Abstract:
This in vitro study aimed to evaluate the volume of polymerization shrinkage (VS), gap (VG), and void (VV) using computerized microtomography (μCT) in bulk fill resin composites and conventional class I restorations, and to establish a correlation between these factors. Class I cavities (4 x 5 x 4 mm), C-factor = 4.2, were performed on caries-free human third molars and randomly divided into five groups (n = 6): FSI (Filtek Supreme XTE incremental insertion); FSS [(Filtek Supreme XTE single insertion(SI)]; TBF [(Tetric Bulk Fill: SI and manual filling (MF)]; SFM (Sonic Fill: SI/MF); and SFS (SonicFill: SI and sonic filling). The teeth were scanned and analyzed by μCT at T0, after filling the cavity with resin, and at T1, after polymerization for VG and VV, and for VS (T1-T0). There was statistically significant difference in VS in μCT for the FSI and FSS groups and between SFS and FSS as well as some difference in VV for FSI and bulk fill resin composites and no difference in VG between the conventional technique and bulk fill composites. Bulk fill resin composites presented similar VS and gap formation to those of incrementally inserted conventional resin composites. There is a moderate and weak positive correlation between polymerization shrinkage and gap formation and void, respectively. The final gap formation was more dependent on the initial gap than on polymerization shrinkage or void volume.
Keywords:
Polymerization; X-ray Microtomography; Composite Resins; Imaging; Three-Dimensional
Introduction
Resin composite (RC) performance has been the focus of many studies, mainly because of polymerization shrinkage and stress.11. Cramer NB, Stansbury JW, Bowman CN. Recent advances and developments in composite dental restorative materials. J Dent Res. 2011;90(4):402-16. https://doi.org/10.1177/0022034510381263
https://doi.org/10.1177/0022034510381263...
There is ample evidence that the stress resulting from polymerization shrinkage in RCs may have deleterious effects such as marginal infiltration, cuspal deflection, dental cracking, reduction in bond strength, low mechanical properties, and gap formation.22. Ferracane JL, Hilton TJ. Polymerization stress: is it clinically meaningful? Dent Mater. 2016;32(1):1-10. https://doi.org/10.1016/j.dental.2015.06.020
https://doi.org/10.1016/j.dental.2015.06...
The control of these clinically relevant effects is of fundamental importance. Major efforts have been put into the improvement and development of materials and techniques that use new polymerization strategies, and also into the control of their effects on the tooth/restoration interface.11. Cramer NB, Stansbury JW, Bowman CN. Recent advances and developments in composite dental restorative materials. J Dent Res. 2011;90(4):402-16. https://doi.org/10.1177/0022034510381263
https://doi.org/10.1177/0022034510381263...
,33. Ferracane JL. Resin composite: state of the art. Dent Mater. 2011;27(1):29-38. https://doi.org/10.1016/j.dental.2010.10.020
https://doi.org/10.1016/j.dental.2010.10...
During the polymerization of RCs, double and simple bonds of carbon monomers form polymer chains with covalent bonds, resulting in 1.5 to 5% of volumetric shrinkage.44. Ferracane JL. Developing a more complete understanding of stresses produced in dental composites during polymerization. Dent Mater. 2005;21(1):36-42. https://doi.org/10.1016/j.dental.2004.10.004
https://doi.org/10.1016/j.dental.2004.10...
When polymerization shrinkage is larger than the bond strength, it leads to the formation of marginal cracks, and such cracks may range from 1.67 to 5.68% of the total restoration volume.55. Davidson CL, Gee AJ, Feilzer A. The competition between the composite-dentin bond strength and the polymerization contraction stress. J Dent Res. 1984;63(12):1396-9. https://doi.org/10.1177/00220345840630121101
https://doi.org/10.1177/0022034584063012...
It should be noted that polymerization shrinkage is greatly influenced by the configuration factor (C-factor). Cavities with a higher C-factor may have lower internal adaptation of the restorative material.66. Han SH, Sadr A, Tagami J, Park SH. Internal adaptation of resin composites at two configurations: influence of polymerization shrinkage and stress. Dent Mater. 2016;32(9):1085-94. https://doi.org/10.1016/j.dental.2016.06.005
https://doi.org/10.1016/j.dental.2016.06...
The incremental filling technique has been recommended for decreasing polymerization shrinkage; however, it is very difficult to prove that the incremental technique needs to be maintained to reduce shrinkage effects.77. Versluis A, Douglas WH, Cross M, Sakaguchi RL. Does an incremental filling technique reduce polymerization shrinkage stresses? J Dent Res. 1996;75(3):871-8. https://doi.org/10.1177/00220345960750030301
https://doi.org/10.1177/0022034596075003...
Increasing the number of increments causes higher stress on the remaining tooth structure and at the tooth/restoration interface, as well as high post-gel shrinkage and/or elastic modulus values;88. Bicalho AA, Valdívia AD, Barreto BC, Tantbirojn D, Versluis A, Soares CJ. Incremental filling technique and composite material. Part II: shrinkage and shrinkage stresses. Oper Dent. 2014;39(2):E83-92. https://doi.org/10.2341/12-442-L
https://doi.org/10.2341/12-442-L...
in addition, the type of composite and filling technique affects the mechanical properties of large restorations.99. Bicalho AA, Pereira RD, Zanatta RF, Franco SD, Tantbirojn D, Versluis A et al. Incremental filling technique and composite material. Part I: cuspal deformation, bond strength, and physical properties. Oper Dent. 2014;39(2):E71-82. https://doi.org/10.2341/12-441-L
https://doi.org/10.2341/12-441-L...
In recent years, bulk fill RCs have been proposed to decrease polymerization shrinkage and gap formation in the pulp wall,1010. Kapoor N, Bahuguna N, Anand S. Influence of composite insertion technique on gap formation. J Conserv Dent. 2016;19(1):77-81. https://doi.org/10.4103/0972-0707.173205
https://doi.org/10.4103/0972-0707.173205...
inserted in a single thick layer (4–5 mm).1111. Ilie N, Bucuta S, Draenert M. Bulk-fill resin-based composites: an in vitro assessment of their mechanical performance. Oper Dent. 2013;38(6):618-25. https://doi.org/10.2341/12-395-L
https://doi.org/10.2341/12-395-L...
,1212. Zorzin J, Maier E, Harre S, Fey T, Belli R, Lohbauer U et al. Bulk-fill resin composites: polymerization properties and extended light curing. Dent Mater. 2015;31(3):293-301. https://doi.org/10.1016/j.dental.2014.12.010
https://doi.org/10.1016/j.dental.2014.12...
RCs seem to have low polymerization shrinkage and a small percentage of voids,1313. Ibarra ET, Lien W, Casey J, Dixon SA, Vandewalle KS. Physical properties of a new sonically placed composite resin restorative material. Gen Dent. 2015;63(3):51-6. besides large clinical acceptance,1414. Dijken JW, Pallesen U. Posterior bulk-filled resin composite restorations: A 5-year randomized controlled clinical study. J Dent. 2016;51:29-35. https://doi.org/10.1016/j.jdent.2016.05.008
https://doi.org/10.1016/j.jdent.2016.05....
,1515. Karaman E, Keskin B, Inan U. Three-year clinical evaluation of class II posterior composite restorations placed with different techniques and flowable composite linings in endodontically treated teeth. Clin Oral Investig. 2017;21(2):709-16. https://doi.org/10.1007/s00784-016-1940-y
https://doi.org/10.1007/s00784-016-1940-...
since they simplify the restorative process.1111. Ilie N, Bucuta S, Draenert M. Bulk-fill resin-based composites: an in vitro assessment of their mechanical performance. Oper Dent. 2013;38(6):618-25. https://doi.org/10.2341/12-395-L
https://doi.org/10.2341/12-395-L...
Another factor that should be considered is the sonic insertion of RCs as a way to reduce the size and number of spaces/voids in the material, as proposed by some manufacturers.1616. Jarisch J, Lien W, Guevara PH, Greenwood WJ, Dunn WJ. Microcomputed tomographic comparison of posterior composite resin restorative techniques: sonicated bulk fill versus incremental fill. Gen Dent. 2016;64(5):20-3.
Despite the great number of studies on polymerization shrinkage, the presence of voids and spaces in the restoration is a negative aspect that has been widely overlooked in the literature.1616. Jarisch J, Lien W, Guevara PH, Greenwood WJ, Dunn WJ. Microcomputed tomographic comparison of posterior composite resin restorative techniques: sonicated bulk fill versus incremental fill. Gen Dent. 2016;64(5):20-3. Voids and spaces may accelerate material deterioration, resulting in marginal infiltration and discoloration, higher wear, and lower flexural strength.1717. Opdam NJ, Roeters JJ, Peters TC, Burgersdijk RC, Teunis M. Cavity wall adaptation and voids in adhesive Class I resin composite restorations. Dent Mater. 1996;12(4):230-5. https://doi.org/10.1016/S0109-5641(96)80028-5
https://doi.org/10.1016/S0109-5641(96)80...
These spaces between the increments can be added during the manufacturing process or during RC insertion.1313. Ibarra ET, Lien W, Casey J, Dixon SA, Vandewalle KS. Physical properties of a new sonically placed composite resin restorative material. Gen Dent. 2015;63(3):51-6.,1818. Chadwick RG, McCabe JF, Walls AW, Storer R. The effect of placement technique upon the compressive strength and porosity of a composite resin. J Dent. 1989;17(5):230-3. https://doi.org/10.1016/0300-5712(89)90171-1
https://doi.org/10.1016/0300-5712(89)901...
Thus, it is recommended that handling of the material be minimal to prevent air from entering the matrix, which will end up forming voids and decreasing longevity.1818. Chadwick RG, McCabe JF, Walls AW, Storer R. The effect of placement technique upon the compressive strength and porosity of a composite resin. J Dent. 1989;17(5):230-3. https://doi.org/10.1016/0300-5712(89)90171-1
https://doi.org/10.1016/0300-5712(89)901...
Polymerization shrinkage and/or gap formation has been evaluated in the literature by means of different destructive tests,1919. Meleo D, Manzon L, Pecci R, Zuppante F, Bedini R. A proposal of microtomography evaluation for restoration interface gaps. Ann Ist Super Sanita. 2012;48(1):83-8.,2020. Agarwal RS, Hiremath H, Agarwal J, Garg A. Evaluation of cervical marginal and internal adaptation using newer bulk fill composites: an in vitro study. J Conserv Dent. 2015;18(1):56-61. https://doi.org/10.4103/0972-0707.148897
https://doi.org/10.4103/0972-0707.148897...
,2121. Campos EA, Ardu S, Lefever D, Jassé FF, Bortolotto T, Krejci I. Marginal adaptation of class II cavities restored with bulk-fill composites. J Dent. 2014;42(5):575-81. https://doi.org/10.1016/j.jdent.2014.02.007
https://doi.org/10.1016/j.jdent.2014.02....
,2222. Algamaiah H, Sampaio CS, Rigo LC, Janal MN, Giannini M, Bonfante EA et al. Microcomputed Tomography Evaluation of Volumetric Shrinkage of Bulk-Fill Composites in Class II Cavities. J Esthet Restor Dent. 2017;29(2):118-27. https://doi.org/10.1111/jerd.12275
https://doi.org/10.1111/jerd.12275...
,2323. Sampaio CS, Chiu KJ, Farrokhmanesh E, Janal M, Puppin-Rontani RM, Giannini M et al. Microcomputed Tomography Evaluation of Polymerization Shrinkage of Class I Flowable Resin Composite Restorations. Oper Dent. 2017;42(1):E16-23. https://doi.org/10.2341/15-296-L
https://doi.org/10.2341/15-296-L...
hindering a more detailed analysis of the resin composite body before and after polymerization. Computerized microtomography (μCT) has been used to quantify and evaluate polymerization shrinkage,2222. Algamaiah H, Sampaio CS, Rigo LC, Janal MN, Giannini M, Bonfante EA et al. Microcomputed Tomography Evaluation of Volumetric Shrinkage of Bulk-Fill Composites in Class II Cavities. J Esthet Restor Dent. 2017;29(2):118-27. https://doi.org/10.1111/jerd.12275
https://doi.org/10.1111/jerd.12275...
,2323. Sampaio CS, Chiu KJ, Farrokhmanesh E, Janal M, Puppin-Rontani RM, Giannini M et al. Microcomputed Tomography Evaluation of Polymerization Shrinkage of Class I Flowable Resin Composite Restorations. Oper Dent. 2017;42(1):E16-23. https://doi.org/10.2341/15-296-L
https://doi.org/10.2341/15-296-L...
in order to examine the tooth/restoration interface, as well as other changes in the material. This type of analysis eliminates the need for cuts and stresses to the tooth, unlike other methods, such as scanning electron microscopy (SEM).1919. Meleo D, Manzon L, Pecci R, Zuppante F, Bedini R. A proposal of microtomography evaluation for restoration interface gaps. Ann Ist Super Sanita. 2012;48(1):83-8. μCT is a safe and nondestructive method that can analyze the material in 3D,2424. Carrera CA, Lan C, Escobar-Sanabria D, Li Y, Rudney J, Aparicio C et al. The use of micro-CT with image segmentation to quantify leakage in dental restorations. Dent Mater. 2015;31(4):382-90. https://doi.org/10.1016/j.dental.2015.01.002
https://doi.org/10.1016/j.dental.2015.01...
but it is infrequently used to quantify spaces and voids in restorative materials.1616. Jarisch J, Lien W, Guevara PH, Greenwood WJ, Dunn WJ. Microcomputed tomographic comparison of posterior composite resin restorative techniques: sonicated bulk fill versus incremental fill. Gen Dent. 2016;64(5):20-3.
Few studies have shown the behavior of manually and sonically inserted bulk fill RCs towards polymerization shrinkage, gap, and void formation in large class I restorations. Thus, this in vitro study aimed to correlate polymerization shrinkage, gap, and void in high C-factor cavities restored with conventional composites and bulk fill, using μCT for the analysis. The following null hypotheses were tested: a) there is no difference in the volume of polymerization shrinkage (VS), gap (VG), and void (VV) between bulk fill and conventional RCs; and b) there is no correlation between polymerization shrinkage, gap, and void in bulk fill and conventional RCs.
Methodology
This study was approved by the local Human Research Ethics Committee (process no. 1708531).
Sample preparation
Thirty caries-free, recently extracted human third molars were previously selected by crown size using a digital caliper (Mitutoyo Co., Tokyo, Japan), and cleaned and stored in thymol at 0.5%. Subsequently, prophylaxis and storage of the teeth were carried out in distilled water at 37 ± 1ºC (24 h). Standard class I cavities (4 x 5 x 4 mm) with a high C-factor (C = 4.2) were made with diamond tips No. 1090 and 1014 (KG SORENSEN, Cotia, Brazil) at high rotation under refrigeration. The diamond tips had a standardized active tip and a vertical stop to provide equal depth during preparation of the wells. At the end of the preparation, the cavities were measured with a digital caliper. The diamond tips were replaced after every five cavity preparations.2323. Sampaio CS, Chiu KJ, Farrokhmanesh E, Janal M, Puppin-Rontani RM, Giannini M et al. Microcomputed Tomography Evaluation of Polymerization Shrinkage of Class I Flowable Resin Composite Restorations. Oper Dent. 2017;42(1):E16-23. https://doi.org/10.2341/15-296-L
https://doi.org/10.2341/15-296-L...
The live internal angles were rounded with tip 10142121. Campos EA, Ardu S, Lefever D, Jassé FF, Bortolotto T, Krejci I. Marginal adaptation of class II cavities restored with bulk-fill composites. J Dent. 2014;42(5):575-81. https://doi.org/10.1016/j.jdent.2014.02.007
https://doi.org/10.1016/j.jdent.2014.02....
in order to facilitate material adaptation and force dissipation. After cavity preparation, the teeth were randomly divided to the following groups (n = 6 each): group 1 = FSI (Filtek Supreme XTE - incremental insertion); group 2 = FSS (Filtek Supreme XTE - single insertion); group 3 = TBF (Tetric Bulk Fill – manual filling); group 4 = SFM (SonicFill - manual filling); and group 5 = SFS (SonicFill – sonic filling). The restorative materials and their respective insertion/filling information and techniques are described in Table 1.
Restorative procedure
After preparation of the samples, enamel and dentin were etched with phosphoric acid at 37% (FGM, Joinville, SC, Brazil) for 30 and 15 s, respectively, followed by rinsing for 20 s. Excess water was removed with thin absorbent paper, followed by the application of Adper Single Bond 2 adhesive (3M, ESPE, ST Paul, USA) according to the manufacturer's instructions and then light-cured for 10 s with a high-power LED polymerization apparatus (Bluephase, Ivoclar Vivadent AG, Austria). The samples were protected from any light sources in dark plastic vials and placed in the microtomograph for scanning and volume quantification before light curing. In the microtomograph, there was no light incidence once Skyscan 1176 (V. 1.1.10, Skyscan, Kontich, Antwerp, Belgium) operational protocol uses a dark environment. Resin composite material was inserted in each of the groups as described in Table 1, and condensation was performed with a cosmedent SP2 spatula (Cosmedent, Chicago, USA). All increments were light-cured for 40 s with 1200 mW/cm2.2525. Van Ende A, De Munck J, Van Landuyt K, Van Meerbeek B. Effect of Bulk-filling on the Bonding Efficacy in Occlusal Class I Cavities. J Adhes Dent. 2016;18(2):119-24. The same operator performed all the restorative procedures. The specimens were then stored in distilled water and kept in an oven at 37°C ± 1°C for 24 h.
Computerized microtomography (μCT)
Computerized microtomography was used to analyze the restored cavities. Each tooth was scanned twice: at T0 – after insertion of the RC material, and at T1 – after the final cure. The microtomograph used a power of 90 Kvp and 275 microamperes with a resolution of 17.48 μm (Cu filter = 0.1 mm). The total number of slices averaged 250, with an average reading time close to 28 min.
The μCT data were then imported into a workstation and evaluated with the NRecon software (Version, 1.6.10.4-2015, Skyscan, Kontich, Antwerp, Belgium). The threshold was standardized by an average of the base algorithm for the components of the control group, thus eliminating any bias between the samples. The images were standardized using the DataViewer (V.1.5.2.4) software and the analyses were performed through the 3D analysis tool from CTAn (CT-Analyser software v1.10.1.0; Skyscan, Kontich, Belgium) based on the volume of black spaces (void spaces) present in the volume of interest (VOI), which consisted of the summation of all 2D images within the region of interest (ROI). In the CTVol software, the two scan images were superimposed, allowing us to get a good arrangement. All calculations were performed using the VOI obtained from the ROI centered on the delimitations of the restorative material (Figure 1).
3D reconstruction of cavity filled with resin composites. Illustrative 2D slice showing the region of interest - ROI (Figure A - red square). Restoration at different angles (B, C, D, and E).
The initial reading (T0) was considered “reference,” and the final reading (T1) was considered a “target” for the geometric alignment of the images. The reference and target images were analyzed individually, and shrinkage, gap, and void were determined by the difference between the reference and target samples. The volume of polymerization shrinkage, gap, and void was calculated through the analysis of the anatomical structure of the restoration and was expressed as percentage.2424. Carrera CA, Lan C, Escobar-Sanabria D, Li Y, Rudney J, Aparicio C et al. The use of micro-CT with image segmentation to quantify leakage in dental restorations. Dent Mater. 2015;31(4):382-90. https://doi.org/10.1016/j.dental.2015.01.002
https://doi.org/10.1016/j.dental.2015.01...
Sample size calculation
The data were analyzed by the STATA 14 (College Station, USA) software. Sample size, taking into account inter-group variation (147.2) and intra-group variation (104.8), as reported elsewhere,2626. Fronza BM, Rueggeberg FA, Braga RR, Mogilevych B, Soares LE, Martin AA et al. Monomer conversion, microhardness, internal marginal adaptation, and shrinkage stress of bulk-fill resin composites. Dent Mater. 2015;31(12):1542-51. https://doi.org/10.1016/j.dental.2015.10.001
https://doi.org/10.1016/j.dental.2015.10...
resulted in four specimens per group with a statistical power of 80% and an alpha of 5%.
Statistical analysis
The Shapiro-Wilk test indicated that, among the three evaluated outcomes, polymerization shrinkage and void values were not normally distributed. These data were analyzed using the Kruskal-Wallis test, followed by Dunn's post-hoc test. ANOVA was used for the gap volume, followed by Tukey's test. The correlation between the volume of shrinkage, void, and gap was obtained by Spearman's rank correlation coefficient. A multivariable linear regression was performed to model the relationship between the final gap (dependent variable) and the initial gap, VS and VV (independent variables). In all analyses, the significance level was set as p < 0.05.
Results
The results of the μCT analysis were expressed as a percentage of volumetric polymerization shrinkage, gap, and void.
Volume of polymerization shrinkage (VS)
Unlike the evaluation of the volume of gap (VG) and void (VV), the analysis of volumetric polymerization shrinkage (VS) took into account the difference in the volume of RCs in each time period (T1-T0) as that represents the shrinkage of the studied material. All of the RCs exhibited polymerization shrinkage (SFI < TBF and FSI < SFM < FSS). A statistically significant difference was observed in the volume of polymerization shrinkage between FSI and FSS (p = 0.03) and between SFS and FSS (p = 0.01) (Table 2).
Volume of polymerization shrinkage (VS), gap (VG), and void (VV) using µCT (mean/SD* * Means with the same superscript letters are not statistically different from each other (p < 0.05). ).
Volume of gap (VG)
Gap volume was measured at nine different points from the pulp wall to the restoration (Figure 2), and the sum of these points determined the total volume of gap per tooth at two different moments: VG0 and VG1. The analysis of the gap and void volume on two different occasions sought to show the presence of gap after RC resin composite insertion and after polymerization of the material. Note that the difference between the final and initial times only shows the size of the gap increase rather than its real volume before and after polymerization.
The presence of gap at the tooth/restoration interface was observed in all groups before (VG0) and after (VG1) light curing (Table 2 and Figure 3). Group 4 (SFM) presented greater gap formation before and after light curing. There was no significant statistical difference in the presence of gap between the groups on the two occasions: before (Kruskal-Wallis, p = 0.43) and after light curing (p = 0.64) (Table 2).
Presence of gaps and voids in the resins before (0) and after (1) light curing indicated by arrows in the μCT (red=gap; yellow=void). FSI: Filtek Supreme XTE - incremental insertion; FSS: Filtek Supreme XTE - single insertion; TBF: Tetric Bulk Fill; SFM: SonicFill - manual filling; SFS: SonicFill - sonic filling.
Volume of void (VV)
The void volume was considered for all spaces, voids, and porosity observed in the body of the material before (VV0) and after light curing (VV1). The groups treated with conventional RCs were those with the lowest void volume. The analysis of VV was similar to that of VG and showed a statistically significant difference at VV0 between FSI and TBF (p < 0.001), FSI and SFM (p= 0.008), FSI and SFS (p = 0.003), and FSS and TBF (p = 0.01). In the same way, some difference in RCs was observed at VV1 for FSI and TBF (p = 0.001), FSI and SFM (p = 0.02), and FSI and SFS (p = 0.01).
Correlation between the volume of shrinkage, gap, and void
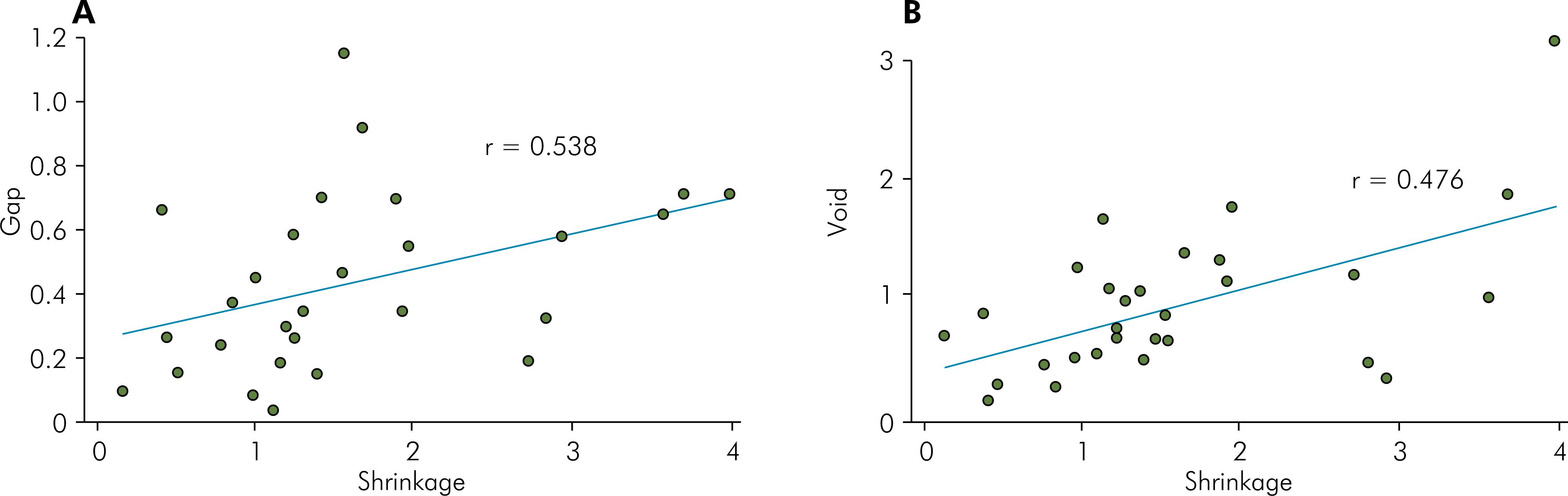
A moderate positive correlation (p = 0.003, r = 0.538) was observed between the volume of shrinkage (%VS) and the volume of the final gap (%VG1) (Figure 4A), whereas there was a weak positive correlation between the volume of polymerization shrinkage (%VS) and the volume of the final void (%VV1) (Figure 4B, p = 0.009, r = 0.476).
A – Correlation between volume of polymerization shrinkage and final gap in the pulp wall at the resin/tooth interface (p = 0.003). B – Correlation between volume of polymerization shrinkage and final void (p = 0.009).
The linear regression model explained 89% of the variation in the final gap. The initial gap was the main factor related to the final gap (p < 0.001). For each 1-mm3 increase in the initial gap, the final gap increased by 0.95 mm33. Ferracane JL. Resin composite: state of the art. Dent Mater. 2011;27(1):29-38. https://doi.org/10.1016/j.dental.2010.10.020
https://doi.org/10.1016/j.dental.2010.10...
, maintaining VV and VS constant.
Discussion
The results of the present study demonstrate that, regardless of the insertion and filling technique, all RCs exhibited polymerization shrinkage, gap, and void. The first null hypothesis was partially rejected because there was a difference between the volume of polymerization shrinkage for FSI and FSS and for SFS and FSS, in addition to a void for FSI and bulk fill RCs; however, no difference was found for gap volume (VG) between bulk fill and conventional RCs. The second null hypothesis was rejected because there was a positive correlation between polymerization shrinkage and gap and void in the studied RCs.
In recent years, μCT has become an important tool in the analysis of polymerization shrinkage,2222. Algamaiah H, Sampaio CS, Rigo LC, Janal MN, Giannini M, Bonfante EA et al. Microcomputed Tomography Evaluation of Volumetric Shrinkage of Bulk-Fill Composites in Class II Cavities. J Esthet Restor Dent. 2017;29(2):118-27. https://doi.org/10.1111/jerd.12275
https://doi.org/10.1111/jerd.12275...
,2323. Sampaio CS, Chiu KJ, Farrokhmanesh E, Janal M, Puppin-Rontani RM, Giannini M et al. Microcomputed Tomography Evaluation of Polymerization Shrinkage of Class I Flowable Resin Composite Restorations. Oper Dent. 2017;42(1):E16-23. https://doi.org/10.2341/15-296-L
https://doi.org/10.2341/15-296-L...
gap formation,2424. Carrera CA, Lan C, Escobar-Sanabria D, Li Y, Rudney J, Aparicio C et al. The use of micro-CT with image segmentation to quantify leakage in dental restorations. Dent Mater. 2015;31(4):382-90. https://doi.org/10.1016/j.dental.2015.01.002
https://doi.org/10.1016/j.dental.2015.01...
and void.1616. Jarisch J, Lien W, Guevara PH, Greenwood WJ, Dunn WJ. Microcomputed tomographic comparison of posterior composite resin restorative techniques: sonicated bulk fill versus incremental fill. Gen Dent. 2016;64(5):20-3. μCT can produce quantitative analyses of polymerization shrinkage when compared with conventional methods, which are qualitative or semiquantitative.2727. Zeiger DN, Sun J, Schumacher GE, Lin-Gibson S. Evaluation of dental composite shrinkage and leakage in extracted teeth using X-ray microcomputed tomography. Dent Mater. 2009;25(10):1213-20. https://doi.org/10.1016/j.dental.2009.04.007
https://doi.org/10.1016/j.dental.2009.04...
Also, this type of analysis does not cause stress, deterioration, cracking, or destruction of the sample, thus allowing for the sample to be analyzed in 3D before and after treatment without interfering in the experiment, unlike SEM1919. Meleo D, Manzon L, Pecci R, Zuppante F, Bedini R. A proposal of microtomography evaluation for restoration interface gaps. Ann Ist Super Sanita. 2012;48(1):83-8. and other 2D methods.
The volume of polymerization shrinkage of the materials investigated in this study ranged from 1.01 to 2.91%, which is an acceptable value, according to the literature.44. Ferracane JL. Developing a more complete understanding of stresses produced in dental composites during polymerization. Dent Mater. 2005;21(1):36-42. https://doi.org/10.1016/j.dental.2004.10.004
https://doi.org/10.1016/j.dental.2004.10...
The low shrinkage values observed in the analyzed RCs may be explained by the increase in inorganic load,2828. Braga RR, Ballester RY, Ferracane JL. Factors involved in the development of polymerization shrinkage stress in resin-composites: a systematic review. Dent Mater. 200521(10):962-70. https://doi.org/10.1016/j.dental.2005.04.018
https://doi.org/10.1016/j.dental.2005.04...
since it is known that RCs with a lower fill load may have a shrinkage greater than those with a higher load. In addition, all methacrylate-based RCs shrink to some extent, and shrinkage can be reduced by using monomers with a high molecular weight.2929. Al Sunbul H, Silikas N, Watts DC. Polymerization shrinkage kinetics and shrinkage-stress in dental resin-composites. Dent Mater. 2016;32(8):998-1006. https://doi.org/10.1016/j.dental.2016.05.006
https://doi.org/10.1016/j.dental.2016.05...
Higher polymerization shrinkage was observed in FSS, and this can be explained by the application of single-increment RC (4 mm) instead of the incremental filling recommended by the manufacturer (Table 1). Shrinkage in the incremental technique was similar to that of bulk fill RCs, but the incremental filling technique increases the deformation of the restored tooth, which could be a negative outcome due to higher stress on the tooth-composite structure.77. Versluis A, Douglas WH, Cross M, Sakaguchi RL. Does an incremental filling technique reduce polymerization shrinkage stresses? J Dent Res. 1996;75(3):871-8. https://doi.org/10.1177/00220345960750030301
https://doi.org/10.1177/0022034596075003...
However, in this study, μCT did not allow us to measure polymerization shrinkage stress.
Low shrinkage values were observed for SFS, and this could perhaps be explained by the modification of the charging behavior of the particles, which possibly minimizes the stress generated by polymerization shrinkage, and also by the fact that methacrylate-based resins, such as SonicFill, decrease shrinkage, to some extent, with the use of high molecular weight monomers, since the nature of the monomer determines the amount of bulk shrinkage during polymerization and the resulting stress.2929. Al Sunbul H, Silikas N, Watts DC. Polymerization shrinkage kinetics and shrinkage-stress in dental resin-composites. Dent Mater. 2016;32(8):998-1006. https://doi.org/10.1016/j.dental.2016.05.006
https://doi.org/10.1016/j.dental.2016.05...
SonicFill was not better than the manual insertion of this same resin composite or than Tetric Bulk Fill for the shrinkage volume, nor did it differ in the FSI. Benetti et al.3030. Benetti AR, Havndrup-Pedersen C, Honoré D, Pedersen MK, Pallesen U. Bulk-fill resin composites: polymerization contraction, depth of cure, and gap formation. Oper Dent. 2015;40(2):190-200. https://doi.org/10.2341/13-324-L
https://doi.org/10.2341/13-324-L...
also did not observe any difference in polymerization shrinkage between SFS and TBF, but class II cavities were analyzed through a linear variable differential transformer (LVDT). On the other hand, Orlowski et al.3131. Orłowski M, Tarczydło B, Chałas R. Evaluation of marginal integrity of four bulk-fill dental composite materials: in vitro study. Sci World J. 2015;2015:701262. https://doi.org/10.1155/2015/701262
https://doi.org/10.1155/2015/701262...
observed better results for SFS than for TBF; however, their work verified the marginal sealing of cavities and not polymerization shrinkage.
All cavities presented a gap at the interface between the RC and the pulp wall (Figure 3), and the final gap volume ranged from 1.97 to 2.95% between the groups. In this study, the sonic filling technique (SFS) did not influence the lower gap formation, because the manually inserted bulk fill RCs (SFM and TBF) did not differ statistically from the sonically inserted ones. In addition, Benetti et al.,3030. Benetti AR, Havndrup-Pedersen C, Honoré D, Pedersen MK, Pallesen U. Bulk-fill resin composites: polymerization contraction, depth of cure, and gap formation. Oper Dent. 2015;40(2):190-200. https://doi.org/10.2341/13-324-L
https://doi.org/10.2341/13-324-L...
when using an LVDT and an electron microscope, did not observe any difference in polymerization shrinkage, gap formation, and polymerization depth between SFS and TBF in class II cavities. However, Kapoor et al.1010. Kapoor N, Bahuguna N, Anand S. Influence of composite insertion technique on gap formation. J Conserv Dent. 2016;19(1):77-81. https://doi.org/10.4103/0972-0707.173205
https://doi.org/10.4103/0972-0707.173205...
found better adaptability and lower gap formation in the pulp wall when bulk fill RCs were used compared with conventional RCs, but the analysis was made by SEM, which may raise some doubts about final gap formation.1919. Meleo D, Manzon L, Pecci R, Zuppante F, Bedini R. A proposal of microtomography evaluation for restoration interface gaps. Ann Ist Super Sanita. 2012;48(1):83-8.
Gap formation is a complex phenomenon and depends on the interaction of several factors.3030. Benetti AR, Havndrup-Pedersen C, Honoré D, Pedersen MK, Pallesen U. Bulk-fill resin composites: polymerization contraction, depth of cure, and gap formation. Oper Dent. 2015;40(2):190-200. https://doi.org/10.2341/13-324-L
https://doi.org/10.2341/13-324-L...
Polymerization shrinkage is not the only factor involved in gap formation around the cavity edges, as some other factors, such as cuspal deflection,3232. Moorthy A, Hogg CH, Dowling AH, Grufferty BF, Benetti AR, Fleming GJ. Cuspal deflection and microleakage in premolar teeth restored with bulk-fill flowable resin-based composite base materials. J Dent. 2012;40(6):500-5. https://doi.org/10.1016/j.jdent.2012.02.015
https://doi.org/10.1016/j.jdent.2012.02....
type of cavity,66. Han SH, Sadr A, Tagami J, Park SH. Internal adaptation of resin composites at two configurations: influence of polymerization shrinkage and stress. Dent Mater. 2016;32(9):1085-94. https://doi.org/10.1016/j.dental.2016.06.005
https://doi.org/10.1016/j.dental.2016.06...
,3030. Benetti AR, Havndrup-Pedersen C, Honoré D, Pedersen MK, Pallesen U. Bulk-fill resin composites: polymerization contraction, depth of cure, and gap formation. Oper Dent. 2015;40(2):190-200. https://doi.org/10.2341/13-324-L
https://doi.org/10.2341/13-324-L...
and insertion technique,1010. Kapoor N, Bahuguna N, Anand S. Influence of composite insertion technique on gap formation. J Conserv Dent. 2016;19(1):77-81. https://doi.org/10.4103/0972-0707.173205
https://doi.org/10.4103/0972-0707.173205...
may also generate a gap. However, observing the presence of a gap in SEM or through other destructive tests creates uncertainty about whether the gap formed before and/or after light curing, because the preparation of the sample can cause stress and deterioration at the tooth/restoration interface, casting doubt about whether the gap occurred before or after light curing or if the failure was caused by the insertion technique or if different areas, mainly near the angles, were not properly selected in the cuts. Therefore, the analysis in μCT has become an accurate, safe, and non-destructive method for evaluating these materials in 3D.1919. Meleo D, Manzon L, Pecci R, Zuppante F, Bedini R. A proposal of microtomography evaluation for restoration interface gaps. Ann Ist Super Sanita. 2012;48(1):83-8.,2424. Carrera CA, Lan C, Escobar-Sanabria D, Li Y, Rudney J, Aparicio C et al. The use of micro-CT with image segmentation to quantify leakage in dental restorations. Dent Mater. 2015;31(4):382-90. https://doi.org/10.1016/j.dental.2015.01.002
https://doi.org/10.1016/j.dental.2015.01...
Both bulk fill and conventional RCs presented voids in the body of the material (Table 2), but a smaller void volume was found for conventional RCs. There was no difference in void volume among bulk fill composites. According to the literature, the handling of RCs by the operator should be minimized to prevent the formation of air bubbles.1818. Chadwick RG, McCabe JF, Walls AW, Storer R. The effect of placement technique upon the compressive strength and porosity of a composite resin. J Dent. 1989;17(5):230-3. https://doi.org/10.1016/0300-5712(89)90171-1
https://doi.org/10.1016/0300-5712(89)901...
Restoring cavities, especially deep ones, with 2-mm-thick increments is time-consuming and implies the risk of entrapment of air bubbles during the incremental technique.3333. Flury S, Hayoz S, Peutzfeldt A, Hüsler J, Lussi A. Depth of cure of resin composites: is the ISO 4049 method suitable for bulk fill materials? Dent Mater. 2012;28(5):521-8. https://doi.org/10.1016/j.dental.2012.02.002
https://doi.org/10.1016/j.dental.2012.02...
However, in the present study, the insertion/condensation of conventional RCs by the incremental technique eventually reduced the number of voids in the body of the material when compared with the sonic and manual technique of bulk fill RCs; one hypothesis is that spatulation could reduce the number of bubbles or other defects present in the matrix during the manufacture of the material.
The results of the present study indicate a moderate positive correlation between polymerization shrinkage and gap formation. In the literature,3030. Benetti AR, Havndrup-Pedersen C, Honoré D, Pedersen MK, Pallesen U. Bulk-fill resin composites: polymerization contraction, depth of cure, and gap formation. Oper Dent. 2015;40(2):190-200. https://doi.org/10.2341/13-324-L
https://doi.org/10.2341/13-324-L...
there is a strong positive correlation; however, polymerization shrinkage was analyzed through LVDT and gap formation was evaluated with a visible scale in the microscope objective. This correlation, as found in the present study and in the literature, demonstrates that there is an association between polymerization shrinkage and the final gap, but other factors should be considered as well. The small difference between the final and initial gaps is proportional to the observed polymerization shrinkage. However, the presence of the final gap in the restoration seems to be associated more with insertion of the material in the cavity (initial gap) than with polymerization shrinkage. This fact had not been previously described in the literature, and the linear regression model performed in the present study explained 89% of the final gap variation, where the initial gap was the main associated factor. For each 1-mm33. Ferracane JL. Resin composite: state of the art. Dent Mater. 2011;27(1):29-38. https://doi.org/10.1016/j.dental.2010.10.020
https://doi.org/10.1016/j.dental.2010.10...
increase in the initial gap, the final gap increased by 0.95 mm33. Ferracane JL. Resin composite: state of the art. Dent Mater. 2011;27(1):29-38. https://doi.org/10.1016/j.dental.2010.10.020
https://doi.org/10.1016/j.dental.2010.10...
, maintaining the void volume and polymerization shrinkage constant.
The correlation between void volume and polymerization shrinkage was weak (Figure 4B). The regression analysis showed that 94.5% of the void volume increased, that is, the final void volume was due to polymerization shrinkage. A possible explanation for these findings is that molecular rearrangement of monomers in a smaller space3434. Bausch JR, de Lange K, Davidson CL, Peters A, de Gee AJ. Clinical significance of polymerization shrinkage of composite resins. J Prosthet Dent. 1982;48(1):59-67. https://doi.org/10.1016/0022-3913(82)90048-8PMID:6955507
https://doi.org/10.1016/0022-3913(82)900...
and the internally generated polymerization shrinkage forces3535. Bowen RL. Adhesive bonding of various materials to hard tooth tissues. VI. Forces developing in direct-filling materials during hardening. J Am Dent Assoc. 1967;74(3):439-45. https://doi.org/10.14219/jada.archive.1967.0078
https://doi.org/10.14219/jada.archive.19...
would increase the gap/void around this region. However, further in vitro studies should be conducted to assess polymerization shrinkage, gap formation, and void in the material, taking into account factors associated with polymerization shrinkage stress in bulk fill RCs.
Conclusions
The sonic and manual insertion of bulk fill RCs in large cavities shows polymerization shrinkage and gap formation similar to those observed in conventional nanoparticle-filled RCs subjected to the incremental technique. There are moderate and weak positive correlations between polymerization shrinkage and gap formation and between polymerization shrinkage and voids, respectively, and final gap formation is more dependent on the initial gap than on polymerization shrinkage or on void volume.
Acknowledgments
The authors thank Fapema (Research Foundation of Maranhão) for the financial support and also support the notice (Universal Notice no. 40/2016, PAEDT Notice No. 16/2015). The authors thank Unesp-Araraquara for its support and technical assistance.
References
-
1Cramer NB, Stansbury JW, Bowman CN. Recent advances and developments in composite dental restorative materials. J Dent Res. 2011;90(4):402-16. https://doi.org/10.1177/0022034510381263
» https://doi.org/10.1177/0022034510381263 -
2Ferracane JL, Hilton TJ. Polymerization stress: is it clinically meaningful? Dent Mater. 2016;32(1):1-10. https://doi.org/10.1016/j.dental.2015.06.020
» https://doi.org/10.1016/j.dental.2015.06.020 -
3Ferracane JL. Resin composite: state of the art. Dent Mater. 2011;27(1):29-38. https://doi.org/10.1016/j.dental.2010.10.020
» https://doi.org/10.1016/j.dental.2010.10.020 -
4Ferracane JL. Developing a more complete understanding of stresses produced in dental composites during polymerization. Dent Mater. 2005;21(1):36-42. https://doi.org/10.1016/j.dental.2004.10.004
» https://doi.org/10.1016/j.dental.2004.10.004 -
5Davidson CL, Gee AJ, Feilzer A. The competition between the composite-dentin bond strength and the polymerization contraction stress. J Dent Res. 1984;63(12):1396-9. https://doi.org/10.1177/00220345840630121101
» https://doi.org/10.1177/00220345840630121101 -
6Han SH, Sadr A, Tagami J, Park SH. Internal adaptation of resin composites at two configurations: influence of polymerization shrinkage and stress. Dent Mater. 2016;32(9):1085-94. https://doi.org/10.1016/j.dental.2016.06.005
» https://doi.org/10.1016/j.dental.2016.06.005 -
7Versluis A, Douglas WH, Cross M, Sakaguchi RL. Does an incremental filling technique reduce polymerization shrinkage stresses? J Dent Res. 1996;75(3):871-8. https://doi.org/10.1177/00220345960750030301
» https://doi.org/10.1177/00220345960750030301 -
8Bicalho AA, Valdívia AD, Barreto BC, Tantbirojn D, Versluis A, Soares CJ. Incremental filling technique and composite material. Part II: shrinkage and shrinkage stresses. Oper Dent. 2014;39(2):E83-92. https://doi.org/10.2341/12-442-L
» https://doi.org/10.2341/12-442-L -
9Bicalho AA, Pereira RD, Zanatta RF, Franco SD, Tantbirojn D, Versluis A et al. Incremental filling technique and composite material. Part I: cuspal deformation, bond strength, and physical properties. Oper Dent. 2014;39(2):E71-82. https://doi.org/10.2341/12-441-L
» https://doi.org/10.2341/12-441-L -
10Kapoor N, Bahuguna N, Anand S. Influence of composite insertion technique on gap formation. J Conserv Dent. 2016;19(1):77-81. https://doi.org/10.4103/0972-0707.173205
» https://doi.org/10.4103/0972-0707.173205 -
11Ilie N, Bucuta S, Draenert M. Bulk-fill resin-based composites: an in vitro assessment of their mechanical performance. Oper Dent. 2013;38(6):618-25. https://doi.org/10.2341/12-395-L
» https://doi.org/10.2341/12-395-L -
12Zorzin J, Maier E, Harre S, Fey T, Belli R, Lohbauer U et al. Bulk-fill resin composites: polymerization properties and extended light curing. Dent Mater. 2015;31(3):293-301. https://doi.org/10.1016/j.dental.2014.12.010
» https://doi.org/10.1016/j.dental.2014.12.010 -
13Ibarra ET, Lien W, Casey J, Dixon SA, Vandewalle KS. Physical properties of a new sonically placed composite resin restorative material. Gen Dent. 2015;63(3):51-6.
-
14Dijken JW, Pallesen U. Posterior bulk-filled resin composite restorations: A 5-year randomized controlled clinical study. J Dent. 2016;51:29-35. https://doi.org/10.1016/j.jdent.2016.05.008
» https://doi.org/10.1016/j.jdent.2016.05.008 -
15Karaman E, Keskin B, Inan U. Three-year clinical evaluation of class II posterior composite restorations placed with different techniques and flowable composite linings in endodontically treated teeth. Clin Oral Investig. 2017;21(2):709-16. https://doi.org/10.1007/s00784-016-1940-y
» https://doi.org/10.1007/s00784-016-1940-y -
16Jarisch J, Lien W, Guevara PH, Greenwood WJ, Dunn WJ. Microcomputed tomographic comparison of posterior composite resin restorative techniques: sonicated bulk fill versus incremental fill. Gen Dent. 2016;64(5):20-3.
-
17Opdam NJ, Roeters JJ, Peters TC, Burgersdijk RC, Teunis M. Cavity wall adaptation and voids in adhesive Class I resin composite restorations. Dent Mater. 1996;12(4):230-5. https://doi.org/10.1016/S0109-5641(96)80028-5
» https://doi.org/10.1016/S0109-5641(96)80028-5 -
18Chadwick RG, McCabe JF, Walls AW, Storer R. The effect of placement technique upon the compressive strength and porosity of a composite resin. J Dent. 1989;17(5):230-3. https://doi.org/10.1016/0300-5712(89)90171-1
» https://doi.org/10.1016/0300-5712(89)90171-1 -
19Meleo D, Manzon L, Pecci R, Zuppante F, Bedini R. A proposal of microtomography evaluation for restoration interface gaps. Ann Ist Super Sanita. 2012;48(1):83-8.
-
20Agarwal RS, Hiremath H, Agarwal J, Garg A. Evaluation of cervical marginal and internal adaptation using newer bulk fill composites: an in vitro study. J Conserv Dent. 2015;18(1):56-61. https://doi.org/10.4103/0972-0707.148897
» https://doi.org/10.4103/0972-0707.148897 -
21Campos EA, Ardu S, Lefever D, Jassé FF, Bortolotto T, Krejci I. Marginal adaptation of class II cavities restored with bulk-fill composites. J Dent. 2014;42(5):575-81. https://doi.org/10.1016/j.jdent.2014.02.007
» https://doi.org/10.1016/j.jdent.2014.02.007 -
22Algamaiah H, Sampaio CS, Rigo LC, Janal MN, Giannini M, Bonfante EA et al. Microcomputed Tomography Evaluation of Volumetric Shrinkage of Bulk-Fill Composites in Class II Cavities. J Esthet Restor Dent. 2017;29(2):118-27. https://doi.org/10.1111/jerd.12275
» https://doi.org/10.1111/jerd.12275 -
23Sampaio CS, Chiu KJ, Farrokhmanesh E, Janal M, Puppin-Rontani RM, Giannini M et al. Microcomputed Tomography Evaluation of Polymerization Shrinkage of Class I Flowable Resin Composite Restorations. Oper Dent. 2017;42(1):E16-23. https://doi.org/10.2341/15-296-L
» https://doi.org/10.2341/15-296-L -
24Carrera CA, Lan C, Escobar-Sanabria D, Li Y, Rudney J, Aparicio C et al. The use of micro-CT with image segmentation to quantify leakage in dental restorations. Dent Mater. 2015;31(4):382-90. https://doi.org/10.1016/j.dental.2015.01.002
» https://doi.org/10.1016/j.dental.2015.01.002 -
25Van Ende A, De Munck J, Van Landuyt K, Van Meerbeek B. Effect of Bulk-filling on the Bonding Efficacy in Occlusal Class I Cavities. J Adhes Dent. 2016;18(2):119-24.
-
26Fronza BM, Rueggeberg FA, Braga RR, Mogilevych B, Soares LE, Martin AA et al. Monomer conversion, microhardness, internal marginal adaptation, and shrinkage stress of bulk-fill resin composites. Dent Mater. 2015;31(12):1542-51. https://doi.org/10.1016/j.dental.2015.10.001
» https://doi.org/10.1016/j.dental.2015.10.001 -
27Zeiger DN, Sun J, Schumacher GE, Lin-Gibson S. Evaluation of dental composite shrinkage and leakage in extracted teeth using X-ray microcomputed tomography. Dent Mater. 2009;25(10):1213-20. https://doi.org/10.1016/j.dental.2009.04.007
» https://doi.org/10.1016/j.dental.2009.04.007 -
28Braga RR, Ballester RY, Ferracane JL. Factors involved in the development of polymerization shrinkage stress in resin-composites: a systematic review. Dent Mater. 200521(10):962-70. https://doi.org/10.1016/j.dental.2005.04.018
» https://doi.org/10.1016/j.dental.2005.04.018 -
29Al Sunbul H, Silikas N, Watts DC. Polymerization shrinkage kinetics and shrinkage-stress in dental resin-composites. Dent Mater. 2016;32(8):998-1006. https://doi.org/10.1016/j.dental.2016.05.006
» https://doi.org/10.1016/j.dental.2016.05.006 -
30Benetti AR, Havndrup-Pedersen C, Honoré D, Pedersen MK, Pallesen U. Bulk-fill resin composites: polymerization contraction, depth of cure, and gap formation. Oper Dent. 2015;40(2):190-200. https://doi.org/10.2341/13-324-L
» https://doi.org/10.2341/13-324-L -
31Orłowski M, Tarczydło B, Chałas R. Evaluation of marginal integrity of four bulk-fill dental composite materials: in vitro study. Sci World J. 2015;2015:701262. https://doi.org/10.1155/2015/701262
» https://doi.org/10.1155/2015/701262 -
32Moorthy A, Hogg CH, Dowling AH, Grufferty BF, Benetti AR, Fleming GJ. Cuspal deflection and microleakage in premolar teeth restored with bulk-fill flowable resin-based composite base materials. J Dent. 2012;40(6):500-5. https://doi.org/10.1016/j.jdent.2012.02.015
» https://doi.org/10.1016/j.jdent.2012.02.015 -
33Flury S, Hayoz S, Peutzfeldt A, Hüsler J, Lussi A. Depth of cure of resin composites: is the ISO 4049 method suitable for bulk fill materials? Dent Mater. 2012;28(5):521-8. https://doi.org/10.1016/j.dental.2012.02.002
» https://doi.org/10.1016/j.dental.2012.02.002 -
34Bausch JR, de Lange K, Davidson CL, Peters A, de Gee AJ. Clinical significance of polymerization shrinkage of composite resins. J Prosthet Dent. 1982;48(1):59-67. https://doi.org/10.1016/0022-3913(82)90048-8PMID:6955507
» https://doi.org/10.1016/0022-3913(82)90048-8PMID:6955507 -
35Bowen RL. Adhesive bonding of various materials to hard tooth tissues. VI. Forces developing in direct-filling materials during hardening. J Am Dent Assoc. 1967;74(3):439-45. https://doi.org/10.14219/jada.archive.1967.0078
» https://doi.org/10.14219/jada.archive.1967.0078
Publication Dates
-
Publication in this collection
2017
History
-
Received
17 May 2017 -
Reviewed
09 Oct 2017 -
Accepted
06 Nov 2017