
Abstract
Objective
To describe the self-reported prevalence of intellectual disability, physical, hearing and visual, according to sociodemographic variables, degree of limitation and frequency of rehabilitation service use.
Methods
Data from the National Health Survey, a population survey. the self-reported prevalence of physical, mental, visual and hearing were calculated and their 95% confidence intervals, stratified by sex, age, race / color, for Brazil, place of residence and Major Regions.
Results
The prevalence of self-reported disability in the country was 6.2% (12.4 million people). The prevalence of disability was 1.3% higher in men, in people aged 60 or more in the Northeast. Visual impairment was more prevalent (3.6%), increased with age, as well as hearing loss. Acquired deficiency was higher in relation to the birth (except intellectual). Lesser degree of limitation was observed among those who reported visual impairment and the use of health services was less frequent.
Conclusion
It is necessary to expand access to health promotion, early diagnosis and treatment, as well as strengthen public policies aimed at this population.
Disabled persons; Self report; Health surveys; Health inequalities
Resumo
Objetivo
descrever a prevalência autorreferida das deficiências intelectual, física, auditiva e visual, segundo variáveis sociodemográficas, grau de limitação e frequência de uso de serviço de reabilitação.
Métodos
Dados provenientes da Pesquisa Nacional de Saúde, inquérito populacional. Foram calculadas as prevalências autorreferidas de deficiência física, mental, visual e auditiva e seus intervalos de confiança de 95%, estratificados por sexo, faixa etária, raça/cor, para Brasil, local de residência e Grandes Regiões.
Resultados
a prevalência de deficiência autorreferida no país foi de 6,2% (12,4 milhões de pessoas). A prevalência de deficiência física foi de 1,3%, maior em homens, em indivíduos com 60 anos ou mais na região Nordeste. A deficiência visual foi mais prevalente (3,6%), aumentou com a idade, assim como deficiência auditiva. A deficiência adquirida foi maior em relação à de nascença (exceto intelectual). Menor grau de limitação foi observado entre os que referiram deficiência visual e o uso de serviços de saúde foi menos frequente.
Conclusão
há necessidade de ampliar o acesso às ações de promoção, diagnóstico e tratamento precoce, bem como o fortalecer políticas públicas direcionadas a esta população.
Pessoas com deficiência; Autorrelato; Inquéritos epidemiológicos; Desigualdades em saúde
Introduction
One billion people is estimated to have some kind of impairment or disability, which accounts for approximately 15% of the worldwide population11. World Health Organization (WHO). World report on disability. [acessado 2015 set 20]. Disponível em: http://www.larchetoronto.org/wordpress/wp-content/uploads/2012/01/launch-of-World-Report-on-Disability-Jan-27-121.pdf
http://www.larchetoronto.org/wordpress/w...
. According to WHO, at least 10% of the children worldwide are born with or acquire some type of physical, mental or sensory disability that leads to negative influences on their development. Additionally, the access to rehabilitation is very unequal; in developing countries, only 3% of the people in need of assistance are provided some kind of rehabilitation service22. World Health Organization (WHO). Disability and Rehabilitation: Future, Trends and Challenges in Rehabilitation. Geneva: WHO; 2002..
Brazilian laws define disability as the loss or abnormality of a psychological, physiological or anatomical structure or function that renders the execution of an activity impossible within what would be considered normal for human beings33. Brasil. Presidência da República. Decreto nº 3.298, de 20 de dezembro de 1999. Regulamenta a Lei no 7.853, de 24 de outubro de 1989, dispõe sobre a Política Nacional para a Integração da Pessoa Portadora de Deficiência, consolida as normas de proteção, e dá outras providências. Diário Oficial da União 1999; 21 dez.. The Continued Payment Benefit Law establishes that a person with disability is someone who presents long-term (at least two years) disabilities of physical, mental, intellectual or sensory nature44. Brasil. Presidência da República. Lei nº 12.470, de 31 de agosto de 2011. Altera os arts. 21 e 24 da Lei no 8.212, de 24 de julho de 1991, que dispõe sobre o Plano de Custeio da Previdência Social, para estabelecer alíquota diferenciada de contribuição para o microempreendedor individual e do segurado facultativo sem renda própria que se dedique exclusivamente ao trabalho doméstico no âmbito de sua residência, desde que pertencente a família de baixa renda; altera os arts. 16, 72 e 77 da Lei no 8.213, de 24 de julho de 1991, que dispõe sobre o Plano de Benefícios da Previdência Social, para incluir o filho ou o irmão que tenha deficiência intelectual ou mental como dependente e determinar o pagamento do salário-maternidade devido à empregada do microempreendedor individual diretamente pela Previdência Social; altera os arts. 20 e 21 e acrescenta o art. 21-A à Lei no 8.742, de 7 de dezembro de 1993 - Lei Orgânica de Assistência Social, para alterar regras do benefício de prestação continuada da pessoa com deficiência; e acrescenta os §§ 4o e 5o ao art. 968 da Lei no 10.406, de 10 de janeiro de 2002 - Código Civil, para estabelecer trâmite especial e simplificado para o processo de abertura, registro, alteração e baixa do microempreendedor individual. Diário Oficial da União 2011; 1 set..
The concept of disability is evolving, as well as the understanding of the role performed by healthcare professionals and services, aiming to creating a wider foundation for social inclusion55. Freita MNC. A Inserção de Pessoas com Deficiência em Empresas Brasileiras. Um Estudo sobre as Relações entre Concepções de Deficiência, Condições de Trabalho e Qualidade de Vida no Trabalho [tese]. Belo Horizonte: Universidade Federal de Minas Gerais; 2007.. However, Ancient Greece handed down to Western civilization its views on disabilities: back then, disabilities were considered an event that would make survival/living difficult, because the person would not have the necessary energy and strength to deal with agriculture or to fight a war55. Freita MNC. A Inserção de Pessoas com Deficiência em Empresas Brasileiras. Um Estudo sobre as Relações entre Concepções de Deficiência, Condições de Trabalho e Qualidade de Vida no Trabalho [tese]. Belo Horizonte: Universidade Federal de Minas Gerais; 2007..
Such interpretation remained through other historical contexts – always linked to social exclusion. After the end of World War II, the scenario began to change, as Europe was in need of men for its labor market. The veterans of war, even when mutilated in the battles, had distinguished social and cultural qualities, marking the beginning of labor rights laws in that continent55. Freita MNC. A Inserção de Pessoas com Deficiência em Empresas Brasileiras. Um Estudo sobre as Relações entre Concepções de Deficiência, Condições de Trabalho e Qualidade de Vida no Trabalho [tese]. Belo Horizonte: Universidade Federal de Minas Gerais; 2007.. From that point on, after several efforts were made by social movements, legal advancements have been obtained in several countries in terms of rights and protection33. Brasil. Presidência da República. Decreto nº 3.298, de 20 de dezembro de 1999. Regulamenta a Lei no 7.853, de 24 de outubro de 1989, dispõe sobre a Política Nacional para a Integração da Pessoa Portadora de Deficiência, consolida as normas de proteção, e dá outras providências. Diário Oficial da União 1999; 21 dez.
4. Brasil. Presidência da República. Lei nº 12.470, de 31 de agosto de 2011. Altera os arts. 21 e 24 da Lei no 8.212, de 24 de julho de 1991, que dispõe sobre o Plano de Custeio da Previdência Social, para estabelecer alíquota diferenciada de contribuição para o microempreendedor individual e do segurado facultativo sem renda própria que se dedique exclusivamente ao trabalho doméstico no âmbito de sua residência, desde que pertencente a família de baixa renda; altera os arts. 16, 72 e 77 da Lei no 8.213, de 24 de julho de 1991, que dispõe sobre o Plano de Benefícios da Previdência Social, para incluir o filho ou o irmão que tenha deficiência intelectual ou mental como dependente e determinar o pagamento do salário-maternidade devido à empregada do microempreendedor individual diretamente pela Previdência Social; altera os arts. 20 e 21 e acrescenta o art. 21-A à Lei no 8.742, de 7 de dezembro de 1993 - Lei Orgânica de Assistência Social, para alterar regras do benefício de prestação continuada da pessoa com deficiência; e acrescenta os §§ 4o e 5o ao art. 968 da Lei no 10.406, de 10 de janeiro de 2002 - Código Civil, para estabelecer trâmite especial e simplificado para o processo de abertura, registro, alteração e baixa do microempreendedor individual. Diário Oficial da União 2011; 1 set.-55. Freita MNC. A Inserção de Pessoas com Deficiência em Empresas Brasileiras. Um Estudo sobre as Relações entre Concepções de Deficiência, Condições de Trabalho e Qualidade de Vida no Trabalho [tese]. Belo Horizonte: Universidade Federal de Minas Gerais; 2007..
The most currently and internationally accepted concept, drawn from International Classification of Functioning (ICF), is based on environmental factors and each individual’s potentials, without being restricted exclusively to incapabilities and limitations of people with disabilities66. Farias N, Buchalla CMA. Classificação Internacional de Funcionalidade, Incapacidade e Saúde da Organização Mundial da Saúde: Conceitos, Usos e Perspectivas. Rev Bras Epidemiol 2005; 8(2):187-193.. Such classification establishes that functioning is based on components of functions and body structures, activities and participation in social life. The concept of incapability, on the other hand, is defined as the result of interacting dysfunctions presented by the individual, limitation of their activities and restricted social participation, in addition to environmental factors55. Freita MNC. A Inserção de Pessoas com Deficiência em Empresas Brasileiras. Um Estudo sobre as Relações entre Concepções de Deficiência, Condições de Trabalho e Qualidade de Vida no Trabalho [tese]. Belo Horizonte: Universidade Federal de Minas Gerais; 2007..
Disability is seen as a consequence resulting from individual’s health conditions and diseases; context of physical and social environments; different cultural perceptions and attitudes regarding disabilities; and availability of services and specific laws. Thus, ICF is not characterized only as a tool to measure the functional status of impaired people; it also allows assessing life conditions and helping to access social inclusion policies66. Farias N, Buchalla CMA. Classificação Internacional de Funcionalidade, Incapacidade e Saúde da Organização Mundial da Saúde: Conceitos, Usos e Perspectivas. Rev Bras Epidemiol 2005; 8(2):187-193..
Studies have demonstrated that some population groups seem to be more susceptible to disabilities. Aspects such as age group, sex, education and income seem to be more associated to a given type and level of disability66. Farias N, Buchalla CMA. Classificação Internacional de Funcionalidade, Incapacidade e Saúde da Organização Mundial da Saúde: Conceitos, Usos e Perspectivas. Rev Bras Epidemiol 2005; 8(2):187-193.,77. World Health Organization (WHO). Towards a Common Language for Functioning, Disability and Health – ICF. Genebra: WHO; 2002..
Prevalence studies, surveys and national inquiries about disability are complex due to several measurement challenges on which comparable data are based88. Instituto Brasileiro de Geografia e Estatística (IBGE). Censo Demográfico 2010. [acessado 2015 out 16]. Disponível em: http://censo2010.ibge.gov.br/
http://censo2010.ibge.gov.br/...
,99. Brasil. Ministério da Saúde (MS). Cartilha do Censo 2010 – Pessoas com Deficiência. Brasília: SDHPR/ SNPD; 2012.. We reiterate the complexity of the phenomenon – both regarding theoretical and conceptual discussion around the term, such as the use of different expressions, typologies, terminologies1010. Szwarcwald CL, Malta DC, Pereira CA, Vieira MLFP, Conde WL, Souza Júnior PRB, Damacena GN, Azevedo LO, Azevedo e Silva G, Theme Filha MM, Lopes CS, Romero DE, Almeida WS, Monteiro CA. Pesquisa Nacional de Saúde no Brasil: concepção e metodologia de aplicação. Cien Saude Colet 2014; 19(2):333-342..
The Brazilian National Health Survey (NHS) includes self-referred disabilities (intellectual, physical, hearing and visual) as the subject, aiming at supporting the public policies planning1010. Szwarcwald CL, Malta DC, Pereira CA, Vieira MLFP, Conde WL, Souza Júnior PRB, Damacena GN, Azevedo LO, Azevedo e Silva G, Theme Filha MM, Lopes CS, Romero DE, Almeida WS, Monteiro CA. Pesquisa Nacional de Saúde no Brasil: concepção e metodologia de aplicação. Cien Saude Colet 2014; 19(2):333-342..
The objective of this document is to describe the self-referred prevalence of intellectual, physical, hearing and visual disabilities in Brazil, according to social/demographical variables, level of limitation and frequency of use rehabilitation services.
Methods
The National Health Survey (NHS) is a nation-wide survey carried out by Ministry of Health along with Brazilian Institute of Geography and Statistics (IBGE) and whose data was collected from each household between August 2013 and February 2014. NHS is part of IBGE’s Integrated Household Survey (IHS) and uses a master sample from that system, which allows better geographical dissemination and improved precision in estimates.
The NHS sample was comprised of clusters in three selection stages. In the first stage, primary sampling units (PSUs), comprised of census regions, were selected. During the second stage, a fixed number (10-14) of private households was selected in each PSU. For the third stage, an individual who is 18 years old or older was selected from each sampled household. For all stages of the NHS sample, a simple random sample was used as selection method1111. Instituto Brasileira de Geografia e Estatística (IBGE). Acesso e Utilização dos Serviços de Saúde, Acidentes e Violências. Rio de Janeiro: IBGE; 2015..
Regarding the sample, out of the 81,254 homes selected, 69,994 were habited. 64,348 interviews were carried out, with loss rate of 20.8% and response rate of 91.9%. The sample was established by considering the level of precision wanted for the estimations of some indicators of interest, allowing for estimation of some parameters in different geographic levels of disaggregation1111. Instituto Brasileira de Geografia e Estatística (IBGE). Acesso e Utilização dos Serviços de Saúde, Acidentes e Violências. Rio de Janeiro: IBGE; 2015..
The data was collected using handheld computers (Personal Digital Assistant, PDA), programmed to assess the input values. The NHS questionnaire is divided into three parts: information about the household; information about all the individuals living in it, provided by a proxy; information about a select individual (adult who is 18 years old or older)1111. Instituto Brasileira de Geografia e Estatística (IBGE). Acesso e Utilização dos Serviços de Saúde, Acidentes e Violências. Rio de Janeiro: IBGE; 2015..
Thus, valid information was collected from 205,000 dwellers. During data analysis, expansion factors or sample weights were used for PSUs, households, all the residents in a given home and select resident1111. Instituto Brasileira de Geografia e Estatística (IBGE). Acesso e Utilização dos Serviços de Saúde, Acidentes e Violências. Rio de Janeiro: IBGE; 2015..
The classification of disability was per the Brazilian laws; according to those laws, hearing disability is defined as bilateral, partial or total hearing loss, of forty one decibels (dB) or higher, established by audiogram in the frequencies of 500Hz, 1,000Hz, 2,000Hz and 3,000Hz.
In order to establish the hearing loss based on the legal definition, NHS asked the following questions:
a) G14 ... Is any hearing disability present? (1. Yes; 2. No); G16. What type of hearing disability? (1. Deafness involving both ears; 2. Deafness involving one ear and reduced hearing in the other; 3. Deafness involving one ear and normal hearing in the other; 4 Reduced hearing in both ears; 5. Reduced hearing in one of the ears);
Calculation method: Numerator: number of individuals with hearing disability (G14 = 1 and (G16 = 1 or G16 = 2 or G16 = 4)) / Denominator: number of respondents
Thus, the subject with normal hearing in one ear is not considered impaired, neither someone with reduced hearing in one ear.
b) In order to consider whether the disability is acquired or if the individual was born with it, please consider Yes as a response to the following question (G15). _... was born with hearing disability or was the disability acquired? (1 Born with disability 2. Acquired. How old were the person when that happened?).
c) G17. Overall, to what extent does the hearing disability limit the daily life activities? (1. It does not limit; 2. A little; 3. Moderately; 4. Severely; 5. Very severely).
High limitation was considered those with severe/very severe level of limitation.
d) G18. Any rehabilitation service is used due to hearing disability? (1. Yes 2. No).
Mental disability is considered intellectual functioning significantly lower to the average, expressed before 18 years of age and limitations associated to two or more adaptive abilities, such as: communication; personal care; social abilities; use of community resources; health and safety; academic abilities; leisure; and work.
The method to calculate intellectual disability was similar to what was previously described, as well as with physical disability.
Visual disability or blindness were based on the legal definition in which visual acuity is the same or below 0.05 (best eye) with the best optical correction; poor vision, which means visual acuity between 0.3 and 0.05 (best eye) with the best optical correction; the cases in which the sum of the visual field measurement in both eyes is equal to or below 60o; or the simultaneous occurrence of any of the previous conditions. In this case, visual disability was considered for anyone who answered Yes to the following question: G21 ... Is any hearing disability present? (1. Yes; 2. No); G23. What type of visual disability? (1. Blindness of both eyes; 2. Blindness of one eye and reduced eyesight in the other; 3 Blindness in one eye and normal view in the other; 4. Poor vision in both eyes; 5. Poor vision in one of the eyes).
Calculation method: Numerator: number of individuals with visual disability (G21 = 1) and (G23 = 1 or G23 = 2 or G23 = 3 or G23 = 4 or G23 = 5). / Denominator: number of respondents.
Multiple disabilities were association of two or more disabilities1212. Brasil. Presidência da República. Decreto nº 5.296, de 2 de dezembro de 2004. Regulamenta as Leis nos 10.048, de 8 de novembro de 2000, que dá prioridade de atendimento às pessoas que especifica, e 10.098, de 19 de dezembro de 2000, que estabelece normas gerais e critérios básicos para a promoção da acessibilidade das pessoas portadoras de deficiência ou com mobilidade reduzida, e dá outras providências. Diário Oficial da União 2000; 3 dez..
When analyzing this study, data was presented for a total of self-referred disabilities and each type separately: intellectual, physical, hearing and visual. Six indicators were assessed:
1. Ratio of disabled people (i.e., total, intellectual, physical, hearing or visual). (Number of people with disability/total number of residents);
2. Ratio of people who were born with disability (number of people who referred having born with disability / total number of residents);
3. Ratio of people with acquired disability (number of people who referred having acquired disability / total number of residents);
4. Ratio of people with disability and severe/very severe limitation or who cannot perform daily life activities (number of people who referred having a severe/very severe limitation/total number of residents);
5. Ratio of people with disability and with little or no limitation to perform daily life activities (number of people who referred little or no limitation to perform daily life activities/total number of residents);
6. Ratio of disabled people who attend some type of rehabilitation service (number of people on rehabilitation/total number of residents);
The indicators of referred prevalence in all the four types of disabilities were stratified into Brazil, macroregions (North, Northeast, Southeast, South and West Central), setting (urban/rural), sex (male/female), age group (0-9, 10-17, 18-29, 30-39, 40-59, 60 years old or older), color or race (white, black and light brown). The prevalence and their respective 95% confidence intervals (95% CI) was described, presenting absolute values. When there was no overlapping of confidence intervals, the difference was considered statistically significant. The remaining indicators were assessed only for Brazil and setting (urban/rural).
Data was assessed by Stata 11.0 software solution, using the “Survey” module, which takes into account the effects of complex sampling. NHS was approved by CONEP (Comissão Nacional de Ética em Pesquisas, National Committee for Ethics in Research) in June 2013. By the time of the interview, all individuals were asked, clarified and accepted to take part in the survey.
Results
The prevalence of self-referred disability in Brazil was 6.2% (95% CI, 5.9-6.5), or approximately 12.4 million people, with no difference between men and women. The difference tended to increase with age, with significant differences reported by age groups 40 to 59 years old: 8.1% (95% CI, 7.6-8.6); and 60 years old or older 18.2% (95% CI, 17.2-19.2). There was no difference according to race/skin color. The prevalence was higher in the rural setting 7.4% (6.7-8.3) and the highest prevalence was seen in the South region 8.4% (95% CI, 7.5-9.3), as described on Table 1.
Self-referred prevalence of disabilities in the Brazilian population, as per social and demographic characteristics. National Health Survey, 2013, Brazil.
The prevalence of intellectual disability in population was 0.8% (95% CI, 0.7; 0.8); higher among men, no differences in age group, race/skin color and macroregions (Table 2).
Self-referred prevalence of intellectual, physical, hearing and visual disabilities in the Brazilian population, as per social and demographic characteristics. National Health Survey, 2013, Brazil.
Physical disability was 1.3% (95% CI: 1.2-1.4), or 2.6 million people, and higher among men (1.6%, 95% CI: 1.5-1.8) than among women (1.0%, 95% CI: 0.9-1.1). Regarding age group, prevalence increased with age, being higher for individuals who are 60 years old or older (3.3%, 95% CI: 2.9-3.6). For race or color, a higher percentage was seen among black individuals, however with no statistically significant difference. There was no difference between urban and rural setting. When it comes to regions, a higher prevalence of physical disability was seen in Northeast region (1.6%, 95% CI: 1.4-1.8) when compared to Southeast (1.2%, 95% CI: 1.0-1.3) and North (1.1%, 95% CI: 0.9-1.3) (Table 2).
Regarding hearing disability, the prevalence was 1.1% (95% CI, 1.0-1.2), or approximately 2.2 million people, with no difference between men and women. The prevalence of hearing disability tended to increase with aging, with significant differences for the age groups 40 to 59 years old (1.0%, 95% CI, 0.9-1.2); and 60 years old or older (5.2%, 95% CI, 4.7-5.7). A higher prevalence was also seen among individuals referring to be white skinned (1.4%, 95% CI: 1.2-1.5). A higher percentage (1.4%, 95% CI, 1.2-1.7) was seen in the South region against the other regions and the prevalence was lower in the North region (0.8%, 95% CI, 0.6-0.9) (Table 2).
Visual disability reached the highest prevalence among the investigated disabilities (3.6%, 95% CI, 3.4-3.9), approximately 7.2 million people, with no difference between men and women. Just like with the hearing disability and physical disability, visual disability also tended to increase with aging, with higher prevalence reported by the age groups 40 to 59 years old (5.1%, 95% CI, 4.7-5.6); and 60 years old or older (11.5%, 95% CI, 10.6-12.4). No differences due to color or race were seen. Regarding location, a higher prevalence was found in individuals living in rural setting (4.7%, 95% CI, 4.0-5.4). The prevalence was similar in each region, with exception of South region, which showed a higher percentage when compared to the other regions, with a significant difference (5.9%, 95% CI, 5.0-6.8) (Table 2).
The ratios of birth and acquired disabilities were also assessed by type of disability, for Brazil and each location. For intellectual disability, the percentage was higher for individuals who were born with such disability. However, a different behavior was seen for other disabilities, higher among those individuals who referred having acquired them. Particularly, a major difference was seen in visual disability, which presented a much higher prevalence in acquired disability regarding birth disabilities: approximately ten times higher (Figure 1).

Ratio of people with birth and acquired disabilities, as per type of disability and location in Brazil. NHS 2013.
Aiming at assessing the level of limitation of those referring some physical disability, the individuals were split into two groups: severe/very severe limitation and little/no limitation. For severe/very severe limitation, very high percentages were reported for intellectual (54.8%) and physical (46.8%) disabilities. Individuals with hearing and visual disability reported 20.6% of severe/very severe limitation and those with visual disability were who referred the least severe/very severe limitation when compared against other disabilities (16.0%) (Figure 2).

Ratio of people with a severe/very severe limitation and with little or no limitation, by type of disability and location. National Health Survey, 2013, Brazil
Regarding the use of rehabilitation services to deal with the referred disability, the percentages were higher among those referring intellectual disability and among those referring physical disability (higher among the residents of urban setting, for both cases) (Figure 3).
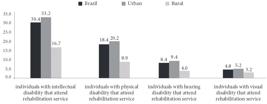
Ratio of people attending some kind of rehabilitation service, by type of disability and location. National Health Survey, 2013, Brazil.
Discussion
The study described the epidemiological distribution of the self-referred disability in Brazil and indicated prevalence of 6.2%, which corresponds to approximately 12.4 million people with intellectual, physical, hearing or visual disability. The prevalence increased with age, especially after 40 years old, and was higher in rural area and South region. The most common disability was visual, with prevalence of 3.6%; the other types were around 1%. The acquired disability was predominant – with exception of intellectual disability, most frequently reported by those who were born with it. The level of limitation intense/very intense was higher between those intellectual disabled (over half of it), followed by physical disability (less than a half), one fifth of the hearing disabled reported intense/very intense limitation and the lowest number of limitation reports was among the visual disabled (16.0%).
The Convention on the Rights of Persons with Disabilities highlights the importance of development to reduce the barriers, caused by attitudes and environment, that obstruct and limit the full and effective participation of the disabled people in the society, with equal opportunities1313. Instituto Brasileira de Geografia e Estatística (IBGE). Ciclos de Vida. Rio de Janeiro: IBGE; 2015.. NHS adds information on the subject, endorsing the commitment to creation of public policies that promote inclusion and the improvement of the quality of life of people with disabilities.
NHS opted to focus on the concept of self-referred disabilities, answered by the user him/herself or by their proxy or guardian. It suggests a trend to increased identification by the interviewees regarding permanent disabilities, which are possibly more associated to a greater impact on the activities of the daily living1111. Instituto Brasileira de Geografia e Estatística (IBGE). Acesso e Utilização dos Serviços de Saúde, Acidentes e Violências. Rio de Janeiro: IBGE; 2015.. Additionally, disabilities and incapacities that are more recognizable and apparent, identifiable by other people in general, are those moderate and severe, which are the most commonly identified, whether by the subject him/herself, whether by their proxy. Population studies (both self-reported and using proxy) establish that there may be a trend to underestimate the occurrence of disabilities, especially in their lightest forms, which may explain the variation of prevalence of occurrence of those problems in other studies.
Additionally, self-assessment or self-declaration is based on the subject’s perception of their own health and characterized as a subjective measurement. When such information is provided by a proxy, it is worth considering that subjectivity is also subject to the perception on the other person’s health1414. Goulart BNG, Martins-Reis VO, Chiari BM. Inquérito domiciliar de distúrbios fonoaudiológicos autodeclarados: desenho e protocolo de pesquisa. Audiol, Commun Res 2015; 20(4):336-348.. However, in case of disabilities, the level of handicap may interfere with the assessment of prevalence, but should not interfere significantly in the assessment of prevalence of global disability, except in the milder cases.
According to WHO, there are many variations in the prevalence of disabilities worldwide. That is because the approaches and data collection methods for the surveys also vary a lot22. World Health Organization (WHO). Disability and Rehabilitation: Future, Trends and Challenges in Rehabilitation. Geneva: WHO; 2002..
The census carried out by IBGE in 2010 registered an universe of 45.6 million people who reported having some kind of disability (23,9%); over 17.7 million of them (6.7% of population) used to present some disability considered “severe”1212. Brasil. Presidência da República. Decreto nº 5.296, de 2 de dezembro de 2004. Regulamenta as Leis nos 10.048, de 8 de novembro de 2000, que dá prioridade de atendimento às pessoas que especifica, e 10.098, de 19 de dezembro de 2000, que estabelece normas gerais e critérios básicos para a promoção da acessibilidade das pessoas portadoras de deficiência ou com mobilidade reduzida, e dá outras providências. Diário Oficial da União 2000; 3 dez.. NHS found a prevalence of 6.2% in 2013, which is close to the concept of severe disability considered by the census. The census data was based on other questions and concepts, including the theme of limitation of functionality, which may explain those differences1212. Brasil. Presidência da República. Decreto nº 5.296, de 2 de dezembro de 2004. Regulamenta as Leis nos 10.048, de 8 de novembro de 2000, que dá prioridade de atendimento às pessoas que especifica, e 10.098, de 19 de dezembro de 2000, que estabelece normas gerais e critérios básicos para a promoção da acessibilidade das pessoas portadoras de deficiência ou com mobilidade reduzida, e dá outras providências. Diário Oficial da União 2000; 3 dez.. NHS used legal bases in the Brazilian laws for its definitions and, in that sense, it became more specific. That may also explain the differences in prevalence found in both surveys1010. Szwarcwald CL, Malta DC, Pereira CA, Vieira MLFP, Conde WL, Souza Júnior PRB, Damacena GN, Azevedo LO, Azevedo e Silva G, Theme Filha MM, Lopes CS, Romero DE, Almeida WS, Monteiro CA. Pesquisa Nacional de Saúde no Brasil: concepção e metodologia de aplicação. Cien Saude Colet 2014; 19(2):333-342.. Comparisons between surveys are complex due to differences in methodology, sampling and survey data collection strategy. Additionally, it is critical to use the same questionnaire, order of questions, options of answers, skips, changes in calculation methods and indicators concepts1515. Barros MBA. Inquéritos domiciliares de saúde: potencialidades e desafios. Rev Bras Epidemiol [periódico na Internet] 2008 maio [acessado 2015 jan 5]; 11(Supl 1):6-19. Disponível em: http://www.scielo.br/pdf/rbepid/v11s1/01.pdf
http://www.scielo.br/pdf/rbepid/v11s1/01...
. Those differences may explain the difference between NHS and other inquiries.
NHS also addresses other questions regarding functionality in modules “Health of subjects who are 60 years old or older”, “Perception of health”, “Lifestyles” and “Chronic diseases”1111. Instituto Brasileira de Geografia e Estatística (IBGE). Acesso e Utilização dos Serviços de Saúde, Acidentes e Violências. Rio de Janeiro: IBGE; 2015.,1313. Instituto Brasileira de Geografia e Estatística (IBGE). Ciclos de Vida. Rio de Janeiro: IBGE; 2015.. The data help in creating a clearer picture regarding disability and functional limitation, indicating the impact of several functional challenges faced by Brazilian population. When these cases of functional limitation are added up to those obtained from self-reported disability, the results is close to what was identified by the 2010 census. In this study, we chose to present only the prevalence regarding the self-reported disabilities.
As per WHO’s Global Burden of Disease (2004), 15% of the worldwide population is estimated to present some kind of disability/limitation of functionality – higher than the estimation from the ‘70s, which was 10%1616. Santos S, Melo US, Lopes SSS, Weller M, Kok F. A Endogamia Explicaria a Elevada Prevalência de Deficiências em Populações do Nordeste Brasileiro? Cien Saude Colet 2012; 18(4):1141-1150.. The very same survey identified that Northeast would present higher prevalence, different from what was identified in NHS, which reported South region, specially a high prevalence of visual disability1616. Santos S, Melo US, Lopes SSS, Weller M, Kok F. A Endogamia Explicaria a Elevada Prevalência de Deficiências em Populações do Nordeste Brasileiro? Cien Saude Colet 2012; 18(4):1141-1150..
The increased disability with aging was identified in NHS and also by the census88. Instituto Brasileiro de Geografia e Estatística (IBGE). Censo Demográfico 2010. [acessado 2015 out 16]. Disponível em: http://censo2010.ibge.gov.br/
http://censo2010.ibge.gov.br/...
, and it may be justified by the acquired disabilities due to accidents and diseases, which are most frequently reported by the elderly. The most frequently reported are cardiovascular diseases, stroke and dementias, as well as diseases inherent to aging, such as presbycusis88. Instituto Brasileiro de Geografia e Estatística (IBGE). Censo Demográfico 2010. [acessado 2015 out 16]. Disponível em: http://censo2010.ibge.gov.br/
http://censo2010.ibge.gov.br/...
,1717. Malta DC, Moura LD, Prado RRD, Escalante JC, Schmidt MI, Duncan BB. Chronic non-communicable disease mortality in Brazil and its regions, 2000-2011. Epidemiologia e Serviços de Saúde 2014; 23(4):599-608.,1818. Schiller JS, Lucas JW, Peregoy JA. Summary health statistics for U.S. adults: National Health Interview Survey, 2011. National Center for Health Statistics. Vital Health Stat 10 2012; (252):1-218..
The prevalence of visual disability was higher than the other disabilities, which may be justified by the Brazilian national laws, that typifies disabled people different from the others, including as disabled poor vision in one or both eyes1212. Brasil. Presidência da República. Decreto nº 5.296, de 2 de dezembro de 2004. Regulamenta as Leis nos 10.048, de 8 de novembro de 2000, que dá prioridade de atendimento às pessoas que especifica, e 10.098, de 19 de dezembro de 2000, que estabelece normas gerais e critérios básicos para a promoção da acessibilidade das pessoas portadoras de deficiência ou com mobilidade reduzida, e dá outras providências. Diário Oficial da União 2000; 3 dez..
Cataract and glaucoma are the most frequently reported causes of severe visual disability1919. Campos B, Cerrate A, Montjoy E, Dulanto Gomero V, Gonzales C, Tecse A, Pariamachi A, Lansingh VC, Dulanto Reinoso V, Minaya Barba J, Silva JC, Limburg H. National survey on the prevalence and causes of blindness in Peru. Rev Panam Salud Publica 2014; 36(5):283-289.,2020. López M, Brea I, Yee R, Yi R, Carles V, Broce A, Limburg H, Silva JC. Survey on avoidable blindness and visual impairment in Panama. Rev Panam Salud Publica 2014; 36(6):355-360.. Uncorrected refractive errors cause moderate visual problems1919. Campos B, Cerrate A, Montjoy E, Dulanto Gomero V, Gonzales C, Tecse A, Pariamachi A, Lansingh VC, Dulanto Reinoso V, Minaya Barba J, Silva JC, Limburg H. National survey on the prevalence and causes of blindness in Peru. Rev Panam Salud Publica 2014; 36(5):283-289. and the affected population requires access to specialized services capable of timely diagnosing and treating those issues2121. Theou O, Brothers TD, Peña FG, Mitnitski A, Rockwood K. Identifying Common Characteristics of Frailty Across Seven Scales. J Am Geriat Soc 2014; 62(5):901-906..
With aging, there is a trend to show increased prevalence of co-occurrence of disabilities associated to other issues, and that aspect is named by international literature as “frailty”2121. Theou O, Brothers TD, Peña FG, Mitnitski A, Rockwood K. Identifying Common Characteristics of Frailty Across Seven Scales. J Am Geriat Soc 2014; 62(5):901-906..
The frequency of service usage was low. The highest use refers to services for the intellectual disabled, regarding the APAE network2222. Associação de Pais e Amigos dos Excepcionais (APAE). Sobre Deficiência Intelectual e as APAES. [acessado 2015 nov 07]. Disponível em: http://www.apaesp.org.br/SobreADeficienciaIntelectual/Paginas/O-que-e.aspx
http://www.apaesp.org.br/SobreADeficienc...
. The question used in this survey is aimed at understanding whether the user uses some kind of service. In that sense, its interpretation is to be weighed, as it may or may not be understood by hearing and physical disabled who obtained prosthesis, because they may not use services on an ongoing basis, since their needs were met regarding adaptation of orthosis and prosthesis. The concept of rehabilitation is to be considered a process with beginning, middle and end; thus, it may be a limit of the survey itself, requiring new questions, for each type of disability, in the next editions2323. Senna MCM, Lobato LVC, Andrade LD. Proteção Social à Pessoa com Deficiência no Brasil Pós-Constituinte. Revista SER Social 2013; 15(32):67-73.. On the other hand, it is necessary to recognize that the access to rehabilitation services is still scarce, even with extended availability. In 2011, the Brazilian federal government released the National Plan on the Rights of Persons with Disabilities – Living without Limitations2424. Brasil. Ministério da Saúde (MS). Política Nacional de Saúde da Pessoa Portadora de Deficiência. Brasília: MS; 2008.. The Plan relied on engagement of fifteen ministries and CONADE (Conselho Nacional da Pessoa com Deficiência, National Council for Persons with Disabilities) and aimed at shared actions between federal, state and municipal levels and creation of governmental policies in areas of access to education, social inclusion, accessibility and healthcare2424. Brasil. Ministério da Saúde (MS). Política Nacional de Saúde da Pessoa Portadora de Deficiência. Brasília: MS; 2008..
In Brazil, it was not until recently that the disabilities were acknowledged as human rights issue and a social justice subject. For several years, disability was dealt with exclusively as a personal tragedy and/or a body abnormality when compared against the “normal” body; the families and philanthropic institutions aimed at rehabilitation, education or confinement of disabled were exclusively responsible for those individuals. Any actions for the person with disability demand higher investments, such as more complex services, infrastructure, equipment and material, human resources of several areas, which are still scarce2323. Senna MCM, Lobato LVC, Andrade LD. Proteção Social à Pessoa com Deficiência no Brasil Pós-Constituinte. Revista SER Social 2013; 15(32):67-73..
Within limits, the replies are self-referred and may be subject to memory bias2525. Sen A. Health: perception versus observation : Self reported morbidity has severe limitations and can be extremely misleading. BMJ 2002; 324(7342):860-861.. Additionally, in case of disability, the proxy may be someone else, and the level of compromise of daily life activities may be perceived differently due to the level of subjectivity inherent to the event.
Conclusion
The data presented several aspects of disabilities in Brazil. These findings are useful to support the decision making when establishing specific actions for the target population. And, even though there were significant improvements in the past few years regarding public policies that aim at promoting integration of healthcare of people with disabilities, in line with what was recommended by NATO and WHO, the access available to promote, prevent, diagnose and early treat is still in need, as well as strengthening the specific public policies regarding health, education, social care, work and jobs.
Disabilities in Brazil affect over 12 million people, mostly men who are 60 years old or older. The use of health services resulting from those disabilities may have been underestimated by the respondents, but it is necessary a deeper survey in order to assess whether it is due to difficult access or whether the subjects did not identify the access to diagnosis and adaptation programs and use of orthosis and prosthesis as access to rehabilitation, and thus to public health services. NHS adds information on the theme, improving its commitment to creating public policies that promote inclusion and improve the quality of life of disabled people.
Referências
-
1World Health Organization (WHO). World report on disability. [acessado 2015 set 20]. Disponível em: http://www.larchetoronto.org/wordpress/wp-content/uploads/2012/01/launch-of-World-Report-on-Disability-Jan-27-121.pdf
» http://www.larchetoronto.org/wordpress/wp-content/uploads/2012/01/launch-of-World-Report-on-Disability-Jan-27-121.pdf -
2World Health Organization (WHO). Disability and Rehabilitation: Future, Trends and Challenges in Rehabilitation. Geneva: WHO; 2002.
-
3Brasil. Presidência da República. Decreto nº 3.298, de 20 de dezembro de 1999. Regulamenta a Lei no 7.853, de 24 de outubro de 1989, dispõe sobre a Política Nacional para a Integração da Pessoa Portadora de Deficiência, consolida as normas de proteção, e dá outras providências. Diário Oficial da União 1999; 21 dez.
-
4Brasil. Presidência da República. Lei nº 12.470, de 31 de agosto de 2011. Altera os arts. 21 e 24 da Lei no 8.212, de 24 de julho de 1991, que dispõe sobre o Plano de Custeio da Previdência Social, para estabelecer alíquota diferenciada de contribuição para o microempreendedor individual e do segurado facultativo sem renda própria que se dedique exclusivamente ao trabalho doméstico no âmbito de sua residência, desde que pertencente a família de baixa renda; altera os arts. 16, 72 e 77 da Lei no 8.213, de 24 de julho de 1991, que dispõe sobre o Plano de Benefícios da Previdência Social, para incluir o filho ou o irmão que tenha deficiência intelectual ou mental como dependente e determinar o pagamento do salário-maternidade devido à empregada do microempreendedor individual diretamente pela Previdência Social; altera os arts. 20 e 21 e acrescenta o art. 21-A à Lei no 8.742, de 7 de dezembro de 1993 - Lei Orgânica de Assistência Social, para alterar regras do benefício de prestação continuada da pessoa com deficiência; e acrescenta os §§ 4o e 5o ao art. 968 da Lei no 10.406, de 10 de janeiro de 2002 - Código Civil, para estabelecer trâmite especial e simplificado para o processo de abertura, registro, alteração e baixa do microempreendedor individual. Diário Oficial da União 2011; 1 set.
-
5Freita MNC. A Inserção de Pessoas com Deficiência em Empresas Brasileiras. Um Estudo sobre as Relações entre Concepções de Deficiência, Condições de Trabalho e Qualidade de Vida no Trabalho [tese]. Belo Horizonte: Universidade Federal de Minas Gerais; 2007.
-
6Farias N, Buchalla CMA. Classificação Internacional de Funcionalidade, Incapacidade e Saúde da Organização Mundial da Saúde: Conceitos, Usos e Perspectivas. Rev Bras Epidemiol 2005; 8(2):187-193.
-
7World Health Organization (WHO). Towards a Common Language for Functioning, Disability and Health – ICF. Genebra: WHO; 2002.
-
8Instituto Brasileiro de Geografia e Estatística (IBGE). Censo Demográfico 2010. [acessado 2015 out 16]. Disponível em: http://censo2010.ibge.gov.br/
» http://censo2010.ibge.gov.br/ -
9Brasil. Ministério da Saúde (MS). Cartilha do Censo 2010 – Pessoas com Deficiência Brasília: SDHPR/ SNPD; 2012.
-
10Szwarcwald CL, Malta DC, Pereira CA, Vieira MLFP, Conde WL, Souza Júnior PRB, Damacena GN, Azevedo LO, Azevedo e Silva G, Theme Filha MM, Lopes CS, Romero DE, Almeida WS, Monteiro CA. Pesquisa Nacional de Saúde no Brasil: concepção e metodologia de aplicação. Cien Saude Colet 2014; 19(2):333-342.
-
11Instituto Brasileira de Geografia e Estatística (IBGE). Acesso e Utilização dos Serviços de Saúde, Acidentes e Violências Rio de Janeiro: IBGE; 2015.
-
12Brasil. Presidência da República. Decreto nº 5.296, de 2 de dezembro de 2004. Regulamenta as Leis nos 10.048, de 8 de novembro de 2000, que dá prioridade de atendimento às pessoas que especifica, e 10.098, de 19 de dezembro de 2000, que estabelece normas gerais e critérios básicos para a promoção da acessibilidade das pessoas portadoras de deficiência ou com mobilidade reduzida, e dá outras providências. Diário Oficial da União 2000; 3 dez.
-
13Instituto Brasileira de Geografia e Estatística (IBGE). Ciclos de Vida Rio de Janeiro: IBGE; 2015.
-
14Goulart BNG, Martins-Reis VO, Chiari BM. Inquérito domiciliar de distúrbios fonoaudiológicos autodeclarados: desenho e protocolo de pesquisa. Audiol, Commun Res 2015; 20(4):336-348.
-
15Barros MBA. Inquéritos domiciliares de saúde: potencialidades e desafios. Rev Bras Epidemiol [periódico na Internet] 2008 maio [acessado 2015 jan 5]; 11(Supl 1):6-19. Disponível em: http://www.scielo.br/pdf/rbepid/v11s1/01.pdf
» http://www.scielo.br/pdf/rbepid/v11s1/01.pdf -
16Santos S, Melo US, Lopes SSS, Weller M, Kok F. A Endogamia Explicaria a Elevada Prevalência de Deficiências em Populações do Nordeste Brasileiro? Cien Saude Colet 2012; 18(4):1141-1150.
-
17Malta DC, Moura LD, Prado RRD, Escalante JC, Schmidt MI, Duncan BB. Chronic non-communicable disease mortality in Brazil and its regions, 2000-2011. Epidemiologia e Serviços de Saúde 2014; 23(4):599-608.
-
18Schiller JS, Lucas JW, Peregoy JA. Summary health statistics for U.S. adults: National Health Interview Survey, 2011. National Center for Health Statistics. Vital Health Stat 10 2012; (252):1-218.
-
19Campos B, Cerrate A, Montjoy E, Dulanto Gomero V, Gonzales C, Tecse A, Pariamachi A, Lansingh VC, Dulanto Reinoso V, Minaya Barba J, Silva JC, Limburg H. National survey on the prevalence and causes of blindness in Peru. Rev Panam Salud Publica 2014; 36(5):283-289.
-
20López M, Brea I, Yee R, Yi R, Carles V, Broce A, Limburg H, Silva JC. Survey on avoidable blindness and visual impairment in Panama. Rev Panam Salud Publica 2014; 36(6):355-360.
-
21Theou O, Brothers TD, Peña FG, Mitnitski A, Rockwood K. Identifying Common Characteristics of Frailty Across Seven Scales. J Am Geriat Soc 2014; 62(5):901-906.
-
22Associação de Pais e Amigos dos Excepcionais (APAE). Sobre Deficiência Intelectual e as APAES. [acessado 2015 nov 07]. Disponível em: http://www.apaesp.org.br/SobreADeficienciaIntelectual/Paginas/O-que-e.aspx
» http://www.apaesp.org.br/SobreADeficienciaIntelectual/Paginas/O-que-e.aspx -
23Senna MCM, Lobato LVC, Andrade LD. Proteção Social à Pessoa com Deficiência no Brasil Pós-Constituinte. Revista SER Social 2013; 15(32):67-73.
-
24Brasil. Ministério da Saúde (MS). Política Nacional de Saúde da Pessoa Portadora de Deficiência Brasília: MS; 2008.
-
25Sen A. Health: perception versus observation : Self reported morbidity has severe limitations and can be extremely misleading. BMJ 2002; 324(7342):860-861.
Publication Dates
-
Publication in this collection
Oct 2016
History
-
Received
17 Nov 2015 -
Reviewed
30 June 2016 -
Accepted
02 July 2016





