Abstract
Fifty one strains of the Bacteroides fragilis group were isolated from 45 fecal samples. Classical phenotypic identification showed that 16 isolates were B. thetaiotaomicron, 12 B. uniformis, 9 B. eggerthii,7 B. vulgatus,3 B. caccae,2 Parabacteroides distasonis with 1 identified B. ovatus and 1 B. fragilis. The 51 strains were tested for susceptibility against 16 antimicrobial agents and the MICs for metronidazole were determined. The tests showed that imipenem, meropenem and chloram-phenicol were the most effective antibiotics (98%, 98% and 92.16% of susceptibility, respectively) followed by ticarcillin/clavulanic acid, piperacillin/tazobactam, rifampin (88.24% susceptibility), moxifloxacin 86.27% and tigecycline 84.31%. Ofloxacin and cefotaxime were the least effective antibiotics with 27.45% and 0% of activity respectively. Only six of the 51 isolated strains were resistant to metronidazole with MICs = 64 mg/L (1 strain) and > 256 mg/L (5 strains).
Bacteroides fragilis group; anaerobic bacteria; antibiotics susceptibility
MEDICAL MICROBIOLOGY
RESEARCH PAPER
Prevalence and antibiotic susceptibility of Bacteroides fragilis group isolated from stool samples in North Lebanon
Mariam YehyaI; Monzer HamzeI,II; Hassan MallatI,II; Fouad DabbousiI,II
IHealth and Environmental Microbiology Laboratory, AZM Centre for Research in Biotechnology and its Application, Doctoral School, Lebanese University, Tripoli, Lebanon
IIFaculty of Public Health, Section 3, Lebanese University, Tripoli, Lebanon
Correspondence Correspondence M. Hamze AZM Centre for Research in Biotechnology and its Application The Lebanese University Mitein Street, Tripoli, Lebanon E-mail: mhamze@monzerhamze.com
ABSTRACT
Fifty one strains of the Bacteroides fragilis group were isolated from 45 fecal samples. Classical phenotypic identification showed that 16 isolates were B. thetaiotaomicron, 12 B. uniformis, 9 B. eggerthii,7 B. vulgatus,3 B. caccae,2 Parabacteroides distasonis with 1 identified B. ovatus and 1 B. fragilis. The 51 strains were tested for susceptibility against 16 antimicrobial agents and the MICs for metronidazole were determined. The tests showed that imipenem, meropenem and chloram-phenicol were the most effective antibiotics (98%, 98% and 92.16% of susceptibility, respectively) followed by ticarcillin/clavulanic acid, piperacillin/tazobactam, rifampin (88.24% susceptibility), moxifloxacin 86.27% and tigecycline 84.31%. Ofloxacin and cefotaxime were the least effective antibiotics with 27.45% and 0% of activity respectively. Only six of the 51 isolated strains were resistant to metronidazole with MICs = 64 mg/L (1 strain) and > 256 mg/L (5 strains).
Key words:Bacteroides fragilis group, anaerobic bacteria, antibiotics susceptibility.
Introduction
Bacteroides fragilis group are gram-negative, anaerobic, non spore-forming and bile resistant bacteria. They are part of the endogenous microbiota of humans and other mammals (Aldridge and O'Brien, 2002; Rodriguez et al., 2006). The species most frequently isolated from the flora are B. thetaiotaomicron, B. vulgatus and P. distasonis and to a less extent B. eggerthii and B. fragilis (Holdeman et al., 1976).
Members of this group have the potential to be opportunistic pathogens when they are transferred to a normally sterile site (Smith et al., 2006). Moreover, they are clinically important and constitute more than a third of anaerobes isolated from clinical samples (Goldstein, 1996).
The Bacteroides are frequently isolated from mixed infections involving aerobic and anaerobic bacteria such as intra-abdominal infections (Aldridge, 1995). They are also responsible for gynecological infections (Bergan, 1983), endocarditis and pericarditis (Brook, 2002a), bacteremia (Brook, 2002b), B. fragilis one of the 10 species of the B. fragilis group is the most frequently isolated from blood cultures (Aldridge, 1995).
The choices of antibiotics for treatment are limited because the species of the Bacteroides fragilis group are among the most resistant anaerobic to antimicrobial agents (Syndman et al., 2002).
The most frequently prescribed antibiotics include β-lactams, carbapenems, clindamycin, metronidazole. Fluoroquinolons are also prescribed in combination with either clindamycin or metronidazole (Brook, 2002c).
Resistance to the most active drugs, such as imipenem, piperacillin-tazobactam, ampicillin-sulbactam, and metronidazole, is reported in occasional strains (Pumbwe et al., 2007).
The antimicrobial susceptibility varies between species of this group (Aldridge and O'Brien, 2002) and B.fragilis being more susceptible to numerous antimicrobial agents than other species of the B. fragilis group (Wexler, 2007).
In Lebanon, we lack national data about the prevalence of various species of Bacteroides fragilis group in the intestinal flora and their susceptibility to antibiotics.
The aim of this work was to determine the prevalence of Bacteroides fragilis group species in 45 diarrheal and non-diarrheal stools samples, their antibiotic susceptibility and finally to determine the minimal inhibitory concentration (MIC) to metronidazole by using E-test.
Materials and Methods
Location and period of the study
The study took place in the microbiology laboratory at the AZM center for biotechnology research and its applications Lebanese University in Tripoli, northern Lebanon, between May 30 and July 25, 2011.
Sampling and transporting of samples
The study was made feasible through collaboration with several hospitals laboratories: Nini, Haykal, Islami, Mazloum and Monla.
Upon receipt of the stool, the technician in charge swabbed the stool. To preserve the viability of Bacteroides, the transport system Port-A-Cul (Beckton-Dikinson, USA) was used. This system contains a medium suitable for the transport of anaerobic bacteria.
Promptly after collection, the samples were transported to the center for analysis.
45 stool samples with different characteristics (liquid, viscous and solid) were collected.
Isolation of Bacteroides
Upon receipt, the contents of each swab was spread on the surface of a regenerated Columbia base agar (Biorad, France) supplemented with 5% blood, hemin 0.005 g/L (Sigma, Germany) and vitamin K 0.01 g/L (Sigma, Germany).
This medium is made selective by the use of the following antibacterial agents: Amikacin (0.01 g/L) and vancomycin (0.004 mg/L) and antifungal agent: mycostatin (240 U/L).
Immediately after inoculation, the plates were rapidly incubated in anaerobic atmosphere, using an Oxoid type jar and GENbox bags (Biomérieux, France). The anaerobic environment was confirmed via the introduction of an anaerobiosis indicator Anaer indicator strips (Biomérieux, France).
After closing, the jar was incubated at 35-36 °C for 48 hours.
To control the medium used and the culture conditions, the following reference strains were used: B. fragilis ATCC 25285, B. uniformis ATCC 8492, B. vulgatus ATCC 29327, B. Ovatus ATCC 8483.
Characterization of isolates
The colonies having these following aspects, smooth white to gray non hemolytic and 1 to 3 mm in diameter, were gram stained and the respiratory type was determined by using the standard tube method according to Marchal et al. (1982) which is based on the culture of the suspected colonies in a regenerated meat-liver medium (Biorad, France) placed in a tube of 9 x 180 mm of size, as result the anaerobic bacteria have grown at the bottom of the agar. A subculture was performed for each colony that showed the presence of anaerobic gram negative bacilli.
The full identification was obtained using a biochemical gallery RapIDTMANAII (Remel Company, USA) whose protocol was followed. The inoculum turbidity was equal to 3 McFerland turbidity or equivalent and the incubation was performed in a non-CO2 incubator for 4 to 6 hours at 37 °C.
The same reference strains were used for the quality control.
Susceptibility of isolates to antibiotics
The susceptibility test was realized by the disk diffusion method and according to the protocol proposed by the committee of antibiogram of the French Microbiology Society (CA-SFM, 2011). The bacterial suspension was prepared in regenerated NaCl 5% and had a turbidity equivalent to 1 McFarland (108 UFC/mL). This suspension was inoculated onto Wilkins-Chalgren agar medium (Beckton-Dikinson, USA) supplemented with 5% of horse blood.
The interpretation of results was done after 48 hours of incubation at 37 °C in an anaerobic atmosphere.
We used the discs commercialized by Biorad®-France as followed: Amoxicillin + Clavulanic Acid AMC (20/10 µg), Ticarcillin + Clavulanic Acid TCC (75/10 µg), Piperacillin + Tazobactam TZP (100/10 µg), Cefoxitin FOX (30 µg), Cefotaxime CTX (30 µg), Imipenem IPM (10 µg),Meropenem MEM (10 µg), Kanamycin K (30 µg), Vancomycin VA (30 µg), Colistin CS (10 µg), Chloram-phenicol C (30 µg), Rifampin RA (30 µg), Ofloxacin OFX (5 µg), Moxifloxacin MXF (5 µg), Clindamycin CM (2 µg), Tigecyclin TGC (15 µg).
Finally, we determined the MIC of the isolates to metronidazole using the E-test method. We used the strips commercialized by Biodisk-Solna, Sweden, distributed in Lebanon by Biomérieux-France. The test was performed according to the protocol suggested by the CA-SFM (2011).
Results
In total, we analyzed 45 stools and after isolation, 51 Bacteroides strains identified by the RapIDTMANAII device, were investigated (Table 1).
Note: there were 6 samples from which we isolated two different species of the Bacteroides fragilis group.
Results of the antimicrobial susceptibility of the Bacteroides fragilis group strains, are summarized in Table 2.
The results of MICs of metronidazole determined by the E-test method were: 45 strains with an MIC < 4 µg/mL, 1 strain with an MIC = 64 µg/mL and 5 strains with an MIC > 256 µg/mL of which 3 were B. thetaiotaomicron, 1 B. vulgatus and 1 B. distasonis.
Discussion
In this study we looked for Bacteroides fragilis group in 45 stools of which 24 (53.33%) were diarrheal and 21 (46.67%) non-diarrheal specimens. After culture and biochemical identification 51 isolates were identified amongst the Bacteroides fragilis group.
Biochemical identification revealed that B. thetaiotaomicron was the predominant species (31.37%) followed by B. uniformis (23.53%), B. eggerthii (17.65%), B. vulgatus (13.73%), B. caccae (5.88%), P. distasonis (3.92%), and B. ovatus and B. fragilis (1.96%), respectively.
In a study performed by Ferreira et al. (2010) in Brazil, the authors reported entirely different results, where P. distasonis was the major species (19.1%), followed by B. fragilis (17.0%), B. vulgatus (17.0%), B. caccae (2.1%) and P. merdae (2.1%).
In the case of diarrheal stools B. thetaiotaomicron and B. uniformis were the dominant species (13.73%, respectively), followed by B. eggerthii (11.76%).
We also found that B. thetaiotaomicron and B. eggerthii (27.27%, respectively) were the major species in diarrheal stools of children under 18 years old followed by B. uniformis (18.18%), B. caccae (13.64%), B. vulgatus (9.09%) and B. ovatus (4.54%) (Table 1).
Nakano and Avila-Campos (2004) reported in a study performed on stools of 15 children with diarrhea the isolation of 64 B. fragilis group strains of which 39 were B. fragilis,8 B. vulgatus,6 B. uniformis,6 P. distasonis and 5 B. ovatus. In our study we isolated a single strain of B. fragilis in diarrheal stool of a person older than 54 years (74 years).
As for the non-diarrheal stools, we found that B. thetaiotaomicron was the most frequent isolate (17.65%) followed by B. uniformis and B. vulgatus (9.80%, respectively), B. eggerthii (5.88%) and P. distasonis (1.96%).
Rodriguez et al. (2006) studied the prevalence of different species of the B. fragilis group; they analyzed 80 non-diarrheal stools and according to their results, B. uniformis and B. fragilis were the most frequent species (24.6% and 16.9%, respectively).
Antibiotic resistance
We studied the susceptibility of 51 isolates belonging to the Bacteroides fragilis group. We found that 60.78% and 88.24% of the investigated strains were susceptible to clavulanic acid combined with either amoxicillin or ticarcillin. Tazobactam combined with piperacillin provided results similar to those of ticarcillin plus clavulanic acid (88.24%).
Therefore, the non suscptibility rates for these three drugs were 39.21%, 11.76% and 11.76%, respectively (Table 2).
A higher rate of resistance to amoxicillin-clavulanic acid (40.5%) was observed in a study performed by Nakano and Avila-campos (2004) on 64 Bacteroides fragilis group strains isolated from children with diarrhea in Brazil.
Only 4% of resistance was detected in a study performed by Oteo et al. (2000) on 100 isolates of Bacteroides fragilis group isolated from fecal samples of healthy people in Madrid, Spain.
In our study, the highest activity was observed with imipenem and meropenem where 98% of strains were sensitive to these antibiotics molecules (we found that one of seven B. vulgatus strains isolated was resistant to imipenem and meropenem) (Table 2).
Nakano and Avila-Campos (2004) showed in their study that none of 64 Bacteroides fragilis group strains isolated from human feces were resistant to imipenem.
A very good activity of meropenem has been reported by Oteo et al. (2000) With 100% of susceptibility, but a higher rate of resistance was reported by Ferreira et al. (2010) (18.2%).
Concerning the cephalosporins, we found that 68.63% of the strains were susceptible to cefoxitin (non susceptibility rate = 31.37%) while 13.73% had intermediate susceptibility to cefotaxime (86.27% resistance) (Table 2).
Different rates of cefoxitin resistance have been reported in several studies performed by Nakano and Avila-Campos (2004) in Brazil (23.5%) and Oteo et al. (2000) in Spain (18%).
For quinolones, susceptibility to ofloxacine was 27.45% while moxifloxacin susceptibility was 86.27%.
The susceptibility to clindamycin was 54.9% (resistance = 45.1%) (Table 2).
Oteo et al. (2000) Ferreira et al. (2010) and Nakano and Avila-Campos (2004) reported high values of resistance (49%, 22.7% and 23.5%, respectively) in studies performed in Spain and Brazil.
In this study, the antibiotic susceptibilty to other molecules were: 92.16% to chloramphenicol (resistance = 7.84%) 82.24% to rifampicin (non susceptibility = 11.76%) and 84.31% to tigecycline (resistance = 15.69%).
Finally, we found a false susceptibility to kanamycin, colistin and vancomycin (3.92%, 9.80% and 7.84%, respectively) (Table 2), false sensitivity was detected because these three antibiotics are disks with special potency that helps to presumptive identification of anaerobes, they are not done to determine antibiotic susceptibility.
However some rare strains of the Bacteroides fragilis may have MIC of 16 mg/L and may appear susceptible to vancomycin.
In addition we didn't use disks with special potency aimed for the identification of anaerobes, instead we used regular disks.
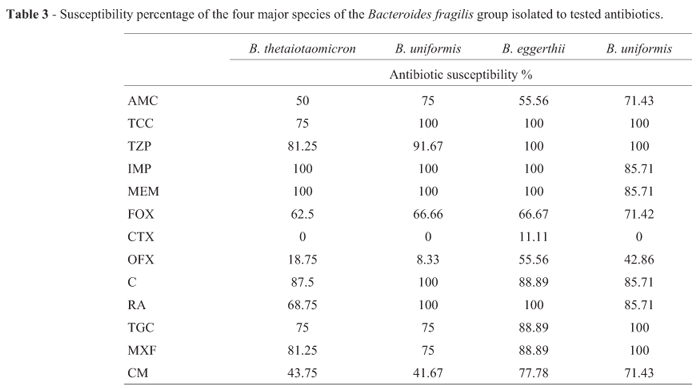
The highest non susceptibility rate to cefoxitin was observed in B. thetaiotaomicron (37.5%).
The highest non susceptibility rates to clindamycin, ofloxacin and moxifloxacin was observed in B. uniformis (58.33%, 75% and 91.67%, respectively).
The best susceptibility to moxifloxacin was observed for B.vulgatus (100%), followed by B. eggerthii (88.99%) and B. thetaiotaomicron (81.25%).
As for chloramphenicol, 100% of the isolates belonging to B. uniformis were susceptible, followed by B. eggerthii (88.89%) and B. thetaiotaomicron (87.5%).
100% of B. vulgatus isolates studied were susceptible to tigecycline followed by B. eggerthii (88.89%) and B. thetaiotaomicron and B. uniformis (75%, respectively) (Table 3).
Avelar et al. (2001) showed that P. distasonis was the most resistant species to cefoxitin and clindamycin in a study performed in Brazil on 73 strains of Bacteroides fragilis group.
Susceptibility to metronidazole
We determined the MIC of metronidazole for the 51 isolates by the E-test method.
We found that there were 6 resistant strains (11.76%), a strain belonging to the species thetaiotaomicron had a MIC = 64 mg/L and five strains had MIC values > 256 mg/L.
Note that a strain of B. vulgatus had a MIC = 0.016 mg/L, four strains of B.thetaitaomicron had MIC = 0.064 and 0.125 mg/L, respectively.
The rate of resistance is significantly higher compared to values reported in studies of strains isolated in Brazil and Spain (0%, respectively) (Ferreira et al., 2010; Nakano and Avila-Campos, 2004; Oteo et al., 2000).
Conclusion
Our study is original in nature as it is the first in Lebanon on the prevalence and distribution of the Bacteroides fragilis group species in diarrheal and non-diarrheal stools in North Lebanon.
Disk diffusion test may not be for some authors the best reference method, nevertheless this sudy allow document the general susceptibility of the B fragilis group strains in Lebanon.
The results showed that B. thetaiotaomicron was the most prevalent species in diarrheal and non-diarrheal stools.
We observed a high rate of resistance to cefoxitin (31.37%).
Imipenem and meropenem showed excellent activity (98% of susceptibility) meanwhile13.73% of our isolates were resistant to moxifloxacin. An alarming rate of resistance to clindamycin was observed (45.1%).
After the determination of MIC of metronidazole, the results showed that 11.76% of our strains were resistant.
It is advisable to continue this investigation, in attempt to identify genes that are involved in different resistance mechanisms observed. This study emphasizes the need for antibiotic surveys of anaerobes in the future.
Submitted: January 29, 2012;
Approved: September 10, 2012.
All the content of the journal, except where otherwise noted, is licensed under a Creative Commons License CC BY-NC.
- Aldridge KE, O'Brien M (2002) In vitro susceptibilities of Bacteroides fragilis group species: change in isolation rates significantly affects overall susceptibility data. J Clin Microbio 40:4349-4352.
- Aldridge KE (1995) The occurrence, virulence and antimicrobial resistance of anaerobes in polymicrobial infections. Am J Surg 169:2S-7S.
- Avelar KES, Vieira JMBD, Antunes LCM, Lobo LA Nazareno E, Antunes F et al. (2001) Antimicrobial resistance of strains of the Bacteroides fragilis group isolated from the intestinal tract of children and adults in Brazil. Int J Antimicro Ag 8:129-134.
- Bergan T (1983) Anaerobic bacteria as cause of infections in female genital organs. Scand J Gastro 85:37-47.
- Brook I (2002a) Endocarditis due to anaerobic bacteria. Cardiol 98:1-5.
- Brook I (2002b) Clinical review: bacteremia caused by anaerobic bacteria in children. Crit Care 6:205-211.
- Brook I (2002c) Microbiology of polymicrobial abscesses and implications for therapy. J Antimicrob Chemother 50:805-810.
- CA-SFM: Comité Antibiogramme de la Société Francaise de Microbiologie (2011) www.sfm-microbiologie.org
- Ferreira DA, Silva VL, Guimaraes AS, Coelho CM, Gomes Zauli DA, Farias LM et al. (2010) Distribution, detection of enterotoxigenic strains and antimicrobial drug susceptibility patterns of Bacteroides fragilis group in diarrheic and nondiarrheic feces from Brazilian infants. Braz J Microbiol 41:603-611.
- Goldstein EJ (1996) Anaerobic bacteremia. Clin Infect Dis 23:97-101.
- Holdeman LV, Good IJ, Moore WE (1976) Human fecal flora: variation in bacterial composition within individuals and a possible effect of emotional stress. App Environ Microbiol 31:359-375.
- Marchal N, Bourdon JL, Richard C (1982) les milieux de cultur pour l'isolement et l'identification biochimique des bactéries. Doin Éditeurs, Paris.
- Nakano V, Avila-Campos MJ (2004) Virulence markers and anti-microbial susceptibility of bacteria of the Bacteroides fragilis group isolated from stool of children with diarrhea in Sao Paulo, Brazil. Mem Inst Owsaldo Cruz 3:307-312.
- Ote J, Aracil B, Alos JI, Gomez-Garces, JI (2000) High prevalence of resistance to clindamycin in Bacteroides fragilis group isolates. J Antimicrob Chemother 45:691-693.
- Pumbwe L, Wareham DW, Aduse-Opoku J, Brazier JS, Wexler HM (2007) Genetic analysis of mechanisms of multidrug resistance in a clinical isolate of Bacteroides fragilis Clini Microbiol Infec 13:183-189.
- Rodriguez E, Gamboa MM, Rodriguez C, Vergas P (2006) Bacteroides fragilis group in non-diarrheal human feces and its antimicrobial susceptibility. Rev Esp Quim 4:357-362.
- Smith CJ, Rocha ER, Paster BJ (2006) The medically important Bacteroides spp. in health and diseas. Prokaryotes 7:381-427.
- Syndman DR, Jacobus NV, McDermott LA, Ruthazer R, Goldstein EJC, Finegold SM et al. (2002) National survey on the susceptibility of Bacteroides fragilis group: report and analysis of trends for 1997-2000. Clin Infect Dis 35:126-134.
- Wexler HM (2007) Bacteroides: the Good, the Bad, and the Nitty-Gritty. Clin Microbiol Rev 593-621.
Publication Dates
-
Publication in this collection
03 Feb 2014 -
Date of issue
Sept 2013
History
-
Received
29 Jan 2012 -
Accepted
10 Sept 2012