Abstract
AIM: To compare the dimensions of quality of life in the stages of chronic kidney disease and the influence of sociodemographic, clinical and laboratory data. INTRODUCTION: The information available on the quality of life of patients on conservative treatment and the relationship between the quality of life and glomerular filtration rate is limited. METHODS: 155 patients in stages 1-5 of chronic kidney disease and 36 in hemodialysis were studied. Quality of life was rated by the Medical Outcomes Study Short Form 36-Item (SF-36) and functional status by the Karnofsky Performance Scale. Clinical, laboratory and sociodemographic variables were investigated. RESULTS: Quality of life decreased in all stages of kidney disease. A reduction in physical functioning, physical role functioning and in the physical component summary was observed progressively in the different stages of kidney disease. Individuals with higher educational level who were professionally active displayed higher physical component summary values, whereas men and those with a higher income presented better mental component summary values. Older patients performed worse on the physical component summary and better on the mental component summary. Hemoglobin levels correlated with higher physical component summary values and the Karnofsky scale. Three or more comorbidities had an impact on the physical dimension. CONCLUSION: Quality of life is decreased in renal patients in the early stages of disease. No association was detected between the stages of the disease and the quality of life. It was possible to establish sociodemographic, clinical and laboratory risk factors for a worse quality of life in this population.
Predialysis; Hemodialysis; SF-36; Chronic kidney insufficiency; Mental health
CLINICAL SCIENCE
INephrology - Universidade Federal de São Paulo, São Paulo, SP/Brazil
IIPsiquiatria - Universidade Federal de São Paulo, São Paulo, SP/Brazil
ABSTRACT
AIM: To compare the dimensions of quality of life in the stages of chronic kidney disease and the influence of sociodemographic, clinical and laboratory data.
INTRODUCTION: The information available on the quality of life of patients on conservative treatment and the relationship between the quality of life and glomerular filtration rate is limited.
METHODS: 155 patients in stages 1-5 of chronic kidney disease and 36 in hemodialysis were studied. Quality of life was rated by the Medical Outcomes Study Short Form 36-Item (SF-36) and functional status by the Karnofsky Performance Scale. Clinical, laboratory and sociodemographic variables were investigated.
RESULTS: Quality of life decreased in all stages of kidney disease. A reduction in physical functioning, physical role functioning and in the physical component summary was observed progressively in the different stages of kidney disease. Individuals with higher educational level who were professionally active displayed higher physical component summary values, whereas men and those with a higher income presented better mental component summary values. Older patients performed worse on the physical component summary and better on the mental component summary. Hemoglobin levels correlated with higher physical component summary values and the Karnofsky scale. Three or more comorbidities had an impact on the physical dimension.
CONCLUSION: Quality of life is decreased in renal patients in the early stages of disease. No association was detected between the stages of the disease and the quality of life. It was possible to establish sociodemographic, clinical and laboratory risk factors for a worse quality of life in this population.
Keywords: Predialysis; Hemodialysis; SF-36; Chronic kidney insufficiency; Mental health.
INTRODUCTION
The incidence and prevalence of patients with chronic kidney disease (CKD) is increasing worldwide. In Brazil, the Brazilian Society of Nephrology has collected information annually on patients with end-stage renal disease (ESRD) since 1999 and made it available on the Society's website.1 In 2008, the estimated number of patients in dialysis amounted to 87,044, of whom 90% were on hemodialysis and 10% on peritoneal dialysis.
Some studies have evaluated the quality of life (QOL) of patients undergoing dialysis, but there is limited information available on the QOL of patients on conservative treatment of CKD and the relationship between QOL and the early stages of the disease. The QOL of these patients seems to be poorer than that of the general population, but better than for patients on dialysis.2,3 Certain factors such as anemia, associated diseases and early treatment by a nephrologist appear to have an impact on the QOL of these patients.3-5
The objectives of this cross-sectional study were to assess the QOL of patients with stages 1-5 CKD on conservative treatment in order to identify a possible association between QOL and progression of kidney insufficiency. The results were compared with those obtained for patients on hemodialysis. Sociodemographics, clinical and laboratory data were also evaluated.
METHODS AND MATERIALS
A total of 202 patients were randomly selected, including 165 with non-dialytic CKD followed up at the CKD outpatient clinic of the Division of Nephrology, Federal University of São Paulo, São Paulo, Brazil, and 37 patients undergoing hemodialysis at the institution. A sample of 30% of all patients under follow-up was selected using a systematic random sampling method. Initially, a list of all patients with CKD (and another for those on hemodialysis) was made, and a consecutive number was given to each one. Then, a starting point was chosen at random and every fifth record (this interval was prespecified) on the list was selected. The procedure was repeated until the estimated number of participants was reached. Among the patients initially contacted, 11 refused to participate in the study.
The subjects were interviewed prior to the medical visits or after the hemodialysis session in a separate room by two trained interviewers. Included patients should be on hemodialysis treatment for >6 months and <6 years and were submitted to a conventional in-center hemodialysis regimen consisting of three weekly hemodialysis sessions lasting 4 hours each. Patients were excluded if they did not consent to participate, were younger than 18 years or had hearing, speech or cognitive deficits that would impair understanding of the questions.
The protocol was approved by the ethics committee of the institution, and all subjects gave written informed consent to participate in the study.
To assess the QOL, we used the Medical Outcomes Study Short Form 36-Item Health Survey (SF-36), a generic instrument translated and validated in Brazilian patients with ESRD.6,7 This instrument is divided into 8 dimensions: physical functioning, physical role functioning, pain, general health, vitality, social role functioning, emotional role functioning, mental health. The results of each scale vary from 0 to 100 (worse to best possible status). The physical and mental components of the 8 scales were combined into a physical component summary (PCS) and a mental component summary (MCS). The 2 summary measures were standardized so as to have a mean value of 50 and a standard deviation (SD) of 10 in the general population.7
The Karnofsky Performance Status (KPS)8 was used to assess self-sufficiency and functional capacity, which determines functional impairment in the performance of activities of daily living, using a score ranging from 100 (indicating no evident disease) to 0 (indicating death). This instrument has been widely used in studies on patients with CKD.
The socioeconomic level of the patients was evaluated according to the criteria of the Brazilian Association of Research Companies, which are recognized in Brazil and divide the population into social classes A, B, C, D and E, with class A corresponding to the highest socioeconomic level.9 Other sociodemographic and clinical variables were also analyzed in an attempt to identify a possible association with QOL.
Glomerular filtration rate (GFR) was estimated by the creatinine clearance according to the formula of Cockcroft and Gault10 adjusted to 1.73 m2 of body surface area, using the latest serum creatinine measurement available for each patient. The stages of CKD were classified as suggested by the Kidney Disease Outcomes Quality Initiative11 and are presented in Table 1.
For the purpose of analysis, CKD stages 1 and 2 and stages 4 and 5 were combined, because of the small number of patients in each group, to increase the power of statistical comparisons between groups.
Statistical analysis
The results are presented as percentage or mean±SD. Chi-square tests were performed to compare categorical variables. For the continuous variables, we used Student's unpaired t-test to compare two groups, and ANOVA to compare more than two groups. Whenever the ANOVA test result was significant, we then compared the groups two by two. Pearson's correlation test was employed to correlate the PCS and the MCS and KPS results with the other continuous variables. Statistical significance was set at p<0.05, and all tests performed were two-tailed.
RESULTS
Of the 191 patients who participated in the study, 155 were predialysis CKD patients and 36 were on HD. The total sample of predialysis CKD patients was divided into five stages according to GFR and subsequently grouped into three groups (stages 1+2, 3 and 4+5).
The patients in the three groups of CKD stage and those on hemodialysis were similar with regard to their socio-demographic characteristics (Table 2).
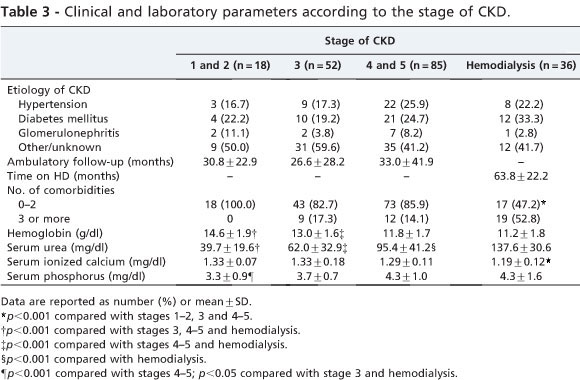
With respect to laboratory variables, the groups differed in some characteristics, as shown in Table 3.
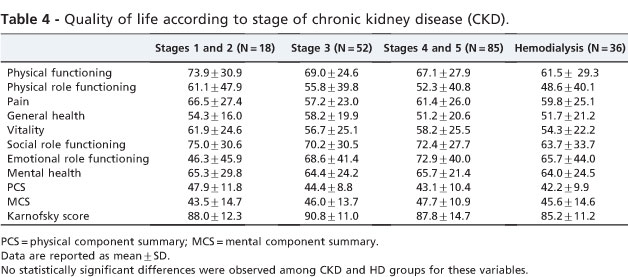
QOL, as evaluated by the means of SF-36 domains, was low for most dimensions in all stages and was not statistically significant different among the patients in the three groups of CKD stage or on hemodialysis. The dimensions showing lower values in stages 1 and 2 were emotional role functioning and general health; in stage 3, physical role functioning and vitality; and in stages 4 and 5 and hemodialysis, physical role functioning and general health. No difference was observed among the groups regarding the PCS, the MCS or on the KPS (Table 4).
Evaluating sociodemographic data, patients who had a higher educational level performed better than the others in mean PCS. As for the patients' mean MCS scores, males and Asians showed better results and those with no individual monthly income had lower values than those with some income. The KPS scores showed no statistically significant differences related to demographic data, except for occupation: those who were professionally active performed better (Table 5). No significantly difference was found between the mean PCS and MCS and the KPS scores when the patients were divided by the etiology of CKD and the occurrence of hospitalization.
With regard to age, there was a negative correlation with the mean PCS and a positive correlation with the mean MCS scores. Hemoglobin level was positively correlated with PCS and KPS, whereas the serum phosphorus levels showed a negative correlation with MCS (Table 6).
Evaluating patients for the number of comorbidities, we found that those with three or more were older, retired and diabetic. Low levels of calcium and high levels of urea were also found in patients with more comorbidities. With respect to the QOL, patients with more comorbidities had worse rates in the assessment of functional capacity (assessed by both SF-36 and the KPS), physical role functioning and PCS.
DISCUSSION
Our results indicate low QOL scores in the early stages of CKD, although we have not demonstrated a significant decrease in QOL progressively in the different stages of renal disease. Not only were mean values of the physical components reduced as early as stages 1-3 of CKD but mental health also seemed to be compromised, based on the mean values of the SF-36 scores, which were below 70 in most dimensions. Normal healthy populations usually have scores above this level in most studies7.
Few studies have evaluated the QOL of patients in the early stages of CKD, especially in the first two stages, or sought to relate QOL and GFR.3,12 In these studies, a significant reduction in QOL was also not identified according to the progression of renal dysfunction. What is reported more frequently in the literature is a decrease in the physical domains of QOL in the advanced stages of CKD, which was also identified in our study.13-16
In our study, the hemoglobin levels showed a correlation with better PCS and KPS scores. In the literature, the impact of anemia on QOL in CKD is well described from the predialysis CKD phases through ESRD.17,18 We observed that a greater number of comorbidities were associated with older age, diabetes and unemployment or retired status. The presence of three or more comorbidities had a negative impact on the domains physical functioning, physical role functioning and PCS, and on KPS. Some reports have suggested that the presence of comorbidities is a major determinant of a decline in QOL.19,20 Diabetes mellitus has also been associated with low QOL.21
It is known, however, that the subjective assessment of QOL is multifactorial, and therefore the progression of renal dysfunction may not be the only determinant in its deterioration. In our study, more sociodemographic factors (age, ethnicity, gender, professional activity, education, income) were associated with decreased QOL than physical factors. Added to this, it is possible that subjective factors such as adaptation to disease and treatment, satisfaction with the medical staff and social support, among others, may interfere directly in the assessment of QOL, but were not evaluated in this study. The influence of these different factors on the assessment of QOL may explain the difficulty in establishing a linear relation with the GFR.
Some limitations of the present study are the relatively small sample size to detect significant differences between the stages of CKD and the difficulties we encountered in recruiting subjects in the initial stages of the disease. The cross-sectional design of the study only permitted us to determine associations between variables and not causal relationships. Thus, longitudinal studies that take into account qualitative assessments should be conducted to seek a better understanding of the influence of the progression of CKD on QOL.
In conclusion, in this study, we observed a negative impact on the QOL of patients in the early stages of CKD, although we were not able to detect a significant association between the stages of the disease and the SF-36 domains. However, it was possible to establish sociodemographic, clinical and laboratory risk factors for a worse QOL in this population (educational level, gender, individual income, professional activity, age, hemoglobin levels, serum phosphorus levels, diabetes and comorbidities). Although several of the variables that were associated with alterations in the QOL cannot be changed (e.g., age, gender, ethnicity), efforts should be made to decrease the effects of those factors that can be changed, such as improving the hemoglobin levels and adequately managing the comorbid-ities. The health professionals responsible for the care provided to this population should ideally be familiar with and trained in the application of the QOL assessment tools, which may be valuable in the global assistance of these patients, even in the earlier stages of disease, and allow timely health care interventions in the course of the disease.
ACKNOWLEDGMENTS
This study was supported by grants from CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior).
Received for publication on December 24, 2010; First review completed on January 17, 2011; Accepted for publication on March 2, 2011
E-mail: rsesso@unifesp.br Tel.: 55 11 59041699
-
1www.sbn.org.br (accessed July 2009).
» link - 2. Kalender B, Ozdemir AC, Dervisoglu E, Ozdemir O. Quality of life in chronic kidney disease: effects of treatment modality, depression, malnutrition and inflammation. Int J Clin Pract. 2007;61:569-76, doi: 10. 1111/j.1742-1241.2006.01251.x.
- 3. Perlman RL, Finkelstein FO, Liu L, Roys E, Kiser M, Eisele G, et al. Quality of life in chronic kidney disease (CKD): a cross-sectional analysis in the Renal Research Institute CKD study. Am J Kidney Dis. 2005;45:658-66, doi: 10.1053/j.ajkd.2004.12.021.
- 4. Harris LE, Luft FC, Rudy DW, Tierney WM. Clinical correlates of functional status inpatients withchronic renal insufficiency. Am JKidney Dis. 1993;21:161-6.
- 5. Sesso R, Yoshihiro MM. Time of diagnosis of chronic renal failure and assessment of quality of life in hemodialysis patients. Nephrol Dial Transplant. 1997;12:2111-16, doi: 10.1093/ndt/12.10.2111.
- 6. Neto JF, Ferraz MB, Cendoroglo M, Draibe S, Yu L, Sesso R. Quality of life at the initiation of maintenance dialysis treatment-- a comparison between the SF-36 and the KDQ questionnaires. Qual Life Res. 2000;9:101-7, doi: 10.1023/A:1008918609281.
- 7. Ware JE, Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473-83, doi: 10.1097/00005650-199206000-00002.
- 8. Karnofsky DA, Burchenal JH. The clinical evaluation of chemotherapeutic agents in cancer. In: Macleod CM, editor. Evaluation of Chemotherapeutic Agents. New York: Columbia University Press; 1949. pp. 191-205.
-
9Associação Brasileira de Empresas de Pesquisa (ABEPE). Critério de Classificação Econômica Brasil. 2003. Available at www.abep.org
- 10. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16:31-41, doi: 10.1159/000180580.
- 11. K/DOQI clinical practice guidelines for chronic kidney disease. Kidney Outcomes Quality Initiative. Am J Kidney Dis. 2002;39 (suppl 2): S1-S266.
- 12. Condé SA, Fernandes N, Santos FR, Chouab A, Mota MM, Bastos MG. Cognitive decline, depression and quality of life in patients at different stages of chronic kidney disease. J Bras Nefrol. 2010;32:242-8.
- 13. DeOreo PB. Hemodialysis patient-assessed functional health status predicts continued survival, hospitalization, and dialysis-attendance compliance. Am J Kidney Dis. 1997;30:204-12, doi: 10.1016/S0272-6386(97)90053-6.
- 14. Spiegel BM, Melmed G, Robbins S, Esrailian E. Biomarkers and health-related quality of life in end-stage renal disease: a systematic review. Clin J Am Soc Nephrol. 2008;3:1759-68, doi: 10.2215/CJN.00820208.
- 15. Fukuhara S, Yamazaki S, Marumo F, Akiba T, Akizawa T, Fujimi S, et al. Health-related quality of life of predialysis patients with chronic renal failure. Nephron Clin Pract. 2007;105:c1-8, doi: 10.1159/000096802.
- 16. Molsted S, Prescott L, Heaf J, Eidemak I. Assessment and clinical aspects of health-related quality of life in dialysis patients and patients with chronic kidney disease. Nephron Clin Pract. 2007;106:c24-33, doi: 10. 1159/000101481.
- 17. Moreno F, Lopez Gomez JM, Sanz-Guajardo D, Jofre R, Valderrabano F. Quality of life in dialysis patients. A Spanish multicentre study. Spanish Cooperative Renal Patients Quality of Life Study Group. Nephrol Dial Transplant. 1996;11(suppl. 2):125-9.
- 18. Finkelstein FO, Story K, Firanek C, Mendelssohn D, Barre P, Takano T, et al. Health-related quality of life and hemoglobin levels in chronic kidney disease patients. Clin J Am Soc Nephrol. 2009;4:33-8, doi: 10. 2215/CJN.00630208.
- 19. Mingardi G, Cornalba L, Cortinovis E, Ruggiata R, Mosconi P, Apolone G. Health-related quality of life in dialysis patients. A report from an Italian study using the SF-36 Health Survey. DIA-QOL Group. Nephrol Dial Transplant. 1999;14:1503-10, doi: 10.1093/ndt/14.6.1503.
- 20. Merkus MP, Jager KJ, Dekker FW, de Haan RJ, Boeschoten EW, Krediet RT. Physical symptoms and quality of life in patients on chronic dialysis: results of The Netherlands Cooperative Study on Adequacy of Dialysis (NECOSAD). Nephrol Dial Transplant. 1999;14:1163-70, doi: 10.1093/ ndt/14.5.1163.
- 21. Baiardi F, Degli Esposti E, Cocchi R, Fabbri A, Sturani A, Valpiani G, et al. Effects of clinical and individual variables on quality of life in chronic renal failure patients. J Nephrol. 2002;15:61-7.
Quality of life in patients with chronic kidney disease
Publication Dates
-
Publication in this collection
21 July 2011 -
Date of issue
2011
History
-
Accepted
02 Mar 2011 -
Reviewed
17 Jan 2011 -
Received
24 Dec 2010