Abstract
PURPOSE: To assess the effect of a program of singing training on the voice of total laryngectomees wearing tracheoesophageal voice prosthesis, considering the quality of alaryngeal phonation, vocal extension and the musical elements of tunning and legato. METHODS: Five laryngectomees wearing tracheoesophageal voice prosthesis completed the singing training program over a period of three months, with exploration of the strengthening of the respiratory muscles and vocalization and with evaluation of perceptive-auditory and singing voice being performed before and after 12 sessions of singing therapy. RESULTS: After the program of singing voice training, the quality of tracheoesophageal voice showed improvement or the persistence of the general degree of dysphonia for the emitted vowels and for the parameters of roughness and breathiness. For the vowel "a", the pitch was displaced to grave in two participants and to acute in one, and remained adequate in the others. A similar situation was observed also for the vowel "i". After the singing program, all participants presented tunning and most of them showed a greater presence of legato. The vocal extension improved in all participants. CONCLUSION: Singing training seems to have a favorable effect on the quality of tracheoesophageal phonation and on singing voice.
Laryngectomy; Speech, Alaryngeal; Voice Training
ORIGINAL ARTICLE
CLINICAL INVESTIGATION
Effect of singing training on total laryngectomees wearing a tracheoesophageal voice prosthesis1 Correspondence: Lílian Neto Aguiar-Ricz Departamento de Oftalmologia, Otorrinolaringologia e Cirurgia de Cabeça e Pescoço Faculdade de Medicina de Ribeirão Preto-USP Avenida Bandeirantes, 3900 14049-900 Ribeirão Preto - SP Brasil Tel.: (55 16)3602-2862 Fax: (55 16)3602-2860 mcecilia@hcrp.fmrp.usp.br
Fernanda OnofreI; Hilton Marcos Alves RiczII; Telma Kioko Takeshita-MonarettiIII; Maria Yuka de Almeida PradoIV; Lílian Neto Aguiar-RiczV
IFellow Master degree, Department of Ophtalmology, Otorhinolaryngology and Head and Neck Surgery, Faculty of Medicine of Ribeirao Preto, USP, Sao Paulo, Brazil. Acquisition, interpretation and analysis of data, manuscript writing, critical revision
IIAssistant Professor, Department of Ophtalmology, Otorhinolaryngology and Head and Neck Surgery, Faculty of Medicine of Ribeirao Preto, USP, Sao Paulo, Brazil. Interpretation and analysis of data, manuscript writing, critical revision
IIIFellow PhD degree, Department of Ophtalmology, Otorhinolaryngology and Head and Neck Surgery, Faculty of Medicine of Ribeirao Preto, USP, Sao Paulo, Brazil. Interpretation and analysis of data, manuscript writing, critical revision
IVPhD Assistant Professor, Department of Music of the Faculty of Philosophy, Sciences and Letters of Ribeirão Preto of University of São Paulo. Interpretation of the data, writing, analysis and critical revision of the manuscript
VPhD, Assistant Professor, Department of Ophtalmology, Otorhinolaryngology and Head and Neck Surgery, Faculty of Medicine of Ribeirao Preto, USP, Sao Paulo, Brazil. Conception and design of the study, interpretation and analysis of data, manuscript writing, critical revision
Correspondence Correspondence: Lílian Neto Aguiar-Ricz Departamento de Oftalmologia, Otorrinolaringologia e Cirurgia de Cabeça e Pescoço Faculdade de Medicina de Ribeirão Preto-USP Avenida Bandeirantes, 3900 14049-900 Ribeirão Preto - SP Brasil Tel.: (55 16)3602-2862 Fax: (55 16)3602-2860 mcecilia@hcrp.fmrp.usp.br
ABSTRACT
PURPOSE: To assess the effect of a program of singing training on the voice of total laryngectomees wearing tracheoesophageal voice prosthesis, considering the quality of alaryngeal phonation, vocal extension and the musical elements of tunning and legato.
METHODS: Five laryngectomees wearing tracheoesophageal voice prosthesis completed the singing training program over a period of three months, with exploration of the strengthening of the respiratory muscles and vocalization and with evaluation of perceptive-auditory and singing voice being performed before and after 12 sessions of singing therapy.
RESULTS: After the program of singing voice training, the quality of tracheoesophageal voice showed improvement or the persistence of the general degree of dysphonia for the emitted vowels and for the parameters of roughness and breathiness. For the vowel "a", the pitch was displaced to grave in two participants and to acute in one, and remained adequate in the others. A similar situation was observed also for the vowel "i". After the singing program, all participants presented tunning and most of them showed a greater presence of legato. The vocal extension improved in all participants.
CONCLUSION: Singing training seems to have a favorable effect on the quality of tracheoesophageal phonation and on singing voice.
Key words: Laryngectomy. Speech, Alaryngeal. Voice Training.
Introduction
After surgical removal of the larynx for the treatment of laryngeal carcinoma, the pharynx, the pharyngoesophageal transition and the esophagus not only perform their digestive function but are also stimulated to take on voice and speech production, which is an extremely refined function.
The perceptive voice pitch and loudness represent aspects of the dynamics of the spoken or singing voice that can be explored and used as expressive resources for the rehabilitation of individuals submitted to ablative larynx surgery due to cancer. The spoken voice differs from the singing voice in terms of the utilization of vocal resources resulting from specific adjustments for different emissions that may help promote the quality of life and the refinement of speech of total laryngectomees.
The multidisciplinary conduct in cases of surgical oncology should favor not only the excision of the tumor and oncologic control, but also the rehabilitation of the individual for life in society1. Thus, multidisciplinary work involving the head and neck surgeon, a speech therapist and a singing teacher is relevant for total laryngectomees speaking with a tracheoesophageal prosthesis in order to favor their oral communication and to elicit or refine the musical profile of those who have it, contributing to their quality of life. The process of alaryngeal voice rehabilitation needs to advance in terms of the quality of communication, permitting the acquisition and utilization of a satisfactory alaryngeal emission capable of reproducing the intentional and emotional aspects of these individuals during conversation with their interlocutors.
The melody of the sentence and singing show improvement when comparing the pre and post-training conditions of total laryngectomees speaking with tracheoesophagel prosthesis. Thus, the need to explore this training as much as possible is emphasized, since a monotonous voice is a common characteristic of this population, which impairs speech intelligibility during a conversation2. Despite the importance of the action of singing for the improvement of communication, there is a need for studies involving singing in the process of speech rehabilitation for patients submitted to total larynx removal for oncologic treatment.
The objective of the present study was to evaluate the effect of a program of singing training on the tracheoesophageal voice of total laryngectomees rehabilitated with a tracheoesophageal prosthesis, considering the quality of alaryngeal voice, the vocal extension and the musical elements of tunning and legato.
Methods
The study was approved by the Research Ethics Committee of the Hospital, protocol nº 57077/2008.
Sixty-seven speech therapy protocols of total laryngectomees submitted to surgery from 1999 to 2008 and rehabilitated with the use of prosthesis for tracheoesophageal voice were reviewed and 14 subjects were invited to participate in the study. Of these, seven started the program of singing training proposed, but two were excluded due to lack of adhesion. Thus, five total laryngectomees aged on average 49.8 years, two women and three men, completed the program of singing training.
All participants were submitted to classical total laryngectomy with closure of the mucosal, submucosal and muscular layers for reconstruction of the pharynx, and four of them had also been submitted to cervical dissection and complementary radiotherapy. Two participants were submitted to primary insertion and three to secondary insertion of the Provox® tracheoesophageal prosthesis (Atos Medical AB, Hörby, Sweden), and all were submitted to speech therapy for the rehabilitation of alaryngeal communication.
Procedures
Evaluation of tracheoesophageal voice quality
After being released and referred by the head and neck surgeon, the participants were first submitted to evaluation of the voice with a tracheoesophageal prosthesis. The voice was recorded individually in an acoustically treated room with monitoring of ambient noise below 50 dB, with a mean value of 43.7 dB measured with a digital decibel meter. Mean habitual temperature in the recording environment was 23.8°C and mean humidity was 53.25%, monitored with a digital thermo-hygrometer.
The voice material of the total laryngectomees was collected and recorded using a Sony® digital video camera adapted to a tripod. The participants remained seated at a distance of one meter from the camera and were instructed to emit the prolonged vowels "a", "i", "u" after inspiration in the maximum phonation time with habitual vocal intensity, velocity and pitch. This procedure was carried out before the program of singing training, characterized as the fixed variable, and at the end of the 12 sessions of proposed training.
The validated categorical scale GIRBAS3 was used to characterize the voice quality of total laryngectomees wearing tracheoesophagel prosthesis. The pitch parameter was rated as adequate (A), grave (Gr) or acute (Ac) for gender and age, with Gr and Ac being accompanied by the degree of severity of deviation, i.e., mild (1), moderate (2) or severe (3).
Perceptive-auditory evaluation was based on the independent rating of three speech therapists with voice specialization and with a clinical experience of at least three years in the rehabilitation of total laryngectomees. The analysis procedure consisted of the following steps: description of the objectives of the study and presentation of the response card; training of the experts with a sample of ten voices of speakers wearing a tracheoesophageal prosthesis; characterization of vocal quality and pitch during a single meeting, and finally random reproduction of a voice sample for the reliability of the analyses, corresponding to 20% of the total number. The stimuli were offered at medium reproduction intensity, comfortable for the raters.
Evaluation of singing voice
After recording the voice for perceptive-auditory analysis, each total laryngectomized was submitted to recording of singing voice, characterized as the fixed variable, before the singing training program and at the end of the 12 sessions under the same recording conditions described earlier, plus the utilization of the Yamaha® PSR E403 keyboard.
To determine the vocal extension within one octave, i.e., a scale of eight notes (do, re, mi, fa, sol, la, si, do), each participant was instructed to emit the vowels "a", "i", "u" after inspiration, in the same tone presented on the keyboard, going up and down the scale with maximum utilization from semitone to semitone, regardless of vocal quality. The analysis was carried out by the singing teacher responsible for training by recording the notes achieved by the participants during each meeting. The type of breathing was evaluated visually during the emission of the vowels "a", "i", "u" during the training session.
Next, the participant was asked to sing "Happy birthday to you" for analysis of the musical elements of tunning, characterized by the "notion" of intervals between notes, and legato, linking a vowel to the other in the melody. These parameters were characterized before and after the 12 training sessions as "Absent", "Present" or "Present Plus" by three independent singing teachers with didactic experience in the area of at least three years. The same steps described earlier for the perceptive-auditory analysis of the voice were followed for the analysis and evaluation of inter-rater reliability regarding the categorical variables of each parameter.
Singing voice training
Each total laryngectomized was submitted to singing training consisting of a weekly trial of 30 minutes for a period of three months (12 sessions) based on the following hierarchically arranged techniques:
1. Exercises for the strengthening of respiratory muscles for singing:
- inhaling slowly - exhaling fast;
- inhaling fast - exhaling slowly;
- inhaling fast- pausing for a few seconds - exhaling slowly;
- inhaling slowly - pause - exhaling fast;
- inhaling slowly - pause - exhaling by adding a count orally presented by another person and gradually increased depending on the possibilities of each participant. Inhaling was performed through the stoma and exhaling through the mouth. These exercises were performed without sound emission;
- inhaling and exhaling fast. This exercise involves three short breaths and one long breath.
2. Vocalization: after breathing training, each participant was instructed to perform the vocalizing exercises executed within a musical scale of eight notes (do, re, mi, fa, sol, la, si, do), accompanied by the keyboard.
Statistical analysis
For the analysis of the quality of tracheoesophageal and singing voice in total laryngectomized, inter-rater reliability was determined regarding the categorical variables of each parameter analyzed by calculating the percentage of concordant (50% or more) and discordant (less than 50%) ratings. To this end, the most experienced rater was considered to be the reference judge for each crossing of the analyses with the remaining raters. The predominance of a parameter was characterized according to the greatest percentage of agreement between raters for the situation before and after the singing program. A file containing all the edited samples was constructed, with the addition of 20% random repetition (one participant) for inter-rater analysis with a minimum of 68% reliability.
Results
The perceptive-auditory evaluation of the quality of tracheoesophageal voice after the program of singing voice training revealed improvement or permanence of the general degree of dysphonia (G) for the vowels emitted as well as for the parameters of roughness (R) and breathiness (B). Asthenia (A) continued to be absent after the proposed training, and strain (S) was found to be worse only for the emission of the vowel "i". After singing training, the instability parameter (I) was found to be moderate for all participants during the emission of the vowel "i" (Table 1).
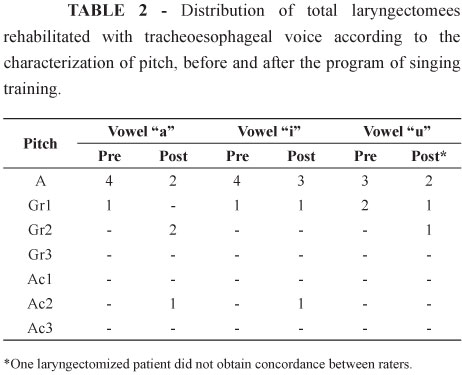
Before singing training, the pitch parameter was characterized as adequate for most of the participants according to the speech therapist raters. After training, pitch shifted to grave (Gr2) for the vowel "a" in two participants and to acute (Ac2) in one, continuing to be adequate in the remaining ones. A similar situation was detected also for the vowel "i", with one case of acute pitch (Ac2) and one case of grave (Gr1) picth, and the remaining ones being adequante after training. An acute pitch was not detected only for the vowel "u". Table 2 presents these findings.
Regarding the evaluation of the musical elements, before singing training, tunning was considered to be absent in three individuals and as present in two. After the singing program, all participants presented tunning. Before training, legato was present in three participants and absent in two. After the training program, three participants showed a greater presence of legato and only one individual continued not to present it according to the evaluation of singing voice (Table 3).
The vocal extension of pitch in semitones for the group of total laryngectomees is presented in Table 4. The mean extension obtained for the vowels "a" and "u" was 14.7 semitones and the mean extension obtained for the vowel "i" was 15.7 semitones.
Discussion
Today, the process of rehabilitation of communication with a tracheoesophageal prosthesis in total laryngectomees requires an accurate speech therapy program not only for the acquisition of alaryngeal sound, but also aiming at its quality and refinement so that the patient submitted to ablative surgery of the larynx will be able to communicate and to make himself understood. Musical activity plays an expressive role in voice refinement. As is the case for individuals with an intact larynx, the interface between Speech Therapy and Singing for the population of total laryngectomees is essential for the joint exploration of the behavior and anatomophysiological adjustments of the new sound source associated with singing techniques.
Despite the small number of participants who completed the program of singing voice training after speech therapy for vocal rehabilitation with a tracheoesophageal prosthesis, the perceptive-auditory evaluation demonstrated maintenance or improvement of the parameters of the general degree of dysphonia, roughness and breathiness after the 12 sessions of singing therapy. This fact suggests that the program offered was favorable for these vocal parameters, influencing the new anatomical conformation of the sound source, considering the individual clinical characteristics that might have influenced the distinct responses of improvement, such as time of surgery, radiotherapy and cervical dissection.
The vocal parameter asthenia was not identified in the participants at the two times of vocal analysis, suggesting that none of the participants presented hypofunction of the new sound source associated with hypertonicity or hypotonicity of the cricopharyngeal musculature after surgery for the removal of the larynx, compromising the quality of tracheoesophageal communication.
A worsening of vocal strain for a minority of participants was identified only for the vowel "i" after the singing program, justified by the greater difficulty of the pharyngeal musculature to adapt to the conditions necessary for its production, with excessive contraction and with an effort in the reproduction of the sound compared to a higher pitch. A similar situation was also observed regarding vocal instability in the production of the vowel "i", which appeared to require more in terms of the behavior of the new sound source to reach phonatory balance. In order to understand this fact, we should emphasize again the individual clinical differences associated with the time of response of each individual to the training offered. Thus it would be necessary to evaluate the therapeutic limits versus the duration of the singing program; in other words, the 12 sessions possibly were not sufficient for some of the participants, or they were sufficient but the anatomophysiological conditions of the subjects represented a limitation. Perhaps an increased number of singing training sessions may contribute to a better elucidation of these findings.
In the pre-training condition, most of the participants presented adequate pitch, with a minority being characterized as Gr1, as commonly observed in the literature, which demonstrates that the pitch of this population is more grave2,4. Because this is a new sound source and because it is necessary to understand its behavior during the emission of the different sounds, the vowels "a", "i" and "u" were contemplated for the analysis of the vocal parameters explored in the present study, based on the basic physiology of laryngeal phonation.
After singing voice training, the emission of the vowel "u" did not present acute pitch in any of the participants, probably due to the more grave nature of its production and possibly due to the anatomical conformation favorable for this behavior. However, for the remaining vowels there was a characterization of pitch Ac2, possibly related to the greater effort of the pharyngoesophageal muscles for its production, resulting in vocal strain and in more acute pitch perception.
According to Damsté and Learman5, the shape of the pharyngoesophageal segment varies with the type of phonation, tending to be more prominent during acute and strong phonation, with greater distention of the upper portion of the esophagus. Deschler et al.6 reported that the cause of pitch control in tracheoesophageal speakers has not been clearly defined, but that knowledge of the sound pressure level is a significant factor for the prediction of pitch associated with other aspects.
Regarding the quality of vocal emission, we emphasize the influence of the control of air flow for sound production when associated with the behavior of the remaining structures that compose the new sound source, which must respond to the different vocal requirements in an adapted manner. In view of this important influence and considering the respiratory work to be one of the primordial objectives for the training of singing voice, the strengthening of the respiratory muscles was explored in the training offered to the participants in the present study, in association with the actual vocalization. Some studies have related the breathing mode to the production of singing voice, permitting improvement of its quality7,8.
Studies on singers9-10 support the notion that breathing permits starting and maintaining the vibration of the vocal folds and controlling the prosodic resources and vocal intensity. In addition, by means of the balance of the laryngeal myoelastic forces, breathing provides an adequate degree of muscle contraction. Perhaps the analysis of the type of breathing and air pressure threshold of total laryngectomees before and after singing may contribute to the quality of the vocal findings.
Although it was not contemplated, the evaluation of voice intensity of total laryngectomees could improve together with the breathing work offered, with a direct effect on the quality of singing and spoken emission, since it is related to the modulation, intonation, rhythm and intention of the discourse, acting together with vocal extension and tessitura.
Singing training had a favorable effect on pitch modulation and vocal extension, showing the importance of this work with pitch for the adapted behavior of the new sound source, the digestive tract, for the production of sound with an appropriate pitch adjustment during conversation, with the voice being no longer monotonous. In addition to the importance of the remaining structures, the control of air flow by the esophagus and the pharynx obtained with respiratory training favored the adjustment of the intensity of the discourse of total laryngectomees. There are no literature data regarding the vocal extension of total laryngectomees for comparison with our data, with studies in this area being necessary since this is an important parameter for the evaluation of the physiological limits of the vocal mechanism11,12.
Despite the improvement achieved with singing voice training, vocal extension was lower compared to literature data, which report values of 4.5 to 5 octaves for individuals with intact vocal folds13-15.
Both the musical elements legato and tunning improved, with most participants showing "presence plus" characterization after singing voice training. Legato was absent in only one participant after training, perhaps owing to his anatomofunctional limitations after complementary radiotherapy following surgery. We infer that that remaining structure of the pharynx may be able to lengthen and contract for the vocal reproduction of the note and the connection of one vowel to the other (legato).
It should be pointed out that experience in the area, training and reliability were essential requirements for the raters involved, guaranteeing the reliability of the data despite the reduced sample size. The adhesion of the participants was the limiting factor detected in the present study, possibly due to the level of motivation, time difficulties and the weekly frequency, problems in the understanding and execution of the instructions, and failure to identify the benefits of singing for one's life.
Based on the present results regarding singing work for tracheoesophageal voice, it is necessary to continue this research line in order to obtain expressive results with respect to the performance of the spoken and singing voice of laryngectomized patients. In addition, the literature does not contain any published reports of standardized and validated programs of speech therapy rehabilitation associated with singing voice training that would permit clinical and methodological reproduction. The present proposal led to a reduction of the degree of roughness and to improved pitch in the subjects studied, in addition to permitting the inclusion of a total laryngectomee in the choir of the local church formed by individuals with an intact larynx.
Conclusions
After the program of singing voice training for total laryngectomees wearing a tracheoesophageal prosthesis, the general degree of dysphonia, roughnness and breathiness improved or remained stable for the prolonged emission of vowels. After the proposed training, there was no occurrence of acute pitch only for the vowel "u". Regarding the musical elements, all participants started to present tunning and most of them presented greater legato, in addition to an increase of vocal extension, demonstrating the effect of singing on tracheoesophageal voice.
Received: September 25, 2012
Review: November 26, 2012
Accepted: December 20, 2012
Conflict of interest: none
Financial source: none
1 Research performed at Division of Otorhinolaryngology, Faculty of Medicine of Ribeirao Preto, University of Sao Paulo (USP), Brazil. Part of Master degree Thesis, Postgraduate Program in Ophthalmology, Otorhinolaryngology and Head and Neck Surgery. Tutor: Profa. Dra. Lilian Neto Aguiar Ricz.
- 1. Blom ED. Current status of voice restoration following total laryngectomy. Oncology (Huntingt). 2000;14:915-22.
- 2. Oliveira IB, Costa CC, Chagas JFS, Rochetti ECG, Oliveira LO. Comunicação oral de laringectomizados com prótese traqueoesofágica: análise comparativa pré e pós-treino. Pró Fono. 2005;17(2):165-74.
- 3. Dejonckere PH, Remacle M, Fresnel-Elbaz E, Woisard V, Crevier-Buchman L, Millet B. Differentiated perceptual evaluation of pathological voice quality: reliability and correlations with acoustic measurements. Rev Laryngol Otol Rhinol.1996;117(3):219-24.
- 4. Hilgers FJ, van As-Brooks CJ, Polak RM, Bing TI. Surgical improvement of hypotonicity in tracheoesophageal speech. Laryngoscope. 2006;116(2):345-8.
- 5. Damsté PH, Lerman JW. Configuration of the neoglottis: an x-ray study. Folia Phoniatr Logop.1969;21(5):347-58.
- 6. Deschler DG, Doherty ET, Reed CG, Singer MI. Effects of sound pressure levels on fundamental frequency in tracheoesophageal speakers. Otolaryngol Head Neck Surg. 1999;121(1):23-6.
- 7. Amato RCF. Investigação sobre o fluxo expiratório na emissão cantada e falada de vogais do português em cantores líricos brasileiros. Rev Mus Hodie. 2007;7(1):67-82.
- 8. Andrade SR, Fontoura DR, Cielo CA. Inter-relações entre fonoaudiologia e canto. Rev Mus Hodie. 2007;7(1):83-98.
- 9. Leanderson R, Sundberg J. Breathing for singing. J Voice. 1988;2(1):2-12.
- 10. Mendes AP, Brown WS, Sapienza C. Effects of vocal training on respiratory kinematics during singing tasks. Folia Phoniatr Logop. 2006;58:363-77.
- 11. Speyer R, Wieneke H, Wijck-Warnaar I, van Dejonckere P. Effects of voice therapy on the voice range profile of dysphonic patients. J Voice. 2003;17(4):544-56.
- 12. Costa PJBM, Ferreira KL, Camargo ZA, Pinho SMR. Extensão vocal de coros evangélicos amadores. Rev CEFAC. 2006;8(1):96-106.
- 13. Vargas AC, Costa AG, Hanayama EM. Perfil da extensão vocal em indivíduos falantes normais do português brasileiro. Rev CEFAC. 2005;7(1):108-16.
- 14. Cruz TLB, Gama ACC, Hanayama EM. Análise da extensão vocal e tessitura vocal do contratenor. Rev CEFAC. 2004;6(4):423-28.
- 15. Rocha TF, Amaral FP, Hanayama EM. Extensão vocal de idosos coralistas e não coralistas. Rev CEFAC. 2007;9(2):248-54
Publication Dates
-
Publication in this collection
28 Jan 2013 -
Date of issue
Feb 2013
History
-
Received
25 Sept 2012 -
Accepted
20 Dec 2012 -
Reviewed
26 Nov 2012