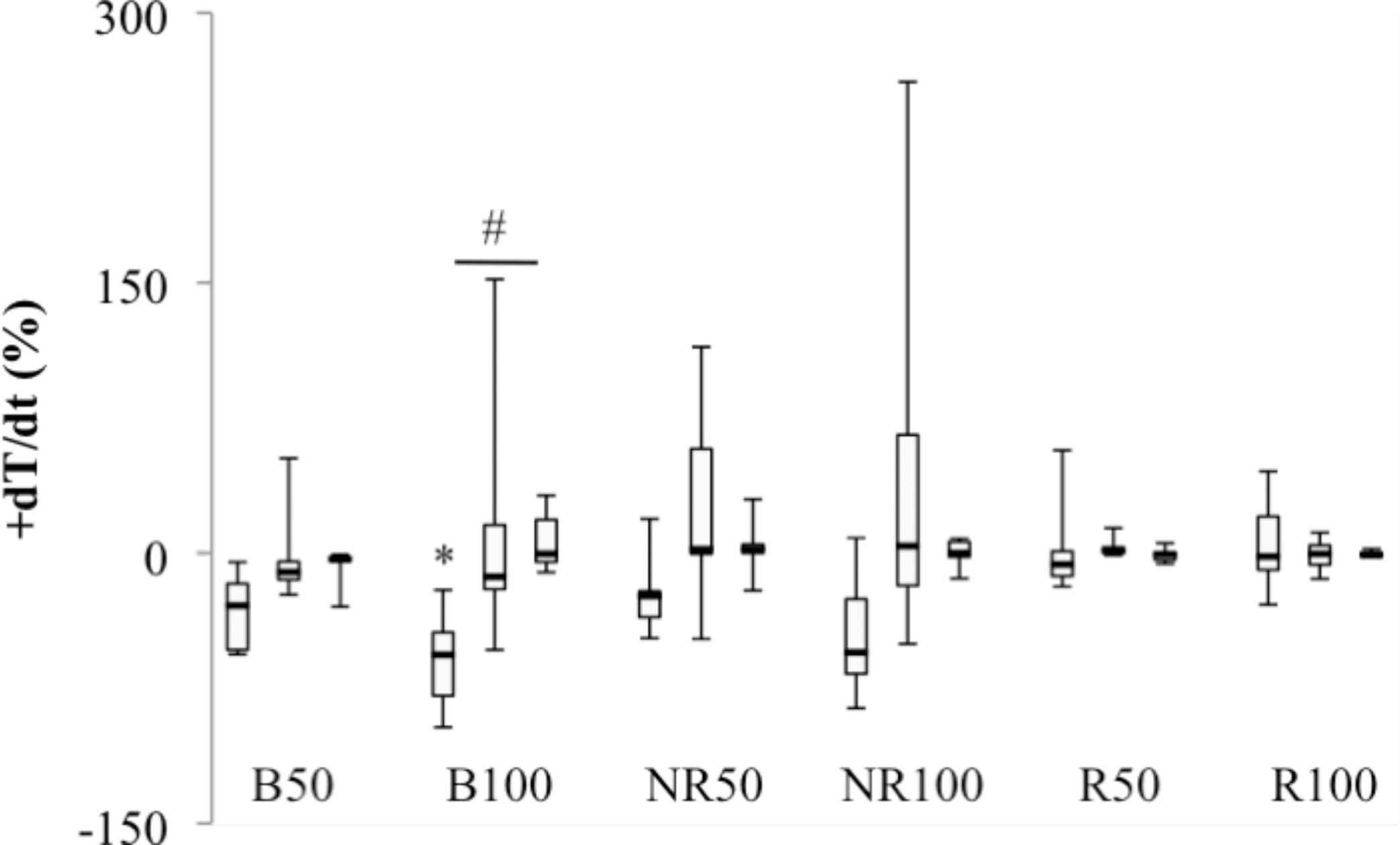
+dT/dt relative variation was different between D1 and D3 in B100 (-56.6 ± 38.0 vs -0.4 ± 21.4, p=0.007). There were no differences among moments in B50, NR50, NR100, R50 and R100. B100 (-56.6 ± 38.0) caused a higher decrease in +dT/dt than R50 (-6.3 ± 37.9) and R100 (-1.9 ± 37.2) in D1 (p=0.005). There were no differences among groups in D2 and D3 (Figure 4).
Maximum rate of tension development (+dT/dt) percentage of variation in different groups and moments. Values are median ± semi-range. B50: papillary muscles intoxicated with racemic bupivacaine 50 mM; B100: papillary muscles intoxicated with racemic bupivacaine 100 mM; NR50: papillary muscles intoxicated with non-racemic bupivacaine 50 mM; NR100: papillary muscles intoxicated with non-racemic bupivacaine 100 mM; R50: papillary muscles intoxicated with ropivacaine 50 mM; R100: papillary muscles intoxicated with ropivacaine 100 mM. D1: variation from M1 in relation to M0; D2: variation from M2 in relation to M1; D3: variation from M3 in relation to M2. * B100 vs R50 and R100 (p=0.005); # D1 vs D3 (p=0.007). Kruskal-Wallis and Dunn's test.
Figure 5 shows -dT/dt variation with LA. D1 was different from D2 and D3 in B50 (-33.5 ± 22.2 vs -4.5 ± 39.1 and -3.9 ± 23.5, p=0.03), B100 (-56.3 ± 31.6 vs -11.9 ± 107.5 and -1.5 ± 11.8, p=0.003) and NR100 (-50.0 ± 45.5 vs 1.9 ± 102.4 and 4.7 ± 4.2, p=0.008). NR50, R50 and R100 did not cause -dT/dt oscillation among moments. -dT/dt variation was more important in B100 (-56.3 ± 31.6) compared to R50 (1.7 ± 56.4) and R100 (0.0 ± 37.9) in D1 (p=0.001). R50 (1.7 ± 56.4) was also lower than NR100 (-50.0 ± 45.5) in D1 (p=0.001). There were no differences among groups in D2 and D3.
Maximum rate of tension decline (-dT/dt) percentage of variation in different groups and moments. Values are median ± semirange. B50: papillary muscles intoxicated with racemic bupivacaine 50 mM; B100: papillary muscles intoxicated with racemic bupivacaine 100 mM; NR50: papillary muscles intoxicated with non-racemic bupivacaine 50 mM; NR100: papillary muscles intoxicated with nonracemic bupivacaine 100 mM; R50: papillary muscles intoxicated with ropivacaine 50 mM; R100: papillary muscles intoxicated with ropivacaine 100 mM. D1: variation from M1 in relation to M0; D2: variation from M2 in relation to M1; D3: variation from M3 in relation to M2. * B100 vs R50 and R100 (p=0.001); # R50 vs B100 and NR50 (p=0.001); § D1 vs D2 and D3 (p=0.03); † D1 vs D2 and D3 (p=0.003); ? D1 vs D2 and D3 (p=0.008). Kruskal-Wallis and Dunn's test.
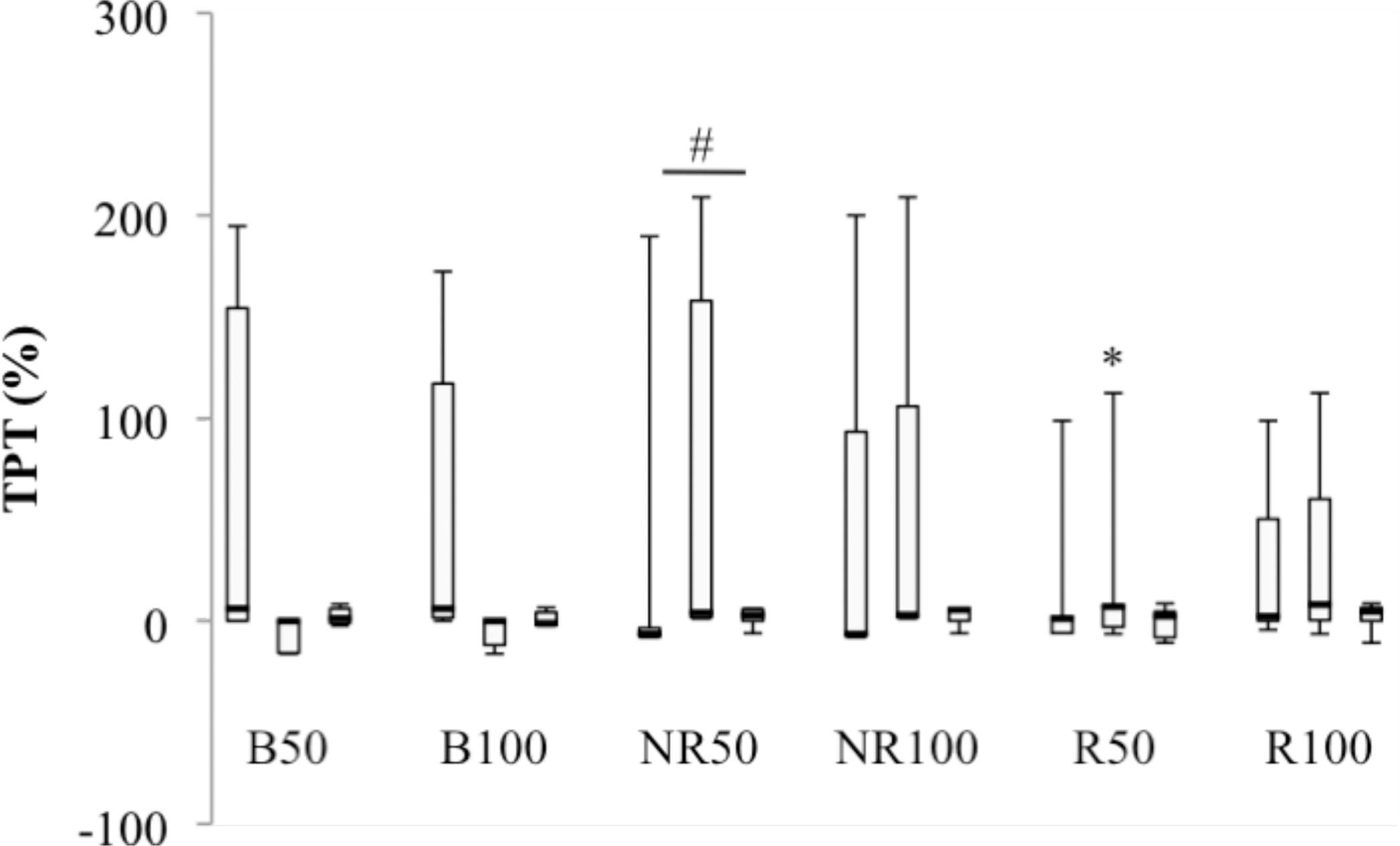
Figure 6 shows the TPT oscillation among groups and moments with LA. D1 was different from D2 with NR50 (-6.5 ± 98.9 vs 4.0 ± 103.9, p=0.04).
Time to peak tension (TPT) percentage of variation in different groups and moments. Values are median ± semi-range. B50: papillary muscles intoxicated with racemic bupivacaine 50 mM; B100: papillary muscles intoxicated with racemic bupivacaine 100 mM; NR50: papillary muscles intoxicated with non-racemic bupivacaine 50 mM; NR100: papillary muscles intoxicated with non-racemic bupivacaine 100 mM; R50: papillary muscles intoxicated with ropivacaine 50 mM; R100: papillary muscles intoxicated with ropivacaine 100 mM. D1: variation from M1 in relation to M0; D2: variation from M2 in relation to M1; D3: variation from M3 in relation to M2. * R50 and R100 vs B50, B100, NR50 and NR100 (p=0.009); # D1 vs D2 (p=0.04). Kruskal-Wallis and Dunn's test.
There were no differences among moments in B50, B100, NR100, R50 and R100. TPT oscillation was higher with R50 (7.0 ± 59.4) and R100 (8.0 ± 59.4) compared to B50 (0.0 ± 8.2), B100 (0.0 ± 8.2), NR50 (4.0 ± 103.9) and NR100 (2.9 ± 103.8) in D2 (p=0.009). There were no differences in TPT variation among groups in D1 and D3.
Discussion
Our results demonstrate that high concentrations racemic bupivacaine impaired myocardial contractile function more than non-racemic bupivacaine and ropivacaine. In addition, high doses of racemic and non-racemic bupivacaine and low doses of racemic bupivacaine caused papillary muscle relaxation impairment compared to ropivacaine.
There is a widespread number of experimental models and methods applied to evaluate the
myocardial contractile function, but isolated papillary muscle preparation is a way to
measure the ability of the cardiac muscle to develop force independent of influences
that can modify mechanical myocardial performance in vivo, such as heart rate, preload
and afterload44 Butterworth JFt. Models and mechanisms of local anesthetic cardiac
toxicity: a review. Reg Anesth Pain Med. 2010 Mar-Apr;35(2):167-76. doi:
10.1097/AAP0b013e3181d231b9.
https://doi.org/10.1097/AAP0b013e3181d23...
.
The present study confirmed the myocardial contractile dysfunction caused by potent
LA22 Groban L, Dolinski SY. Differences in cardiac toxicity among
ropivacaine, levobupivacaine, bupivacaine and lidocaine. Tech Reg Anesth Pain Manag.
2001;5(2):48-55. doi: 10.1053/trap.2001.2379.
https://doi.org/10.1053/trap.2001.2379...
,
88 David JS, Ferreti C, Amour J, Vivien B, Eve O, Petit P, Riou B,
Gueugniaud PY. Effects of bupivacaine, levobupivacaine and ropivacaine on myocardial
relaxation. Can J Anaesth. 2007 Mar;54(3):208-17. doi:
10.1007/BF03022642.
https://doi.org/10.1007/BF03022642...
,
1313 Trachez MM, Zapata-Sudo G, Moreira OR, Chedid NG, Russo VF, Russo EM,
Sudo RT. Motor nerve blockade potency and toxicity of non-racemic bupivacaine in
rats. Acta Anaesthesiol Scand. 2005 Jan;49(1):66-71. doi:
10.1111/j.1399-6576.2004.00536.x.
https://doi.org/10.1111/j.1399-6576.2004...
,
1414 Mio Y, Fukuda N, Kusakari Y, Tanifuji Y, Kurihara S. Bupivacaine
attenuates contractility by decreasing sensitivity of myofilaments to Ca2+ in rat
ventricular muscle. Anesthesiology. 2002 Nov;97(5):1168-77. PMID:
12411803.. Developed tension and maximum rate of tension
development were both decreased more intensely with 100 mM racemic bupivacaine in
relation to other LA in this study (Figures 2 and
4). Previous researches demonstrated racemic
bupivacaine had major impact to cause developed tension decrease in relation to other
LA22 Groban L, Dolinski SY. Differences in cardiac toxicity among
ropivacaine, levobupivacaine, bupivacaine and lidocaine. Tech Reg Anesth Pain Manag.
2001;5(2):48-55. doi: 10.1053/trap.2001.2379.
https://doi.org/10.1053/trap.2001.2379...
,
1414 Mio Y, Fukuda N, Kusakari Y, Tanifuji Y, Kurihara S. Bupivacaine
attenuates contractility by decreasing sensitivity of myofilaments to Ca2+ in rat
ventricular muscle. Anesthesiology. 2002 Nov;97(5):1168-77. PMID:
12411803.. Maximum rate of tension decline was affected
with both racemic bupivacaine concentrations and with 100 mM non-racemic bupivacaine
(Figure 5). It is important to note that only
75% of S(-)bupivacaine had the same effect of pure levobupivacaine in the myocardial
relaxation as previously reported in equimolar concentrations88 David JS, Ferreti C, Amour J, Vivien B, Eve O, Petit P, Riou B,
Gueugniaud PY. Effects of bupivacaine, levobupivacaine and ropivacaine on myocardial
relaxation. Can J Anaesth. 2007 Mar;54(3):208-17. doi:
10.1007/BF03022642.
https://doi.org/10.1007/BF03022642...
. Ropivacaine did not impair the myocardial function compared to
racemic and non-racemic bupivacaine in this study. Preceding researchers reported
equimolar concentrations of ropivacaine had the same negative inotropic effect of
racemic bupivacaine and levobupivacaine88 David JS, Ferreti C, Amour J, Vivien B, Eve O, Petit P, Riou B,
Gueugniaud PY. Effects of bupivacaine, levobupivacaine and ropivacaine on myocardial
relaxation. Can J Anaesth. 2007 Mar;54(3):208-17. doi:
10.1007/BF03022642.
https://doi.org/10.1007/BF03022642...
.
Previous studies demonstrated negative inotropic effects with different LA88 David JS, Ferreti C, Amour J, Vivien B, Eve O, Petit P, Riou B,
Gueugniaud PY. Effects of bupivacaine, levobupivacaine and ropivacaine on myocardial
relaxation. Can J Anaesth. 2007 Mar;54(3):208-17. doi:
10.1007/BF03022642.
https://doi.org/10.1007/BF03022642...
,
1313 Trachez MM, Zapata-Sudo G, Moreira OR, Chedid NG, Russo VF, Russo EM,
Sudo RT. Motor nerve blockade potency and toxicity of non-racemic bupivacaine in
rats. Acta Anaesthesiol Scand. 2005 Jan;49(1):66-71. doi:
10.1111/j.1399-6576.2004.00536.x.
https://doi.org/10.1111/j.1399-6576.2004...
14 Mio Y, Fukuda N, Kusakari Y, Tanifuji Y, Kurihara S. Bupivacaine
attenuates contractility by decreasing sensitivity of myofilaments to Ca2+ in rat
ventricular muscle. Anesthesiology. 2002 Nov;97(5):1168-77. PMID:
12411803.
-
1515 Szentandrassy N, Szabo A, Almassy J, Jona I, Horvath B, Szabo G, Banyasz
T, Marton I, Nanasi PP, Magyar J. Effects of articaine and ropivacaine on calcium
handling and contractility in canine ventricular myocardium. Eur J Anaesthesiol. 2010
Feb;27(2):153-61. doi: 10.1097/EJA.0b013e328331a37b.
https://doi.org/10.1097/EJA.0b013e328331...
. Divergent LA concentrations were described to
induce myocardial contractile function impairment. While 10 mM racemic bupivacaine
decreased DT values in rat ventricular muscle1414 Mio Y, Fukuda N, Kusakari Y, Tanifuji Y, Kurihara S. Bupivacaine
attenuates contractility by decreasing sensitivity of myofilaments to Ca2+ in rat
ventricular muscle. Anesthesiology. 2002 Nov;97(5):1168-77. PMID:
12411803.,
other authors have found that 0.5 mM racemic bupivacaine caused myocardial contractile
dysfunction1313 Trachez MM, Zapata-Sudo G, Moreira OR, Chedid NG, Russo VF, Russo EM,
Sudo RT. Motor nerve blockade potency and toxicity of non-racemic bupivacaine in
rats. Acta Anaesthesiol Scand. 2005 Jan;49(1):66-71. doi:
10.1111/j.1399-6576.2004.00536.x.
https://doi.org/10.1111/j.1399-6576.2004...
. Besides, non-racemic
bupivacaine had the maximal contractility impairment at 20 mM1313 Trachez MM, Zapata-Sudo G, Moreira OR, Chedid NG, Russo VF, Russo EM,
Sudo RT. Motor nerve blockade potency and toxicity of non-racemic bupivacaine in
rats. Acta Anaesthesiol Scand. 2005 Jan;49(1):66-71. doi:
10.1111/j.1399-6576.2004.00536.x.
https://doi.org/10.1111/j.1399-6576.2004...
. Ropivacaine has been reported to cause negative inotropic
effects with 100 to 1.000 mM1515 Szentandrassy N, Szabo A, Almassy J, Jona I, Horvath B, Szabo G, Banyasz
T, Marton I, Nanasi PP, Magyar J. Effects of articaine and ropivacaine on calcium
handling and contractility in canine ventricular myocardium. Eur J Anaesthesiol. 2010
Feb;27(2):153-61. doi: 10.1097/EJA.0b013e328331a37b.
https://doi.org/10.1097/EJA.0b013e328331...
. Myocardial
relaxation was also impaired by LA88 David JS, Ferreti C, Amour J, Vivien B, Eve O, Petit P, Riou B,
Gueugniaud PY. Effects of bupivacaine, levobupivacaine and ropivacaine on myocardial
relaxation. Can J Anaesth. 2007 Mar;54(3):208-17. doi:
10.1007/BF03022642.
https://doi.org/10.1007/BF03022642...
. Racemic
bupivacaine, S(-)bupivacaine and ropivacaine caused rat papillary muscle relaxation
dysfunction88 David JS, Ferreti C, Amour J, Vivien B, Eve O, Petit P, Riou B,
Gueugniaud PY. Effects of bupivacaine, levobupivacaine and ropivacaine on myocardial
relaxation. Can J Anaesth. 2007 Mar;54(3):208-17. doi:
10.1007/BF03022642.
https://doi.org/10.1007/BF03022642...
. Differences among LA
concentrations causing myocardial contractile harm could be understood by divergent
frequencies of stimulation used in the experiments88 David JS, Ferreti C, Amour J, Vivien B, Eve O, Petit P, Riou B,
Gueugniaud PY. Effects of bupivacaine, levobupivacaine and ropivacaine on myocardial
relaxation. Can J Anaesth. 2007 Mar;54(3):208-17. doi:
10.1007/BF03022642.
https://doi.org/10.1007/BF03022642...
. As LA blockade is called phasic, when decreasing frequency of stimulation
LA concentration should be increased to obtain the same effect44 Butterworth JFt. Models and mechanisms of local anesthetic cardiac
toxicity: a review. Reg Anesth Pain Med. 2010 Mar-Apr;35(2):167-76. doi:
10.1097/AAP0b013e3181d231b9.
https://doi.org/10.1097/AAP0b013e3181d23...
,
1616 Mulroy MF. Systemic toxicity and cardiotoxicity from local anesthetics:
incidence and preventive measures. Reg Anesth Pain Med. 2002 Nov-Dec;27(6):556-61.
PMID: 12430104.. In the present study, myocardial performance
was impaired with LA concentrations 20 times less than previous researches, however,
with papillary muscle frequency of stimulation 5 times superior88 David JS, Ferreti C, Amour J, Vivien B, Eve O, Petit P, Riou B,
Gueugniaud PY. Effects of bupivacaine, levobupivacaine and ropivacaine on myocardial
relaxation. Can J Anaesth. 2007 Mar;54(3):208-17. doi:
10.1007/BF03022642.
https://doi.org/10.1007/BF03022642...
. The same authors have reported that increasing the frequency of
stimulation with the same LA concentration increases the LA negative inotropic effect,
which returned to baseline after reducing the frequency of stimulation to initial
conditions88 David JS, Ferreti C, Amour J, Vivien B, Eve O, Petit P, Riou B,
Gueugniaud PY. Effects of bupivacaine, levobupivacaine and ropivacaine on myocardial
relaxation. Can J Anaesth. 2007 Mar;54(3):208-17. doi:
10.1007/BF03022642.
https://doi.org/10.1007/BF03022642...
.
Experiments demonstrated the importance of isomerism to improve drugs safety. Myocardial
performance impairment was increased with racemic bupivacaine and R(+)bupivacaine
compared to S(-)bupivacaine and non-racemic bupivacaine1313 Trachez MM, Zapata-Sudo G, Moreira OR, Chedid NG, Russo VF, Russo EM,
Sudo RT. Motor nerve blockade potency and toxicity of non-racemic bupivacaine in
rats. Acta Anaesthesiol Scand. 2005 Jan;49(1):66-71. doi:
10.1111/j.1399-6576.2004.00536.x.
https://doi.org/10.1111/j.1399-6576.2004...
. Even though LA cardiotoxicity has been widely described and R(+) isomer
cardiotoxic potential is frequently reported as more important than S(-),
S(-)bupivacaine had more consequences to myocardial relaxation than racemic bupivacaine
and ropivacaine88 David JS, Ferreti C, Amour J, Vivien B, Eve O, Petit P, Riou B,
Gueugniaud PY. Effects of bupivacaine, levobupivacaine and ropivacaine on myocardial
relaxation. Can J Anaesth. 2007 Mar;54(3):208-17. doi:
10.1007/BF03022642.
https://doi.org/10.1007/BF03022642...
. Non-racemic bupivacaine with
75% S(-)bupivacaine also impaired cardiac muscle relaxation as reported in the present
study.
Many mechanisms were related to myocardial dysfunction associated to LA isomerism. Cardiac sodium channel blockade was caused by both bupivacaine isomers leading to heart conduction impairment, rhythm changes and hemodynamic instability. Moreover, R(+)bupivacaine effect was more potent than S(-) isomer1717 Nau C, Wang SY, Strichartz GR, Wang GK. Block of human heart hH1 sodium channels by the enantiomers of bupivacaine. Anesthesiology. 2000 Oct;93(4):1022-33. PMID: 11020758.. LA was also implicated in sarcolemmal KATP channel harm. Racemic bupivacaine blockade sarcolemmal KATP channel is the same as threefold S(-)bupivacaine and ropivacaine1818 Kawano T, Oshita S, Takahashi A, Tsutsumi Y, Tomiyama Y, Kitahata H, Kuroda Y, Nakaya Y. Molecular mechanisms of the inhibitory effects of bupivacaine, levobupivacaine, and ropivacaine on sarcolemmal adenosine triphosphate-sensitive potassium channels in the cardiovascular system. Anesthesiology. 2004 Aug;101(2):390-8. PMID: 15277922..
Calcium handling impairment was thoroughly studied to explain LA cardiotoxicity.
Isolated myocardium developed tension and intracellular calcium concentration were
equally reduced by racemic bupivacaine and ropivacaine with a potency ratio of 2:11919 Mio Y, Fukuda N, Kusakari Y, Amaki Y, Tanifuji Y, Kurihara S.
Comparative effects of bupivacaine and ropivacaine on intracellular calcium
transients and tension in ferret ventricular muscle. Anesthesiology. 2004
Oct;101(4):888-94. PMID: 15448521.. Racemic bupivacaine and its isomers increased
intracellular calcium concentration in isolated myocytes. Authors believed sarcoplasmic
reticulum ryanodine efflux was favored by racemic bupivacaine and its isomers in the
same manner2020 Zapata-Sudo G, Trachez MM, Sudo RT, Nelson TE. Is comparative
cardiotoxicity of S(-) and R(+) bupivacaine related to enantiomer-selective
inhibition of L-type Ca(2+) channels? Anesth Analg. 2001 Feb;92(2):496-501. PMID:
11159257.. Besides sarcoplasmic reticulum
calcium release, sarcoplasmic reticulum calcium reuptake was blockade and calcium
sensitivity of the contractile system was increased with racemic bupivacaine and its
isomers, displaying a stereoselectivity to S(-)bupivacaine and leading to myocardial
relaxation slowness77 Chedid NG, Sudo RT, Aguiar MI, Trachez MM, Masuda MO, Zapata-Sudo G.
Regulation of intracellular calcium by bupivacaine isomers in cardiac myocytes from
Wistar rats. Anesth Analg. 2006 Mar;102(3):792-8. doi:
10.1213/01.ane.0000195341.65260.87.
https://doi.org/10.1213/01.ane.000019534...
,
1414 Mio Y, Fukuda N, Kusakari Y, Tanifuji Y, Kurihara S. Bupivacaine
attenuates contractility by decreasing sensitivity of myofilaments to Ca2+ in rat
ventricular muscle. Anesthesiology. 2002 Nov;97(5):1168-77. PMID:
12411803.. It was also demonstrated high ropivacaine
concentrations caused L-type calcium channel blockade, leading to negative inotropic
effects in canine ventricular muscle1515 Szentandrassy N, Szabo A, Almassy J, Jona I, Horvath B, Szabo G, Banyasz
T, Marton I, Nanasi PP, Magyar J. Effects of articaine and ropivacaine on calcium
handling and contractility in canine ventricular myocardium. Eur J Anaesthesiol. 2010
Feb;27(2):153-61. doi: 10.1097/EJA.0b013e328331a37b.
https://doi.org/10.1097/EJA.0b013e328331...
.
Previous studies described heart mitochondrial injuries caused by LA. Racemic
bupivacaine induced more respiratory chain impairment than ropivacaine, lidocaine and
etidocaine in cardiac mitochondria2121 Weinberg GL, Palmer JW, VadeBoncouer TR, Zuechner MB, Edelman G, Hoppel
CL. Bupivacaine inhibits acylcarnitine exchange in cardiac mitochondria.
Anesthesiology. 2000 Feb;92(2):523-8. PMID: 10691241.. Myocardial
oxygen consumption was reduced in isolated rat heart intoxicated with
S(-)bupivacaine2222 Stehr SN, Ziegeler JC, Pexa A, Oertel R, Deussen A, Koch T, Hubler M.
The effects of lipid infusion on myocardial function and bioenergetics in
l-bupivacaine toxicity in the isolated rat heart. Anesth Analg. 2007
Jan;104(1):186-92. doi: 10.1213/01.ane.0000248220.01320.58.
https://doi.org/10.1213/01.ane.000024822...
. Mitochondrial injuries,
myocardial oxygen consumption decrease and negative inotropic effects were reported
after bupivacaine and ropivacaine isolated heart intoxication55 Hiller N, Mirtschink P, Merkel C, Knels L, Oertel R, Christ T, Deussen
A, Koch T, Stehr SN. Myocardial accumulation of bupivacaine and ropivacaine is
associated with reversible effects on mitochondria and reduced myocardial function.
Anesth Analg. 2013 Jan;116(1):83-92. doi:
10.1213/ANE.0b013e31826c8095.
https://doi.org/10.1213/ANE.0b013e31826c...
.
Potency is another LA chemical property associated with cardiotoxicity22 Groban L, Dolinski SY. Differences in cardiac toxicity among
ropivacaine, levobupivacaine, bupivacaine and lidocaine. Tech Reg Anesth Pain Manag.
2001;5(2):48-55. doi: 10.1053/trap.2001.2379.
https://doi.org/10.1053/trap.2001.2379...
. It could be a bias to this research because
ropivacaine is less potent than racemic and non-racemic ropivacaine and all LA were
studied in equimolar concentrations. One very important study evaluated the myocardial
contractility impairment with LA and demonstrated ropivacaine did not depress the
developed tension compared to equimolar concentrations of racemic bupivacaine and
levobupivacaine88 David JS, Ferreti C, Amour J, Vivien B, Eve O, Petit P, Riou B,
Gueugniaud PY. Effects of bupivacaine, levobupivacaine and ropivacaine on myocardial
relaxation. Can J Anaesth. 2007 Mar;54(3):208-17. doi:
10.1007/BF03022642.
https://doi.org/10.1007/BF03022642...
. However, myocardial function
evaluated in the isolated rat heart was equally depressed with ropivacaine and racemic
bupivacaine. Ropivacaine concentration was 1.75 times higher than racemic
bupivacaine22 Groban L, Dolinski SY. Differences in cardiac toxicity among
ropivacaine, levobupivacaine, bupivacaine and lidocaine. Tech Reg Anesth Pain Manag.
2001;5(2):48-55. doi: 10.1053/trap.2001.2379.
https://doi.org/10.1053/trap.2001.2379...
. Dose-response relationships
could also be appropriate to better discuss the LA cardiotoxic effects instead of
evaluating two different concentrations. It was also considered a limitation to the
present study.
Conclusions
High concentrations non-racemic bupivacaine, with 75% S(-)bupivacaine and 25% R(+)bupivacaine, depressed the myocardial relaxation similarly to racemic bupivacaine at low and high concentrations. High concentrations of racemic bupivacaine impaired the myocardial contractile function more than non-racemic bupivacaine and ropivacaine. Equimolar ropivacaine concentrations did not lead to significantly myocardial function impairment.
Acknowledgement
To Lidia Raquel de Carvalho, PhD, for her precious assistance with the statistical analysis of this research.
References
-
1Albright GA. Cardiac arrest following regional anesthesia with etidocaine or bupivacaine. Anesthesiology. 1979 Oct;51(4):285-7. PMID: 484889.
-
2Groban L, Dolinski SY. Differences in cardiac toxicity among ropivacaine, levobupivacaine, bupivacaine and lidocaine. Tech Reg Anesth Pain Manag. 2001;5(2):48-55. doi: 10.1053/trap.2001.2379.
» https://doi.org/10.1053/trap.2001.2379 -
3David JS, Amour J, Duracher C, Ferretti C, Precloux P, Petit P, Riou B, Gueugniaud PY. Comparison of the effects of mepivacaine and lidocaine on rat myocardium. Eur J Anaesthesiol. 2007 Feb;24(2):190-7. doi: 10.1017/S0265021506001359.
» https://doi.org/10.1017/S0265021506001359 -
4Butterworth JFt. Models and mechanisms of local anesthetic cardiac toxicity: a review. Reg Anesth Pain Med. 2010 Mar-Apr;35(2):167-76. doi: 10.1097/AAP0b013e3181d231b9.
» https://doi.org/10.1097/AAP0b013e3181d231b9 -
5Hiller N, Mirtschink P, Merkel C, Knels L, Oertel R, Christ T, Deussen A, Koch T, Stehr SN. Myocardial accumulation of bupivacaine and ropivacaine is associated with reversible effects on mitochondria and reduced myocardial function. Anesth Analg. 2013 Jan;116(1):83-92. doi: 10.1213/ANE.0b013e31826c8095.
» https://doi.org/10.1213/ANE.0b013e31826c8095 -
6Tsuchiya H, Mizogami M. R(+)-, Rac-, and S(-)-bupivacaine stereostructure-specifically interact with membrane lipids at cardiotoxically relevant concentrations. Anesth Analg. 2012 Feb;114(2):310-2. doi: 10.1213/ANE.0b013e31823ed410.
» https://doi.org/10.1213/ANE.0b013e31823ed410 -
7Chedid NG, Sudo RT, Aguiar MI, Trachez MM, Masuda MO, Zapata-Sudo G. Regulation of intracellular calcium by bupivacaine isomers in cardiac myocytes from Wistar rats. Anesth Analg. 2006 Mar;102(3):792-8. doi: 10.1213/01.ane.0000195341.65260.87.
» https://doi.org/10.1213/01.ane.0000195341.65260.87 -
8David JS, Ferreti C, Amour J, Vivien B, Eve O, Petit P, Riou B, Gueugniaud PY. Effects of bupivacaine, levobupivacaine and ropivacaine on myocardial relaxation. Can J Anaesth. 2007 Mar;54(3):208-17. doi: 10.1007/BF03022642.
» https://doi.org/10.1007/BF03022642 -
9Vladimirov M, Nau C, Mok WM, Strichartz G. Potency of bupivacaine stereoisomers tested in vitro and in vivo: biochemical, electrophysiological, and neurobehavioral studies. Anesthesiology. 2000 Sep;93(3):744-55. PMID: 10969308.
-
10Valenzuela C, Snyders DJ, Bennett PB, Tamargo J, Hondeghem LM. Stereoselective block of cardiac sodium channels by bupivacaine in guinea pig ventricular myocytes. Circulation. 1995 Nov;92(10):3014-24. doi: 10.1161/01.CIR.92.10.3014. PMID: 7586272.
-
11Morrison SG, Dominguez JJ, Frascarolo P, Reiz S. A comparison of the electrocardiographic cardiotoxic effects of racemic bupivacaine, levobupivacaine, and ropivacaine in anesthetized swine. Anesth Analg. 2000 Jun;90(6):1308-14. PMID: 10825311.
-
12Graf BM, Abraham I, Eberbach N, Kunst G, Stowe DF, Martin E. Differences in cardiotoxicity of bupivacaine and ropivacaine are the result of physicochemical and stereoselective properties. Anesthesiology. 2002 Jun;96(6):1427-34. PMID: 12170056.
-
13Trachez MM, Zapata-Sudo G, Moreira OR, Chedid NG, Russo VF, Russo EM, Sudo RT. Motor nerve blockade potency and toxicity of non-racemic bupivacaine in rats. Acta Anaesthesiol Scand. 2005 Jan;49(1):66-71. doi: 10.1111/j.1399-6576.2004.00536.x.
» https://doi.org/10.1111/j.1399-6576.2004.00536.x -
14Mio Y, Fukuda N, Kusakari Y, Tanifuji Y, Kurihara S. Bupivacaine attenuates contractility by decreasing sensitivity of myofilaments to Ca2+ in rat ventricular muscle. Anesthesiology. 2002 Nov;97(5):1168-77. PMID: 12411803.
-
15Szentandrassy N, Szabo A, Almassy J, Jona I, Horvath B, Szabo G, Banyasz T, Marton I, Nanasi PP, Magyar J. Effects of articaine and ropivacaine on calcium handling and contractility in canine ventricular myocardium. Eur J Anaesthesiol. 2010 Feb;27(2):153-61. doi: 10.1097/EJA.0b013e328331a37b.
» https://doi.org/10.1097/EJA.0b013e328331a37b -
16Mulroy MF. Systemic toxicity and cardiotoxicity from local anesthetics: incidence and preventive measures. Reg Anesth Pain Med. 2002 Nov-Dec;27(6):556-61. PMID: 12430104.
-
17Nau C, Wang SY, Strichartz GR, Wang GK. Block of human heart hH1 sodium channels by the enantiomers of bupivacaine. Anesthesiology. 2000 Oct;93(4):1022-33. PMID: 11020758.
-
18Kawano T, Oshita S, Takahashi A, Tsutsumi Y, Tomiyama Y, Kitahata H, Kuroda Y, Nakaya Y. Molecular mechanisms of the inhibitory effects of bupivacaine, levobupivacaine, and ropivacaine on sarcolemmal adenosine triphosphate-sensitive potassium channels in the cardiovascular system. Anesthesiology. 2004 Aug;101(2):390-8. PMID: 15277922.
-
19Mio Y, Fukuda N, Kusakari Y, Amaki Y, Tanifuji Y, Kurihara S. Comparative effects of bupivacaine and ropivacaine on intracellular calcium transients and tension in ferret ventricular muscle. Anesthesiology. 2004 Oct;101(4):888-94. PMID: 15448521.
-
20Zapata-Sudo G, Trachez MM, Sudo RT, Nelson TE. Is comparative cardiotoxicity of S(-) and R(+) bupivacaine related to enantiomer-selective inhibition of L-type Ca(2+) channels? Anesth Analg. 2001 Feb;92(2):496-501. PMID: 11159257.
-
21Weinberg GL, Palmer JW, VadeBoncouer TR, Zuechner MB, Edelman G, Hoppel CL. Bupivacaine inhibits acylcarnitine exchange in cardiac mitochondria. Anesthesiology. 2000 Feb;92(2):523-8. PMID: 10691241.
-
22Stehr SN, Ziegeler JC, Pexa A, Oertel R, Deussen A, Koch T, Hubler M. The effects of lipid infusion on myocardial function and bioenergetics in l-bupivacaine toxicity in the isolated rat heart. Anesth Analg. 2007 Jan;104(1):186-92. doi: 10.1213/01.ane.0000248220.01320.58.
» https://doi.org/10.1213/01.ane.0000248220.01320.58
-
Financial source: FAPESP (Protocol d2010/50638-3)
-
1
Research performed at Papillary Muscle Experimental Laboratory, Department of Internal Medicine, Botucatu School of Medicine, Universidade Estadual de São Paulo (UNESP), Brazil. Part of PhD degree thesis, Postgraduate Program in Anesthesiology, UNESP. Tutor: Eliana Marisa Ganen.
Publication Dates
-
Publication in this collection
July 2015
History
-
Received
20 Mar 2015 -
Reviewed
18 May 2015 -
Accepted
22 June 2015