Abstract
OBJECTIVE:
To determine the range of motion and stability of the human cadaveric cervical spine after the implantation of a novel artificial disc and vertebra system by comparing an intact group and a fusion group.
METHODS:
Biomechanical tests were conducted on 18 human cadaveric cervical specimens. The range of motion and the stability index range of motion were measured to study the function and stability of the artificial disc and vertebra system of the intact group compared with the fusion group.
RESULTS:
In all cases, the artificial disc and vertebra system maintained intervertebral motion and reestablished vertebral height at the operative level. After its implantation, there was no significant difference in the range of motion (ROM) of C3-7 in all directions in the non-fusion group compared with the intact group (p>0.05), but significant differences were detected in flexion, extension and axial rotation compared with the fusion group (p<0.05). The ROM of adjacent segments (C3-4, C6-7) of the non-fusion group decreased significantly in some directions compared with the fusion group (p<0.05). Significant differences in the C4-6 ROM in some directions were detected between the non-fusion group and the intact group. In the fusion group, the C4-6 ROM in all directions decreased significantly compared with the intact and non-fusion groups (p<0.01). The stability index ROM (SI-ROM) of some directions was negative in the non-fusion group, and a significant difference in SI-ROM was only found in the C4-6 segment of the non-fusion group compared with the fusion group.
CONCLUSION:
An artificial disc and vertebra system could restore vertebral height and preserve the dynamic function of the surgical area and could theoretically reduce the risk of adjacent segment degeneration compared with the anterior fusion procedure. However, our results should be considered with caution because of the low power of the study. The use of a larger sample should be considered in future studies.
Biomechanics; Cervical vertebral corpectomy and fusion; Adjacent segment disease; Artificial disc and vertebra system; Range of motion; Stability index range of motion
INTRODUCTION
Anterior cervical fusion has been used as an effective therapy for cervical spine
diseases (11. Emery SE, Bolesta MJ, Banks MA, Jones PK. Robinson anterior
cervical fusion comparison of the standard and modified techniques. Spine (Phila
Pa 1976). 1994;19(6):660-3, 10.1097/00007632-199403001-00004
http://dx.doi.org/10.1097/00007632-19940...
,22. McGuire RA, St John K. Comparison of anterior cervical fusions
using autogenous bone graft obtained from the cervical vertebrae to the modified
Smith-Robinson technique. J Spinal Disord. 1994;7(6):499-503.). However, increasing attention is being paid to the incidence of
adjacent segment disease (ASD) after successful fusion (33. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH.
Radiculopathy and myelopathy at segments adjacent to the site of a previous
anterior cervical arthrodesis. Journal of Bone and Joint Surgery-American
Volume. 1999;81A(4):519-28.). The lost motion at the fusion level redistributes into the
adjacent segments, increasing the pressure in facet joints and adjacent discs and
thus leading to ASD (33. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH.
Radiculopathy and myelopathy at segments adjacent to the site of a previous
anterior cervical arthrodesis. Journal of Bone and Joint Surgery-American
Volume. 1999;81A(4):519-28.–55. Colle KO, Butler JB, Reyes PM, Newcomb AG, Theodore N, Crawford
NR. Biomechanical evaluation of a metal-on-metal cervical intervertebral disc
prosthesis. Spine J. 2013;13(11):1640-9,
10.1016/j.spinee.2013.06.026
http://dx.doi.org/10.1016/j.spinee.2013....
). Previous studies of cervical artificial
discs (CADs) have shown the success of that method (66. Wigfield CC, Gill SS, Nelson RJ, Metcalf NH, Robertson JT. The
new Frenchay artificial cervical joint - Results from a two-year pilot study.
Spine. 2002;27(22):2446-52, 10.1097/00007632-200211150-00006
http://dx.doi.org/10.1097/00007632-20021...
); in contrast, when anterior cervical corpectomy and fusion (ACCF) is
used to treat cervical spinal diseases such as spondylitis, burst fracture,
vertebral tumor, and vertebral tuberculosis (77. Bilbao G, Duart M, Aurrecoechea JJ, Pomposo I, Igartua A, Catalan
G, et al. Surgical results and complications in a series of 71 consecutive
cervical spondylotic corpectomies. Acta Neurochir (Wien).
2010;152(7):1155-63.–99. Nuckley DJ, Konodi MA, Raynak GC, Ching RP, Chapman JR, Mirza SK.
Neural space integrity of the lower cervical spine: Effect of anterior lesions.
Spine. 2004;29(6):642-9, 10.1097/01.BRS.0000115132.49734.33
http://dx.doi.org/10.1097/01.BRS.0000115...
), it destroys both the
disc and the vertebra. Most clinical experience with CAD focuses on the
intervertebral disc, not the vertebra, and CAD use cannot replace ACCF.
Consequently, it is necessary to develop a prosthesis that can both preserve
intervertebral motion and reconstruct the vertebral height.
We have designed a novel artificial disc and vertebra system (ADVS) that replaces both the disc and the vertebra in a functional spinal unit (FSU). This system can maintain both cervical motion and vertebral height after it is implanted into the anterior defect at the C5 level. In this study, we performed biomechanical experiments to examine the ADVS’s function and stability by comparing it with an intact group and a vertebral fusion group.
MATERIALS AND METHODS
Design of the ADVS
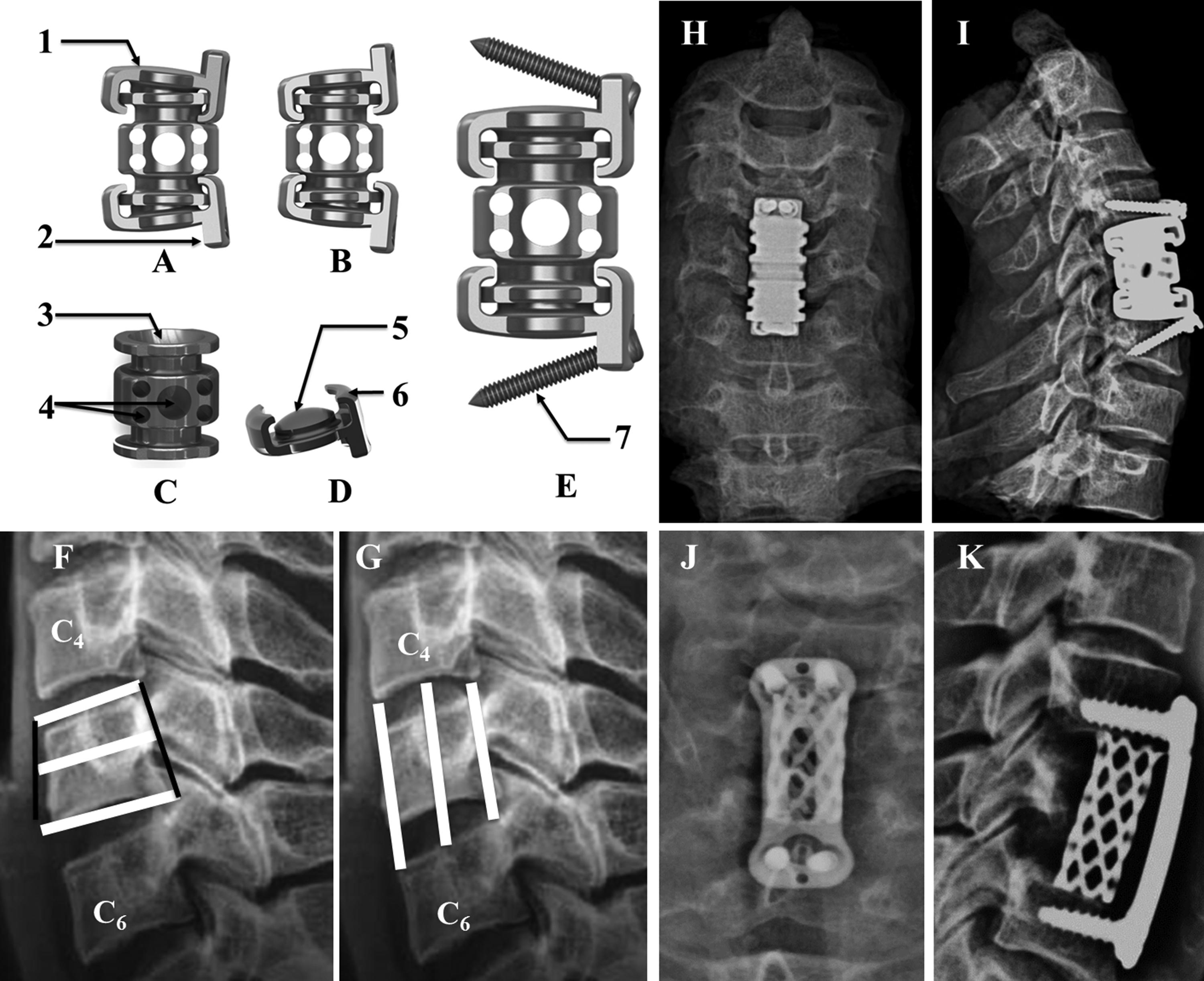
The ADVS prosthesis (China patent number: 201410072192.7) was designed to mimic the physiological motion of the cervical spine (Bright Laser Rapid Prototyping Technology Co., Ltd, Xiʹan, China.). It was made from a titanium alloy (Ti6Al4V) and comprised three major compartments: the upper & lower artificial cervical discs and the middle artificial vertebra (Figure 1). Each disc featured a base and a front wing with a 90° angle between them. The base included an articular head and a spherical surface 8 mm in diameter and 4 mm in depth at the bottom. The front wing featured two cancellous bone screw holes one on each side. There was a unique “L” structure on each side of the disc’s base that was designed to prevent the dislocation of the disc and the vertebra. The artificial vertebra had an articular fossa 8 mm in diameter and 4 mm in depth on its upper & lower sides. Several tubes of different diameters were designed for bone grafts and were included on the lateral side of the vertebra. There was a hemispherical socket joint between the disc and the vertebra that theoretically allowed a 12° range of motion (ROM) in flexion, extension and lateral bending and a 360° ROM in rotation. Rotation of the upper & lower components was achieved by allowing the hemisphere of the joint to glide in the socket with metal-on-metal articulating surfaces. The prosthesis was assembled in vitro. The disc was first fixed on the vertebra and then rotated 90° until the wing was facing anteriorly. The ADVS was fixed onto the upper and lower vertebrae using four self-drilling trapping screws. The cancellous screws were 3 mm in diameter and 16 mm to 20 mm in length.
The ADVS is made of a titanium alloy (Ti6Al4V), which has three major parts, two discs and a vertebra. There is a hemisphere socket joint between the disc and vertebra that theoretically allow 12° in flexion, extension and lateral bending, 360° in axial rotation. A) ADVS in flexion; B) ADVS in extension; C) the artificial vertebra part; D) the artificial disc part; E) the lateral view of ADVS. 1) the base part of disc, it has a smooth surface on the top that fits the adjacent vertebra; 2) the front wing part; 3) the articular fossa; 4) bone graft tubes in different diameter; 5) the articular head; 6) the “L” structure, which was designed for dislocation between the disc part and the vertebra part; 7) the self-drilling trapping screw; F) upper, middle and lower sagittal diameters of C5 vertebra; G) anterior, media and posterior height from C4∼5 disc to C5∼6 disc. The ADVS was implanted after corpectomy was performed at C5 level, X-ray films of posteroanterior view H) and lateral I) views. The anterior plate fusion performed after cervical discectomy and vertebral corpectomy of C5 level, X-ray films of posteroanterior view J) and lateral K) views.
Specimens
All of the specimens were obtained via informed donation from cadaveric materials in accordance with federal and state regulations. The specimens comprised 18 sets of cervical spines with multiple levels (C2-T1; average donor age: 42.4±2.4 years; 11 male, 7 female) from the Anatomy and Pathology Department of the Medical College of Xiʹan Jiaotong University. Subjective examinations confirmed the absence of skeletal abnormalities. Digital X-ray films (QDR-2000; Hologic, Waltham, MA.) were obtained to ensure that none of the specimens had osteoporosis. In our previous study, we obtained measurements of human cervical spines from 50 volunteers. The obtained parameters are shown in Figure 1. All of the specimens were stored at -20° C in double-sealed plastic bags until preparation. The muscle tissue was removed, but all ligaments and bony structures were preserved.
Biomechanical Tests
Biomechanical Model
The 18 specimens were tested as normal cervical spines (intact group), and their ROM was recorded. All of the specimens were then randomly assigned to one of 2 groups, a fusion group and a non-fusion group (ADVS implantation at C5), with 9 specimens in each group. Before testing, the specimens were thawed, and the muscle tissue was carefully removed; all ligaments, bony structures and discs were preserved. Corpectomy was performed at the C5 level using a high-speed spherical drill bit, and discectomy was performed at C4-5 and C5-6 using nucleus pulposus forceps and curettes (Figure 1). In the fusion group, a plate was fixed anteriorly from C4 to C6. To allow comparisons with the fusion group, the artificial prosthesis was implanted at the C5 level in the non-fusion group. After the screw length was measured, two superior and two inferior self-drilled trapping cancellous bone screws (3.0 mm in diameter) were fixed superoposteriorly and inferoposteriorly, respectively. The screws were inserted at a 20° angle in the cranial and caudal directions, respectively (Figure 1).
Three-Dimensional Flexibility Test
An MTS rotating machine (MTS-858/2.5, MTS System Inc., Minneapolis, MN, USA)
was used for the biomechanical tests. The C3-T1
vertebrae of the test model were embedded in a special metal mould
containing polymethylmethacrylate to keep the specimens in a set position
with the C3 vertebra parallel to the horizontal plane. To
determine the stability of the specimens, a multidirectional flexibility
test was used. Our research was concerned with developing a kinematic model
to establish the axes of rotation and the mutual positioning of the
vertebrae with regard to flexion, extension, lateral bending and axial
rotation in 4 equal steps to a maximum of 2.0 N·m (1010. Snijders CJ, Vandijke GAH, Roosch ER. A biomechanical model for
the analysis of the cervical-spine in static postures. J Biomech.
1991;24(9):783-92, 10.1016/0021-9290(91)90303-5
http://dx.doi.org/10.1016/0021-9290(91)9...
,1111. Zhang J, He XJ, Li HP, Wang D, Zhao WD, Xu JH, et al.
Biomechanical study of anterior cervical corpectomy and step-cut grafting with
bioabsorbable screws fixation in cadaveric cervical spine model. Spine.
2006;31(19):2195-201, 10.1097/01.brs.0000232798.97075.73
http://dx.doi.org/10.1097/01.brs.0000232...
). The ROM of the C3-7, C3-4,
C4-6 and C6-7 segments was recorded; then, the
traction arm of the MTS testing machine was stretched at a speed of 5 mm/s.
A laser 3D scanning system (RealScan USB Scanner 200, 3-dimensional; Digital
Corp., Danbury, CT) was used to record the under-zero load and to obtain
maximum-load motion images of the cervical spine. Markers were attached to
different segments of the specimen and were not in contact with each other
to ensure that they could be readily distinguished. The digitized positions
of the markers along the spine under different loading conditions were
recorded, and the data were stored in the computer. The system then analyzed
and converted the image data using the corresponding software system.
Special care was taken throughout the tests to keep the specimens moist
using a saline solution.
Stability Index Flexibility Test
Zhang et al. (1111. Zhang J, He XJ, Li HP, Wang D, Zhao WD, Xu JH, et al.
Biomechanical study of anterior cervical corpectomy and step-cut grafting with
bioabsorbable screws fixation in cadaveric cervical spine model. Spine.
2006;31(19):2195-201, 10.1097/01.brs.0000232798.97075.73
http://dx.doi.org/10.1097/01.brs.0000232...
) introduced the
stability index ROM (SI-ROM) to quantify the stability that instrumentation
provided to the spine. The SI-ROM was defined using the following equations:
SI-ROM=(ROMintact-ROMinstrumented)/ROMintact.
An SI-ROM value of zero indicates that the spinal contruct is as stable as
the intact spine, while a positive or negative value indicates that the
spinal construct is more stable or less stable, respectively, than the
intact spine.
Statistical Analysis
The data were analyzed using SPSS software (version 19.0; SPSS Inc., Chicago, IL, USA). The results were presented as the mean±SD. GraphPad Prism 5.01 (GraphPad Software, Inc.) was used to create the histogram. The ROM and SI-ROM data were analyzed using two-tailed Student’s t-tests. P-values less than 0.05 were considered statistically significant.
Ethics
This study followed the ethics guidelines of the Medical College of Xian Jiaotong University. All of the co-authors participated sufficiently in the work to assume public responsibility for appropriate portions of the content.
RESULTS
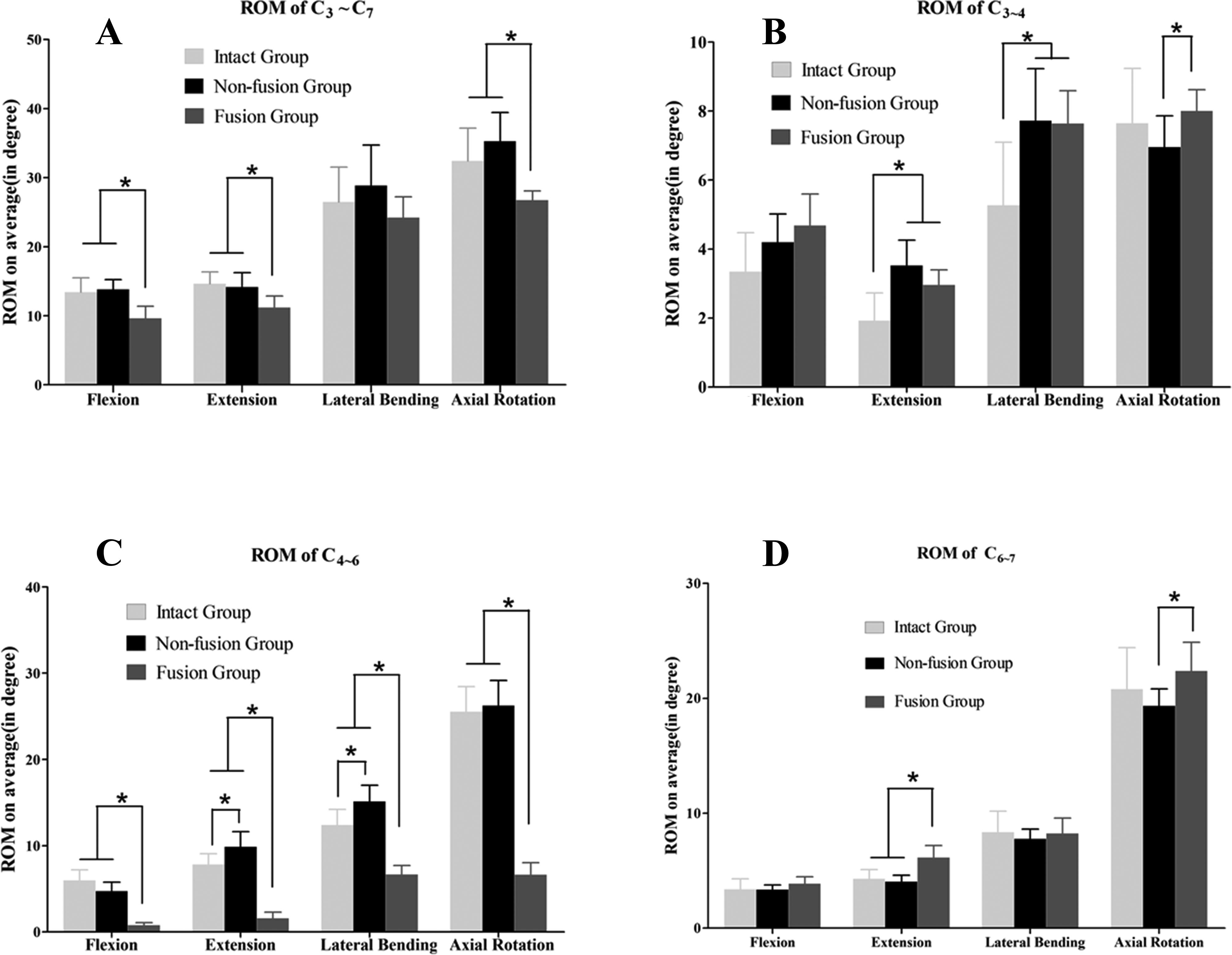
The height and sagittal diameter of the C5 vertebra and the C4-5 and C5-6 disc height were measured (Figure 1); the results are shown in Table 1. In all cases, the ADVS maintained intervertebral motion at the operative levels while reestablishing vertebral height. Figure 2 and Table 2 show the ROM of different segments of the cervical spine. Compared with the intact group, the non-fusion group showed no significant difference in the ROM of the C3-7 segment in any direction (p>0.05), and the fusion group showed significantly decreased flexion, extension and axial rotation (p<0.05; Figure 2A). The ROM of the C3-4 segment in the non-fusion and fusion groups increased significantly in extension and lateral bending compared with that of the intact group (p<0.05). Moreover, the ROM for axial rotation at the C3-4 segment differed significantly between the non-fusion and fusion groups (p<0.05; Figure 2B). The C4-6 segment ROM was compared among the groups. In the fusion group, the ROM of the C4-6 segment decreased significantly in all directions compared with that of the intact and non-fusion groups (p<0.001), and significant differences in extension and lateral bending were detected between the intact and fusion groups (Figure 2C). No significant differences in the ROM of the C6-7 segment were observed between the intact and non-fusion groups. In addition, the extension and axial rotation of this segment differed significantly between the non-fusion and fusion groups, and the ROM in extension differed significantly between the fusion and intact groups (Figure 2D). Table 3 shows the SI-ROM of the non-fusion and fusion groups. At the C3-7 segment, the SI-ROM of the non-fusion group was positive in flexion and extension and negative in lateral bending and axial rotation; in contrast, the SI-ROM of the fusion group was positive in all directions. No difference was detected between the two groups at this segment. At the C3-4 segment, the SI-ROM of the non-fusion group was positive in axial rotation and negative in the other three directions; the SI-ROM of the fusion group was negative in all directions. At the C4-6 segment, the SI-ROM of the non-fusion group was negative in all directions except in axial rotation, and the SI-ROM of the fusion group was positive in all directions and was significantly increased compared with the non-fusion group (p<0.05). At the C6-7 segment, the SI-ROM of the non-fusion group was negative in flexion and positive in the other three directions, and the SI-ROM of the fusion group was negative in all directions. There was a significant difference in extension between the two groups at this segment.
ROM of C3∼C7, C3∼4, C4∼6, C6∼7. The ROM were measured under 2 N·m torque loading pressure. A) the fusion group showed a significantly restricted ROM of C3∼C7 regarding flexion, extension and axial rotation ROM of C3∼C7 compared to the intact group and non-fusion group. No significant difference of ROM in any direction was detected when compared the intact group and non-fusion group. B) the fusion group and non-fusion group showed a significantly increased ROM of C3∼4 regarding extension and lateral bending ROM of C3∼4 compared to the intact group. Significant difference of ROM of C3∼4 in axial rotation was detected when compared the intact group and non-fusion group. C) the fusion group showed a significantly restricted ROM of C4∼6 in all directions compared to the intact group and non-fusion group. Comparing with the intact group, the extension and lateral bending ROM of C4∼6 in non-fusion group increased significantly. D) the fusion group showed a significantly restricted ROM of C6∼7 in extension compared to the intact group and non-fusion group. The axial rotation ROM of C6∼7 in non-fusion group decreased significantly comparing with the fusion group. No significant difference of ROM of C6∼7 in any direction was detected when compared the intact group and non-fusion group. *p<0.05
DISCUSSION
Anterior cervical fusion has been widely used to treat cervical disc and vertebral
diseases (11. Emery SE, Bolesta MJ, Banks MA, Jones PK. Robinson anterior
cervical fusion comparison of the standard and modified techniques. Spine (Phila
Pa 1976). 1994;19(6):660-3, 10.1097/00007632-199403001-00004
http://dx.doi.org/10.1097/00007632-19940...
,22. McGuire RA, St John K. Comparison of anterior cervical fusions
using autogenous bone graft obtained from the cervical vertebrae to the modified
Smith-Robinson technique. J Spinal Disord. 1994;7(6):499-503.). The procedure fuses two or more cervical vertebrae and removes the
disc; consequently, the dynamic function of the fusion segment is changed
considerably, which can lead to long-term complications (33. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH.
Radiculopathy and myelopathy at segments adjacent to the site of a previous
anterior cervical arthrodesis. Journal of Bone and Joint Surgery-American
Volume. 1999;81A(4):519-28.). For example, the loss of motion is believd to result in
high pressure in adjacent discs and facet joints, and ASD has been detected after
long-term follow-up (55. Colle KO, Butler JB, Reyes PM, Newcomb AG, Theodore N, Crawford
NR. Biomechanical evaluation of a metal-on-metal cervical intervertebral disc
prosthesis. Spine J. 2013;13(11):1640-9,
10.1016/j.spinee.2013.06.026
http://dx.doi.org/10.1016/j.spinee.2013....
,1212. Cason GW, Herkowitz HN. Cervical intervertebral disc
replacement. J Bone Joint Surg Am. 2013;95(3):279-85,
10.2106/JBJS.J.01042
http://dx.doi.org/10.2106/JBJS.J.01042...
). In recent years, CAD use has been proposed to replace the
degenerated disc to preserve the dynamic function of the intervertebral space.
Several CAD methods have yielded superior results compared with anterior cervical
discectomy and fusion (ACDF) in the treatment of cervical disease (66. Wigfield CC, Gill SS, Nelson RJ, Metcalf NH, Robertson JT. The
new Frenchay artificial cervical joint - Results from a two-year pilot study.
Spine. 2002;27(22):2446-52, 10.1097/00007632-200211150-00006
http://dx.doi.org/10.1097/00007632-20021...
,) (1212. Cason GW, Herkowitz HN. Cervical intervertebral disc
replacement. J Bone Joint Surg Am. 2013;95(3):279-85,
10.2106/JBJS.J.01042
http://dx.doi.org/10.2106/JBJS.J.01042...
). However, in some methods, vertebral resection leads to the loss of
intervertebral motion and vertebral height. Both problems can result from ACCF, and
CAD use cannot reestablish vertebral height. Thus, the development of a prosthesis
that could preserve intervertebral motion and reconstruct the vertebral height is
necessary.
To maintain the dynamic function of the intervertebral space and reconstruct the
vertebral height, we designed an artificial cervical vertebra and intervertebral
complex (ACVC), and in 2012, we established a goat model to analyze the biomechanics
of the prosthesis (1616. Qin J, He X, Wang D, Qi P, Guo L, Huang S, et al. Artificial
cervical vertebra and intervertebral complex replacement through the anterior
approach in animal model: a biomechanical and in vivo evaluation of a successful
goat model. PLoS One. 2012;7(12):e52910,
10.1371/journal.pone.0052910
http://dx.doi.org/10.1371/journal.pone.0...
). Recently, other
motion-preserved prostheses have been developed (1717. Wu ZX, Han BJ, Zhao X, Kong L, Liu D, Cui G, et al.
Biomechanical evaluation of a novel total cervical prosth9. Nuckley DJ, Konodi
MA, Raynak GC, Ching RP, Chapman JR, Mirza SK. Neural space integrity of the
lower cervical spine: Effect of anterior lesions. Spine. 2004;29(6):642-9,
10.1097/01.BRS.0000115132.49734.33
http://dx.doi.org/10.1097/01.BRS.0000115...
,1818. Snijders CJ, Vandijke GAH, Roosch ER. A biomechanical model for
the analysis of the cervical-spine in static postures. J Biomech.
1991;24(9):783-92, 10.1016/0021-9290(91)90303-5
http://dx.doi.org/10.1016/0021-9290(91)9...
). However, the
ball-in-trough articulation of these prostheses was the high-friction surface, and
the centers of rotation of these prostheses were not in the intervertebral space.
Thus, we designed a new ADVS that contained three parts: two discs and a vertebra.
This new system had a larger articular surface between the disc and vertebra that
confined the motion within the intervertebral space. Moreover, it had a unique
L-shaped structure (Figure 1) to prevent
dislocation of the two parts. The assembly processes of the system were also unique;
the disc and vertebra parts were fixed at a 90° angle, and the disc part was
then rotated until the wing faced anteriorly. This device allowed a 12° range
of motion in flexion, extension and lateral bending and a 360° range of motion
in axial rotation. Based on a cervical prosthesis classification system presented by
the Cervical Spine Study Group, most cervical implants comprise metallic or
polymeric components or both (1919. Zhang J, He XJ, Li HP, Wang D, Zhao WD, Xu JH, et al.
Biomechanical study of anterior cervical corpectomy and step-cut grafting with
bioabsorbable screws fixation in cadaveric cervical spine model. Spine.
2006;31(19):2195-201, 10.1097/01.brs.0000232798.97075.73
http://dx.doi.org/10.1097/01.brs.0000232...
,2020. Cason GW, Herkowitz HN. Cervical intervertebral disc
replacement. J Bone Joint Surg Am. 2013;95(3):279-85,
10.2106/JBJS.J.01042
http://dx.doi.org/10.2106/JBJS.J.01042...
). Metals provide the necessary strength,
ductility, and toughness required for load bearing, whereas some polymers provide
low-friction surfaces for articulation and shock absorption (2020. Cason GW, Herkowitz HN. Cervical intervertebral disc
replacement. J Bone Joint Surg Am. 2013;95(3):279-85,
10.2106/JBJS.J.01042
http://dx.doi.org/10.2106/JBJS.J.01042...
). Some artificial discs, such as Prestige and CerviCore,
have articulating metal-on-metal surfaces, and long-term follow-up has indicated
their safety (55. Colle KO, Butler JB, Reyes PM, Newcomb AG, Theodore N, Crawford
NR. Biomechanical evaluation of a metal-on-metal cervical intervertebral disc
prosthesis. Spine J. 2013;13(11):1640-9,
10.1016/j.spinee.2013.06.026
http://dx.doi.org/10.1016/j.spinee.2013....
). Because of manufacturing
limitations, we preliminary designed the ADVS using titanium alloy.
Theoretically, spinal fusion leads to a loss of motion of the fusion segment and
increased motion of the adjacent upper and lower segments. In contrast, the motion
of the segment is restored after ADVC implantation. In this study, we found that the
non-fusion group did not show any difference in the ROM of C3-7 compared
with the intact group, but it showed significant differences compared with the
fusion group in all directions except lateral bending. After ADVS implantation, the
ROM of C4-6 increased significantly. These results suggest that the ADVS
could preserve motion in the surgical area. However, the ROM of adjacent segments
(C3-4, C6-7) in the non-fusion group decreased
significantly only in some directions compared with the fusion group. There are two
possible explanations for this finding. First, the movement of the cervical vertebra
from C3 to C7 is a coupled motion that is closely related to
the facet joint (2121. Cepoiu-Martin M, Faris P, Lorenzetti D, Prefontaine E,
Noseworthy T, Sutherland L. Artificial cervical disc arthroplasty: a systematic
review. Spine (Phila Pa 1976). 2011;36(25):E1623-33,
10.1097/BRS.0b013e3182163814
http://dx.doi.org/10.1097/BRS.0b013e3182...
), and the cervical ROM of
each direction after ADVS implantation is unequal to that of the intact cervical
spine. Because there is a 45° angle between the sagittal and horizontal planes
of the facet joint, cervical lateral bending is often accompanied by axial rotation
(2222. Davis RJ, Kim KD, Hisey MS, Hoffman GA, Bae HW, Gaede SE, et al.
Cervical total disc replacement with the Mobi-C cervical artificial disc
compared with anterior discectomy and fusion for treatment of 2-level
symptomatic degenerative disc disease: a prospective, randomized, controlled
multicenter clinical trial. J Neurosurg Spine. 2013;19(5):532-45,
10.3171/2013.6.SPINE12527
http://dx.doi.org/10.3171/2013.6.SPINE12...
,2323. Tian W, Han X, Li ZY, Mao JP, Sun YQ, Albert TJ. Reversal of
Anterior Cervical Discectomy and Fusion With Cervical Artificial Disc
Replacement Regain Motion After 9 Years Fusion. Journal of Spinal Disorders
& Techniques. 2013;26(1):55-9.) (1616. Qin J, He X, Wang D, Qi P, Guo L, Huang S, et al. Artificial
cervical vertebra and intervertebral complex replacement through the anterior
approach in animal model: a biomechanical and in vivo evaluation of a successful
goat model. PLoS One. 2012;7(12):e52910,
10.1371/journal.pone.0052910
http://dx.doi.org/10.1371/journal.pone.0...
). When the cervical spine
bends to the left, for example, the lower left zygopophysis of the upper vertebra
will move down along the upper left zygopophysis of the lower vertebra, shifting the
right side of the upper vertebra forward. Thus, the comprehensive movement is
left-axial rotation, and the spinous process moves to the right. In our study, the
facet joint of the C5 vertebra was still intact after ADVS implantation;
thus, the ROM of the non-fusion group could not be maintained at 12° in
flexion/extension and lateral bending. Second, the instant center of rotation (ICR)
should also be considered, as it has been proposed for evaluating the quality of
spine movement (2424. Qin J, He X, Wang D, Qi P, Guo L, Huang S, et al. Artificial
cervical vertebra and intervertebral complex replacement through the anterior
approach in animal model: a biomechanical and in vivo evaluation of a successful
goat model. PLoS One. 2012;7(12):e52910,
10.1371/journal.pone.0052910
http://dx.doi.org/10.1371/journal.pone.0...
). The path of the ICR
during dynamic motion has been reported as moving superiorly with each successive
motion segment from C2-3 to C6-7 (2424. Qin J, He X, Wang D, Qi P, Guo L, Huang S, et al. Artificial
cervical vertebra and intervertebral complex replacement through the anterior
approach in animal model: a biomechanical and in vivo evaluation of a successful
goat model. PLoS One. 2012;7(12):e52910,
10.1371/journal.pone.0052910
http://dx.doi.org/10.1371/journal.pone.0...
). The ADVS does not have a dynamic ICR, which contributes to
the increased ROM in extension and lateral bending. The SI-ROM indicated the
stability that the instrumentation to the spine (1111. Zhang J, He XJ, Li HP, Wang D, Zhao WD, Xu JH, et al.
Biomechanical study of anterior cervical corpectomy and step-cut grafting with
bioabsorbable screws fixation in cadaveric cervical spine model. Spine.
2006;31(19):2195-201, 10.1097/01.brs.0000232798.97075.73
http://dx.doi.org/10.1097/01.brs.0000232...
). The motion of C4-6 was redistributed into the adjacent
level because the fusion procedure causes the ROM of this area to disappear. ADVS
implantation increased the ROM of lateral bending and axial rotation, resulting in a
negative SI-ROM in most directions. However, no significant difference was found
between the SI-ROMs of the non-fusion and fusion groups, except at C4-6.
This result suggests that ADVS implantation could provide a stable biomechanical
environment for the cervical spine.
The limitations of this study must be acknowledged. Although our results suggest that
the ADVS preserves the dynamic function of the intervertebral space and reconstructs
the vertebral height, the results should be cautiously accepted because of the
study’s low power. The use of larger samples should be considered in future
studies. Endurance tests such as the fatigue test, the tensile test, the compression
test, the shear test and the pull-out test were not performed. Titanium-on-titanium
has historically been a poor bearing surface, and in vitro biomechanical testing is
necessary to pre-clinically evaluate new surgical procedures and implants (2525. Wu ZX, Han BJ, Zhao X, Kong L, Liu D, Cui G, et al.
Biomechanical evaluation of a novel total cervical prosthesis in a single-level
cervical subtotal corpectomy model: an in vitro human cadaveric study. J Surg
Res. 2012;175(1):76-81, 10.1016/j.jss.2011.02.022
http://dx.doi.org/10.1016/j.jss.2011.02....
). The prosthesis has a high profile, which
may cause such complications as dysphagia and esophageal perforation. We will
establish an animal model to test the biomechanics of a low-profile prosthesis made
of cobalt-chromium alloy and high molecular weight polyethylene (HMWPE) in future
experiments.
We thank Ms. Yang and her colleagues from the surgical laboratory of the Second Affiliated Hospital of Xian Jiaotong University for their help with preparing the instruments.
This work was supported by funding from the Ph.D. Programs Foundation of the Ministry of Education of China (No.: 20120201130009). No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
REFERENCES
-
1Emery SE, Bolesta MJ, Banks MA, Jones PK. Robinson anterior cervical fusion comparison of the standard and modified techniques. Spine (Phila Pa 1976). 1994;19(6):660-3, 10.1097/00007632-199403001-00004
» http://dx.doi.org/10.1097/00007632-199403001-00004 -
2McGuire RA, St John K. Comparison of anterior cervical fusions using autogenous bone graft obtained from the cervical vertebrae to the modified Smith-Robinson technique. J Spinal Disord. 1994;7(6):499-503.
-
3Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH. Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. Journal of Bone and Joint Surgery-American Volume. 1999;81A(4):519-28.
-
4Matsumoto M, Nojiri K, Chiba K, Toyama Y, Fukui Y, Kamata M. Open-door laminoplasty for cervical myelopathy resulting from adjacent-segment disease in patients with previous anterior cervical decompression and fusion. Spine. 2006;31(12):1332-7, 10.1097/01.brs.0000218632.82159.2b
» http://dx.doi.org/10.1097/01.brs.0000218632.82159.2b -
5Colle KO, Butler JB, Reyes PM, Newcomb AG, Theodore N, Crawford NR. Biomechanical evaluation of a metal-on-metal cervical intervertebral disc prosthesis. Spine J. 2013;13(11):1640-9, 10.1016/j.spinee.2013.06.026
» http://dx.doi.org/10.1016/j.spinee.2013.06.026 -
6Wigfield CC, Gill SS, Nelson RJ, Metcalf NH, Robertson JT. The new Frenchay artificial cervical joint - Results from a two-year pilot study. Spine. 2002;27(22):2446-52, 10.1097/00007632-200211150-00006
» http://dx.doi.org/10.1097/00007632-200211150-00006 -
7Bilbao G, Duart M, Aurrecoechea JJ, Pomposo I, Igartua A, Catalan G, et al. Surgical results and complications in a series of 71 consecutive cervical spondylotic corpectomies. Acta Neurochir (Wien). 2010;152(7):1155-63.
-
8Chen JF, Lee ST. Antibiotic-polymethylmethacrylate strut: an option for treating cervical pyogenic spondylitis. J Neurosurg. 2006;5(1):90-5.
-
9Nuckley DJ, Konodi MA, Raynak GC, Ching RP, Chapman JR, Mirza SK. Neural space integrity of the lower cervical spine: Effect of anterior lesions. Spine. 2004;29(6):642-9, 10.1097/01.BRS.0000115132.49734.33
» http://dx.doi.org/10.1097/01.BRS.0000115132.49734.33 -
10Snijders CJ, Vandijke GAH, Roosch ER. A biomechanical model for the analysis of the cervical-spine in static postures. J Biomech. 1991;24(9):783-92, 10.1016/0021-9290(91)90303-5
» http://dx.doi.org/10.1016/0021-9290(91)90303-5 -
11Zhang J, He XJ, Li HP, Wang D, Zhao WD, Xu JH, et al. Biomechanical study of anterior cervical corpectomy and step-cut grafting with bioabsorbable screws fixation in cadaveric cervical spine model. Spine. 2006;31(19):2195-201, 10.1097/01.brs.0000232798.97075.73
» http://dx.doi.org/10.1097/01.brs.0000232798.97075.73 -
12Cason GW, Herkowitz HN. Cervical intervertebral disc replacement. J Bone Joint Surg Am. 2013;95(3):279-85, 10.2106/JBJS.J.01042
» http://dx.doi.org/10.2106/JBJS.J.01042 -
13Cepoiu-Martin M, Faris P, Lorenzetti D, Prefontaine E, Noseworthy T, Sutherland L. Artificial cervical disc arthroplasty: a systematic review. Spine (Phila Pa 1976). 2011;36(25):E1623-33, 10.1097/BRS.0b013e3182163814
» http://dx.doi.org/10.1097/BRS.0b013e3182163814 -
14Davis RJ, Kim KD, Hisey MS, Hoffman GA, Bae HW, Gaede SE, et al. Cervical total disc replacement with the Mobi-C cervical artificial disc compared with anterior discectomy and fusion for treatment of 2-level symptomatic degenerative disc disease: a prospective, randomized, controlled multicenter clinical trial. J Neurosurg Spine. 2013;19(5):532-45, 10.3171/2013.6.SPINE12527
» http://dx.doi.org/10.3171/2013.6.SPINE12527 -
15Tian W, Han X, Li ZY, Mao JP, Sun YQ, Albert TJ. Reversal of Anterior Cervical Discectomy and Fusion With Cervical Artificial Disc Replacement Regain Motion After 9 Years Fusion. Journal of Spinal Disorders & Techniques. 2013;26(1):55-9.
-
16Qin J, He X, Wang D, Qi P, Guo L, Huang S, et al. Artificial cervical vertebra and intervertebral complex replacement through the anterior approach in animal model: a biomechanical and in vivo evaluation of a successful goat model. PLoS One. 2012;7(12):e52910, 10.1371/journal.pone.0052910
» http://dx.doi.org/10.1371/journal.pone.0052910 -
17Wu ZX, Han BJ, Zhao X, Kong L, Liu D, Cui G, et al. Biomechanical evaluation of a novel total cervical prosth9. Nuckley DJ, Konodi MA, Raynak GC, Ching RP, Chapman JR, Mirza SK. Neural space integrity of the lower cervical spine: Effect of anterior lesions. Spine. 2004;29(6):642-9, 10.1097/01.BRS.0000115132.49734.33
» http://dx.doi.org/10.1097/01.BRS.0000115132.49734.33 -
18Snijders CJ, Vandijke GAH, Roosch ER. A biomechanical model for the analysis of the cervical-spine in static postures. J Biomech. 1991;24(9):783-92, 10.1016/0021-9290(91)90303-5
» http://dx.doi.org/10.1016/0021-9290(91)90303-5 -
19Zhang J, He XJ, Li HP, Wang D, Zhao WD, Xu JH, et al. Biomechanical study of anterior cervical corpectomy and step-cut grafting with bioabsorbable screws fixation in cadaveric cervical spine model. Spine. 2006;31(19):2195-201, 10.1097/01.brs.0000232798.97075.73
» http://dx.doi.org/10.1097/01.brs.0000232798.97075.73 -
20Cason GW, Herkowitz HN. Cervical intervertebral disc replacement. J Bone Joint Surg Am. 2013;95(3):279-85, 10.2106/JBJS.J.01042
» http://dx.doi.org/10.2106/JBJS.J.01042 -
21Cepoiu-Martin M, Faris P, Lorenzetti D, Prefontaine E, Noseworthy T, Sutherland L. Artificial cervical disc arthroplasty: a systematic review. Spine (Phila Pa 1976). 2011;36(25):E1623-33, 10.1097/BRS.0b013e3182163814
» http://dx.doi.org/10.1097/BRS.0b013e3182163814 -
22Davis RJ, Kim KD, Hisey MS, Hoffman GA, Bae HW, Gaede SE, et al. Cervical total disc replacement with the Mobi-C cervical artificial disc compared with anterior discectomy and fusion for treatment of 2-level symptomatic degenerative disc disease: a prospective, randomized, controlled multicenter clinical trial. J Neurosurg Spine. 2013;19(5):532-45, 10.3171/2013.6.SPINE12527
» http://dx.doi.org/10.3171/2013.6.SPINE12527 -
23Tian W, Han X, Li ZY, Mao JP, Sun YQ, Albert TJ. Reversal of Anterior Cervical Discectomy and Fusion With Cervical Artificial Disc Replacement Regain Motion After 9 Years Fusion. Journal of Spinal Disorders & Techniques. 2013;26(1):55-9.
-
24Qin J, He X, Wang D, Qi P, Guo L, Huang S, et al. Artificial cervical vertebra and intervertebral complex replacement through the anterior approach in animal model: a biomechanical and in vivo evaluation of a successful goat model. PLoS One. 2012;7(12):e52910, 10.1371/journal.pone.0052910
» http://dx.doi.org/10.1371/journal.pone.0052910 -
25Wu ZX, Han BJ, Zhao X, Kong L, Liu D, Cui G, et al. Biomechanical evaluation of a novel total cervical prosthesis in a single-level cervical subtotal corpectomy model: an in vitro human cadaveric study. J Surg Res. 2012;175(1):76-81, 10.1016/j.jss.2011.02.022
» http://dx.doi.org/10.1016/j.jss.2011.02.022 -
26Jian Y, Lan-Tao L, Jian-ning Z. Design and preliminary biomechanical analysis of artificial cervical joint complex. Arch Orthop Trauma Surg. 2013;133(6):735-43, 10.1007/s00402-013-1717-6
» http://dx.doi.org/10.1007/s00402-013-1717-6 -
27Yi S, Lee DY, Kim DH, Ahn PG, Kim KN, Shin HC, et al. Cervical artificial disc replacement - Part 1: History, design, and overview of the cervical artificial disc. Neurosurg Q. 2008;18(2):89-95, 10.1097/WNQ.0b013e318172f349
» http://dx.doi.org/10.1097/WNQ.0b013e318172f349 -
28Durbhakula MM, Ghiselli G. Cervical total disc replacement, part I: rationale, biomechanics, and implant types. Orthop Clin North Am. 2005;36(3):349-54, 10.1016/j.ocl.2005.02.011
» http://dx.doi.org/10.1016/j.ocl.2005.02.011 -
29Mimura M, Moriya H, Watanabe T, Takahashi K, Yamagata M, Tamaki T. 3-dimensional motion analysis of the cervical-spine with special reference to the axial rotation. Spine. 1989;14(11):1135-9, 10.1097/00007632-198911000-00001
» http://dx.doi.org/10.1097/00007632-198911000-00001 -
30Ishii T, Mukai Y, Hosono N, Sakaura H, Fujii R, Nakajima Y, et al. Kinematics of the subaxial cervical spine in rotation in vivo three-dimensional analysis. Spine. 2004;29(24):2826-31, 10.1097/01.brs.0000147806.31675.6b
» http://dx.doi.org/10.1097/01.brs.0000147806.31675.6b -
31Ishii T, Mukai Y, Hosono N, Sakaura H, Fujii R, Nakajima Y, et al. Kinematics of the cervical spine in lateral bending in vivo three-dimensional analysis. Spine. 2006;31(2):155-60, 10.1097/01.brs.0000195173.47334.1f
» http://dx.doi.org/10.1097/01.brs.0000195173.47334.1f -
32Anderst W, Baillargeon E, Donaldson W, Lee J, Kang J. Motion path of the instant center of rotation in the cervical spine during in vivo dynamic flexion-extension: implications for artificial disc design and evaluation of motion quality after arthrodesis. Spine (Phila Pa 1976). 2013;38(10):E594-601, 10.1097/BRS.0b013e31828ca5c7
» http://dx.doi.org/10.1097/BRS.0b013e31828ca5c7 -
33Wilke HJ, Geppert J, Kienle A. Biomechanical in vitro evaluation of the complete porcine spine in comparison with data of the human spine. Eur Spine J. 2011;20(11):1859-68, 10.1007/s00586-011-1822-6
» http://dx.doi.org/10.1007/s00586-011-1822-6
Publication Dates
-
Publication in this collection
July 2015
History
-
Received
20 Dec 2014 -
Reviewed
17 Mar 2015 -
Accepted
30 Apr 2015