Abstracts
Secular trends in rates of low birth weight in Brazilian state capital cities were evaluated for the period 1996 to 2010 using joinpoint regression models. The rates were calculated using data from the Live Births Information System. Newborns weighing less than 500g were excluded. Only data for capital cities was included since under-registration of births in these cities is lower and new trends can be detected earlier. There was a significant increase in the rate of low birth weight in the Brazilian capitals of the North Region, Northeast Region, South Region and Southeast Region up to 2003/2004, stabilizing thereafter. In the capitals of the Center-west Region the rate increased throughout the whole study period. The rate of low birth weight was higher in the capitals of the more developed regions. The rate of multiple births increased significantly in all Brazilian capitals, while the stillbirth rate decreased and showed a negative correlation with the rate of low birth weight. The increase in the rate of low birth weight may be partially explained by the increase in multiple births, an increase in the birth of infants weighing 500 to 999g and by the reduction in the stillbirth rate.
Low Birth Neight Infant; Stillbirth; Multiple Birth Offspring
La tendencia secular de la tasa de bajo peso al nacer de 1996 a 2010 en las capitales brasileñas se evaluó utilizando modelos de regresión joinpoint. Las tasas se calcularon a partir del Sistema de Información sobre Nacidos Vivos, excluyéndose recién nacidos con un peso < 500g. Fueron incluidos solamente datos de las capitales, donde el sub-registro es menor y las nuevas tendencias pueden ser detectadas más precozmente. La tasa de bajo peso al nacer aumentó significantemente en las capitales brasileñas de las regiones Norte, Nordeste, Sur y Sudeste hasta 2003/2004, habiéndose estabilizado a partir de entonces. En las capitales de la Región Centro-oeste la tasa aumentó a lo largo de todo el período. La tasa de bajo peso al nacer fue mayor en las capitales de las regiones más desarrolladas. La tasa de partos múltiples aumentó significantemente en las capitales brasileñas. La tasa de natimortalidad disminuyó y presentó una correlación negativa con la tasa de bajo peso al nacer. Una parte del crecimiento en la tasa de bajo peso al nacer puede ser explicada por el aumento en la tasa de nacimientos múltiple, por el nacimiento de recién nacidos pesando de 500g a 999g y por la reducción de la tasa de natimortalidad.
Recién Nacido de Bajo Peso; Mortinato; Progenie de Nascimento Múltiple
A tendência secular da taxa de baixo peso ao nascer de 1996 a 2010 nas capitais brasileiras foi avaliada utilizando-se modelos de regressão joinpoint. As taxas foram calculadas a partir do Sistema de Informações sobre Nascidos Vivos, excluindo-se recém-nascido com peso < 500g. Foram incluídos apenas dados das capitais, onde o sub-registro é menor e novas tendências podem ser detectadas mais precocemente. A taxa de baixo peso ao nascer aumentou significantemente nas capitais brasileiras das regiões Norte, Nordeste, Sul e Sudeste até 2003/2004, tendo se estabilizado a partir de então. Nas capitais da Região Centro-oeste a taxa aumentou ao longo de todo o período. A taxa de baixo peso ao nascer foi maior nas capitais das regiões mais desenvolvidas. A taxa de partos múltiplos aumentou significantemente nas capitais brasileiras. A taxa de natimortalidade diminuiu e apresentou correlação negativa com a taxa de baixo peso ao nascer. Parte do aumento na taxa de baixo peso ao nascer pode ser explicado pelo aumento na taxa de nascimentos múltiplos e pelo nascimento de recém-nascido pesando de 500g a 999g e pela redução da taxa de natimortalidade.
Recém-Nascido de Baixo Peso; Natimorto; Prole de Múltiplos Nascimentos
ARTICLE ARTIGO
Secular trends in the rate of low birth weight in Brazilian State Capitals in the period 1996 to 2010
Tendência secular da taxa de baixo peso ao nascer nas capitais brasileiras de 1996 a 2010
Tendencia secular de la tasa de bajo peso al nacer en las capitales brasileñas de 1996 a 2010
Helma Jane Ferreira VelosoI; Antônio Augusto Moura da SilvaI; Marco Antônio BarbieriII; Marcelo Zubarán GoldaniIII; Fernando Lamy FilhoI; Vanda Maria Ferreira SimõesI; Rosângela Fernandes Lucena BatistaI; Maria Teresa S. S. Britto e AlvesI; Heloísa BettiolII
IDepartamento de Saúde Pública, Universidade Federal do Maranhão, São Luís, Brasil
IIFaculdade de Medicina de Ribeirão Preto, Universidade de São Paulo, Ribeirão Preto, Brasil
IIIDepartamento de Puericultura e Pediatria, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brasil
Correspondence Correspondence: H. J. F. Veloso Programa de Pós-graduação em Saúde Coletiva, Departamento de Saúde Pública, Universidade Federal do Maranhão. Rua Barão de Itapary 155, São Luís, MA 65020-070, Brasil. helma@oi.com.br
ABSTRACT
Secular trends in rates of low birth weight in Brazilian state capital cities were evaluated for the period 1996 to 2010 using joinpoint regression models. The rates were calculated using data from the Live Births Information System. Newborns weighing less than 500g were excluded. Only data for capital cities was included since under-registration of births in these cities is lower and new trends can be detected earlier. There was a significant increase in the rate of low birth weight in the Brazilian capitals of the North Region, Northeast Region, South Region and Southeast Region up to 2003/2004, stabilizing thereafter. In the capitals of the Center-west Region the rate increased throughout the whole study period. The rate of low birth weight was higher in the capitals of the more developed regions. The rate of multiple births increased significantly in all Brazilian capitals, while the stillbirth rate decreased and showed a negative correlation with the rate of low birth weight. The increase in the rate of low birth weight may be partially explained by the increase in multiple births, an increase in the birth of infants weighing 500 to 999g and by the reduction in the stillbirth rate.
Low Birth Neight Infant; Stillbirth; Multiple Birth Offspring
RESUMO
A tendência secular da taxa de baixo peso ao nascer de 1996 a 2010 nas capitais brasileiras foi avaliada utilizando-se modelos de regressão joinpoint. As taxas foram calculadas a partir do Sistema de Informações sobre Nascidos Vivos, excluindo-se recém-nascido com peso < 500g. Foram incluídos apenas dados das capitais, onde o sub-registro é menor e novas tendências podem ser detectadas mais precocemente. A taxa de baixo peso ao nascer aumentou significantemente nas capitais brasileiras das regiões Norte, Nordeste, Sul e Sudeste até 2003/2004, tendo se estabilizado a partir de então. Nas capitais da Região Centro-oeste a taxa aumentou ao longo de todo o período. A taxa de baixo peso ao nascer foi maior nas capitais das regiões mais desenvolvidas. A taxa de partos múltiplos aumentou significantemente nas capitais brasileiras. A taxa de natimortalidade diminuiu e apresentou correlação negativa com a taxa de baixo peso ao nascer. Parte do aumento na taxa de baixo peso ao nascer pode ser explicado pelo aumento na taxa de nascimentos múltiplos e pelo nascimento de recém-nascido pesando de 500g a 999g e pela redução da taxa de natimortalidade.
Recém-Nascido de Baixo Peso; Natimorto; Prole de Múltiplos Nascimentos
RESUMEN
La tendencia secular de la tasa de bajo peso al nacer de 1996 a 2010 en las capitales brasileñas se evaluó utilizando modelos de regresión joinpoint. Las tasas se calcularon a partir del Sistema de Información sobre Nacidos Vivos, excluyéndose recién nacidos con un peso < 500g. Fueron incluidos solamente datos de las capitales, donde el sub-registro es menor y las nuevas tendencias pueden ser detectadas más precozmente. La tasa de bajo peso al nacer aumentó significantemente en las capitales brasileñas de las regiones Norte, Nordeste, Sur y Sudeste hasta 2003/2004, habiéndose estabilizado a partir de entonces. En las capitales de la Región Centro-oeste la tasa aumentó a lo largo de todo el período. La tasa de bajo peso al nacer fue mayor en las capitales de las regiones más desarrolladas. La tasa de partos múltiples aumentó significantemente en las capitales brasileñas. La tasa de natimortalidad disminuyó y presentó una correlación negativa con la tasa de bajo peso al nacer. Una parte del crecimiento en la tasa de bajo peso al nacer puede ser explicada por el aumento en la tasa de nacimientos múltiple, por el nacimiento de recién nacidos pesando de 500g a 999g y por la reducción de la tasa de natimortalidad.
Recién Nacido de Bajo Peso; Mortinato; Progenie de Nascimento Múltiple
Introduction
In addition to being considered the most important factor affecting neonatal mortality, low birth weight is associated with a higher risk of infant mortality 1. Low birth weight, defined as less than 2,500g 2, is considered to be a risk factor for non-communicable diseases and injuries (NCDI) and learning difficulties 3,4,5,6,7.
Although the etiology of low birth weight is complex 1,7, its major determinants are preterm birth and intrauterine growth restriction (IUGR). The rate of low birth weight rate is high in developing countries compared to developed countries 8. According to global estimates, 15% of all babies are born with low birth weight; between 2005 and 2009 rates were 8% in Latin America and Caribbean, 15% in developing countries and 16% in the least developed countries 9.
Rates of low birth weight started to increase in the 1980s in the United States 10 and in the 1970s in Japan 11. The increase in the rate of low birth weight observed in the United States since the 1980s has been attributed to the increased rate of preterm and multiple births. However, an increase in the rate of low birth weight has also been described in Finland and France, where a reduction in preterm birth rates was observed. The rate of low birth weight increased from 4% in 1991 to 4.4% in 1998 in Finland 12 and from 3.8% in 1988 to 6.3% in 1998 in France, indicating that other factors, in addition to prematurity, are contributing to the increase in the rate of low birth weight in developed nations 13.
Brazil has experienced an insignificant increase in the rate of low birth weight from 7.9% in 1995 to 8.2% in 2007. After decreasing between 1995 and 2000 and later increasing up to 2003, rates have remained practically constant. However, trends have varied between the different regions of Brazil, with a significant increase in the rate in the North Region between 1999 and 2006, and in the South and Center-west Regions between 1995 and 2007, reflecting the fact that Brazilian regions seem to be at different stages of epidemiological perinatal transition since rates have stabilized in some regions but continue to increase in others 14.
In Brazil, the rate of low birth weight is higher in more developed cities 15. However, it would be expected that areas of higher socioeconomic level would show a lower incidence of low birth weight and this paradox is yet to be explained. While the explanation that this phenomenon is due to the under-registration of liveborns in less developed regions has been contested 16, high rates of maternal smoking and multiple births and the use of assisted reproductive technologies in more developed regions have been associated with this paradox 17,18.
Another factor to consider when explaining the increase in the rate of low birth weight is the change in concept of fetal viability. Today, very low birth weight babies, who would have been recorded in the past as stillborn or as a spontaneous abortion, are being recorded as low birth weight liveborns 19.
The objective of the present study was to analyze secular trends in rates of low birth weight, multiple births and stillbirths in capital cities in Brazil with low rates of under-registration of births to allow early identification of new trends. We also determined changes in rates of low birth weight excluding birth weights of less than 1,000 g and multiple births.
Methods
A cross-sectional study was carried out based on the analysis of secular trends, analyzing data from all state capital cities and by groups of regions.
Brazil consists of 27 states and the Federal District that are divided into five regions. In terms of socioeconomic development, the South and Southeast Regions are the most developed, the North and Northeast Regions are the least developed, while the Center-west Region is situated between these two poles. The regional rate of low birth weight was calculated by aggregating data from the capitals of each region.
The rates of low birth weight and multiple deliveries between 1996 and 2010 were calculated using data derived from the state-run Live Births Information System (SINASC, acronym in Portuguese) which had an estimated national coverage in 2005 of 92.1%. Coverage rates were lower in less developed regions (85.2% in the Northeast) and higher in the most developed regions (99.3% in the South) 14. Newborns weighing less than 500g were excluded. The crude rate of low birth weight was calculated by dividing the total number of newborns with a birth weight of 500g to 2,499g by the total number of liveborns weighing more than 500g multiplied by 100. The rate of low birth weight was also calculated in two different ways: (1) by excluding multiple births and newborns weighing less than 1,000g and calculating multiple births rate by dividing the total number of multiple births by the total number of births and multiplying the result by 100. Data from the year 1996 was excluded from the analysis of the multiple births rate due to a high frequency of missing values regarding the variable number of fetuses in the municipality of São Paulo. To evaluate the percentage contribution of each low birth weight group to the overall low birth weight rate the latter was subdivided into five categories: less than 500g, 500 to 999g, 1,000 to 1,499g, 1,500 to 1,999g, and 2,000 to 2,499g; (2) the number of stillborns was obtained from the Mortality Information System (Sistema de Informação sobre Mortalidade, acronym SIM in Portuguese). The stillbirth rate was calculated by dividing the number of stillborns by the sum of liveborns plus stillborns and multiplying by 1,000.
The trends in low birth weight, multiple birth and stillbirth rates were evaluated using joinpoint regression models based on the software developed by the National Cancer Institute of the United States. This method is used for modeling temporal changes in rates of low birth weight using an algorithm that tests whether a multisegmented line is significantly better than a straight line or a line with fewer segments. Joinpoint regression analysis joins a series of straight lines on a logarithmic scale in order to detect the trend of the annual rate. Each joinpoint denotes a statistically significant change in the trend. Statistical significance was tested using the Monte Carlo permutation procedure, which chooses the best segment for each model 20. The historical series studied covers a relatively short period of 15 years, leading to a higher probability of detecting a non-significant trend in the annual percent change. Therefore, a maximum of two joinpoints were permitted in order to increase the power to detect the statistical significance of variations in trends. The significance of the annual percent change in the rate of low birth weight was evaluated using a level of significance of 0.05.
Spearman's rank correlation coefficient was also calculated for rate of low birth weight and stillbirth rate for the Brazilian capitals for the period 1996 to 2010. Differences between proportions were assessed with the chi-squared test.
Results
The rate of low birth weight increased from 8.5% in 1996 to 9.1% in 2010 in all Brazilian capitals (p less than 0.001) with a general increase up to 2003/2004, followed by a stabilization of rates from 2003/2004 to 2010. Throughout the entire period, the rates of low birth weight were higher in capitals of the more developed regions (South and Southeast) and lower in those of the less developed regions (North, Northeast and Center-west) (Figure 1).
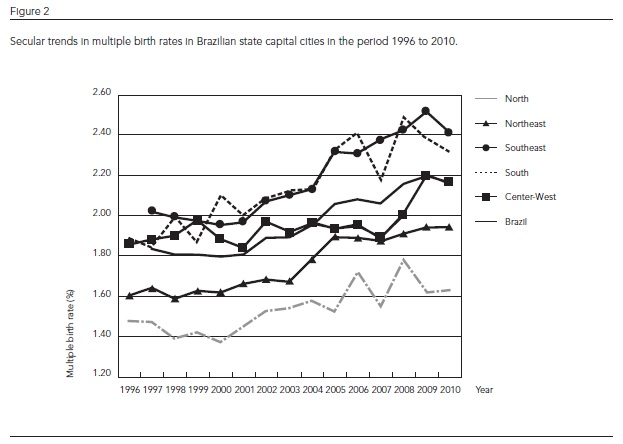
The rate of multiple births increased from 1.84% in 1997 to 2.15% in 2010 in the Brazilian capitals (p < 0.001). Again, the rates of multiple births were higher in capitals of the more developed regions (South and Southeast) and lower in capitals in the less developed regions (North, Northeast and Center-west) (Figure 2).
The stillbirth rate decreased from 14.1 per thousand in 1996 to 9.3 per thousand in 2010 in all Brazilian capitals (p < 0.001), and was higher in capitals of less developed regions and lower in capitals of the more developed regions (Figure 3).
The results of the joinpoint regression models show that the rate of low birth weight increased significantly in capitals of the Center-west region (0.87% per year) throughout the study period. From the beginning of the series to 2003 or 2004, the rate increased significantly by 1.97% per year in the capitals of the North Region, 1.22% per year in the capitals of the Northeast Region, 0.99% per year in the capitals of the Southeast Region, 1.8% per year in the capitals of the South Region, and 1.19% in all Brazilian capitals. After 2003/2004, the rate stabilized in all regions except the Center-west (Table 1).
From the beginning of the series to 2003 and 2004, even after the exclusion of multiple births, the rate of low birth weight continued to show a lower though still statistically significant increase in all Brazilian capitals except those of the Center-west Region, which showed a significant increase of 0.72% per year from 1996 to 2010. Starting in 2003/2004, the rate tended to stabilize in all capitals except those of the Center-west Region (Table 1).
With the exclusion of newborns weighing less than 1,000g, the rate of low birth weight showed a lower though statistically significant increase from 1996/1997 to 2003/2004 in all Brazilian capitals (0.98% per year), in the capitals of the North Region (1.71% per year), Northeast Region (0.9% per year), South Region (1.64% per year) and Southeast Region (0.83% per year). In capitals of the Center-west Region, this tendency towards an increase (0.74% per year) continued throughout the series (Table 1).
When multiple births and newborns weighing less than 1,000g were simultaneously excluded the increase in rate of low birth weight gradually lost intensity though maintaining statistical significance from the beginning of the series to 2003/2004 in all Brazilian capitals , except those in the North Region and Center-west Region, where a gradual loss of intensity of the increase was observed until the end of the series. A statistically significant reduction in rates was observed only in the capitals of the Southeast Region, with a value of -0.7% for the period 2003 to 2010 (Table 1).
For the period 1996 to 2010, the multiple births rate increased significantly in the capitals of the North Region (1.34% per year) and South Region (1.97% per year). In all Brazilian capitals and in the capitals of the Northeast and Southeast the increase in rates started later in 2000 through to 2010 (2.12%, 2.05% and 2.6% per year, respectively). During a more recent period (2007 to 2010) there was a significant increase in the multiple births rate (4.45% per year) in the capitals of the Center-west Region (Table 2).
The tendency towards a reduction in the rate of stillbirths was significant for all Brazilian capitals (-2.63% per year) and for capitals of the North Region (-2.68% per year), Northeast Region (-1.17% per year), South Region (-3.83% per year) and Center-west Region (-2.13% per year). For the capitals of the Southeast Region there was a-4.56% per year fall in the rate for the period 1995 to 2005. After 2005, the stillbirth rate in this region stabilized and therefore the fall was no longer significant (Table 2).
The correlation between rate of low birth weight and stillbirth rate in all Brazilian capitals was negative (-0.72) and statistically significant (p = 0.003).
While there was a reduction in the total number of low birth weight newborns in all Brazilian capitals and in the capitals of the Southeast Region, Northeast Region and South Region, an increase was detected in the capitals of the North Region and Center-west Region. The percentage of extremely low birth weight liveborns (less than 1,000g) within the total number of low birth weight newborns increased in all Brazilian capitals (from 4.64% in 1996 to 6.75% in 2010) (p less than 0.001). An increase in the percentage of newborns weighing 1,000 to 1,499g and 1,500 to 1,999g was also observed, compared to newborns weighing 2,000 to 2,499 g (p < 0.001) (Table 3).
Discussion
During the first years of the series, the rate of low birth weight increased in all Brazilian capital cities and continued to rise throughout the whole study period in the capitals of the Center-west Region. The rate tended to stabilize in the most recent years in all Brazilian capitals, except in the Center-west Region. The increase in rates was less intense when multiple deliveries and newborns weighing less than 1,000g were excluded, but remained significant. Throughout the whole period, the rate of low birth weight was higher in the capitals of the more developed regions and lower in capitals of the less developed regions. The multiple birth rate increased significantly in all Brazilian capitals, with regional variations. There was a significant reduction in the stillbirth rate in all Brazilian capitals, which showed a negative correlation with the rate of low birth weight.
The increase in rate of low birth weight observed at the beginning of the series seems to be paradoxical in view of the improved conditions of maternal and child health and the increased access to health services that occurred during that period. In the city of Pelotas, Southern Brazil, mean birth weight reduced by 47g between 1982 and 2004, while the prevalence of IUGR remained stable, indicating that most occurrences of lower birth weights were due to shorter gestations. This deduction was confirmed by the observation of a marked increase in the preterm birth rate during the period. The authors believe that the increase in preterm birth rate may have been a consequence of two factors: increased maternal risk factors for preterm delivery or increased medical intervention to interrupt high-risk pregnancies 21. This study shows that the increase in the rate of low birth weight diminished with the exclusion of newborns weighing less than 1,000g, indicating that at least part of the increase in the rate of low birth weight can be explained by the increase in preterm births, since all infants it this weight range were preterm.
The increase in the rate of low birth weight may also be due to changes in concepts of fetal viability. Studies have shown that the reduction of stillbirths associated with an increase in obstetrical interventions contributes to the increase in the rate of low birth weight since very small babies (less than 1,000g) who used to be considered unviable have started to be recorded as liveborns instead of stillbirths. In the United States, 86% of newborns weighing 501-1,500g and 55% of those weighing 501-750g survive 22. In Brazil, the neonatal mortality rate of very low birth weight newborns is 26 per thousand 23. This advance in medicine, through changes in the concept of fetal viability tends to reduce the number of fetal deaths, with a consequent reduction of birth weight 10,24,25,26. The increased percentage of newborns weighing less than 2,000g among low birth weight babies observed in the present study suggests that this phenomenon is also occurring in Brazilian capitals. During the study period, the increase in the rate of low birth weight was concomitant with the reduction of the stillbirth rate, with a statistically significant negative correlation between these rates. This suggests that part of the increase in low birth weight rate at the beginning of the historical series may be attributed to a reduction in the stillbirth rate. It is possible that increased medical interventions initially provoke a paradoxical increase in low birth weight rate. It is possible however that this increase in the rate of low birth weight may be a reflection of a reduction in the stillbirth rate as opposed to a worsening of health status.. A statistically significant reduction in the rate of low birth weight was observed together with a stabilization of the fall in the stillbirth rate during the most recent period of the time series in capitals of the Southeast Region after the exclusion of birth weight of less than 1,000g and multiple births. It is possible that in this region, where there was considerable reduction in the stillbirths rate, that the increase in low birth weight is partially attributable to the reduction of stillbirths. This suggests that medical intervention in more recent years is succeeding in reducing stillbirths and low birth weight at the same time.
The percentage of very low birth weight liveborns (less than 1,500g) is increasing. Studies have shown that, concomitantly with this increase, these babies are surviving for a longer period of time due to improved prenatal and childbirth care, new technologies and improved knowledge in all aspects of perinatal medicine 27,28,29,30. Ethical questions have been raised in some cases regarding the limit of viability and the polemic issue of emotional disorder and distress that intervention may provoke in families who must take care of children with serious neurological and sensory sequelae 31.
It is possible that the stabilization of rates of low birth weight that started in 2003/2004 were due to changes in concepts regarding fetal viability, since this trend was less pronounced when newborns with a birth weight of 500-1,000g were excluded. A study of secular trends in low birth weight conducted in the city of São Paulo showed little change in the rate of low birth weight in the period 1976 to 1998 32. Another more recent study in the same city confirmed this tendency towards stabilization of the rate of low birth weight in 2002/2003, when the rate was 9.4% 33. In Campinas, one of the more developed cities in the State of São Paulo, no changes in birth weight were observed in the period 1975 to 1996, with low birth weight remaining at around 9% 34. In Rio de Janeiro, the rate of low birth weight, which was 9.5% in 1994, remained at 9.1% in 2000 35.
There was a significant increase in multiple births across all Brazilian capitals. This may have partially contributed to the increase in the rate of low birth weight since the trend towards an increase in the rate was less pronounced when multiple births were excluded. A study conducted in Porto Alegre observed that the increase in the rate of multiple births contributed to the increase in the rate of low birth weight, explaining 23.9% of the increase in rate from 1994 to 2005 17. There has been a significant global increase in multiple pregnancies, especially in developed countries, due to the diffusion of assisted reproductive technologies 36. In the United States, in the period 1997 to 2000, the proportion of multiple births attributable to assisted reproductive technologies increased from 11.2% to 13.6% 37. In Brazil, in the period 1984 to 2003, the total number of births increased by 9.5%, while the number of triplet births and other higher order births increased five-fold 38. A possible explanation includes the increase in the use of assisted reproductive technologies and older maternal age 39. Among twin births, 50% of newborns are born with low weight and in triplet pregnancies, 90% of newborns present IUGR 36. Assisted reproductive technologies are related to a higher occurrence of preterm births, IUGR and multiple pregnancies, which are considered to be risk factors for low birth weight 40,41.
The results of the present study demonstrate the low birth weight paradox where more developed regions continue to present the highest rates of low birth weight. A partial explanation for these findings is based on a higher rate of very low birth weight and multiple births in capitals of the most developed regions.
Important strong points of this study include the representativeness of the sample, which included all Brazilian capital cities and the use of joinpoint regression, which allowed the identification of variations in the distribution of annual percentage change with high degree of sensitivity. We opted to analyze only the capital cities, where changes tend to occur first. The capitals are more urbanized and developed and therefore under-registration of deaths and births is low.
A limitation of this study was the exclusion of 1996 data on the municipality of São Paulo and of data on the Southeast Region and all Brazil in the analysis of multiple births. This exclusion was necessary in view of the large number of missing data regarding the variable number of fetuses in the municipality of São Paulo. The lack of information about assisted or natural reproduction was another limitation.
Even after the removal of multiple deliveries and newborns weighing less than 1,000g, the increase in the rate of low birth weight continued to be significant, indicating that other variables not included in this analysis, such as preterm birth or maternal age, may also have contributed to this increase. Individual level variables available in the SINASC were not used since the information on this database is a result of an ecological analysis. It was not possible to study trends in preterm birth rates because these rates calculated from the SINASC are underestimated in some Brazilian settings 42,43.
Conclusions
The rate of low birth weight increased in the capitals in all regions of Brazil in the first years of the series and throughout the study period in the capitals of some regions. In the capitals of all regions, except the Center-west, rates showed a tendency towards stabilization in recent years. Part of the increase in the rate of low birth weight may be explained by the increase in multiple births, the increase in the birth of infants weighing 500 to 999g and by the reduction in the stillbirth rate.
Contributors
H. J. F. Veloso and A. A. M. Silva contributed to project conception, data analysis and interpretation and writing this paper. M. A. Barbieri, M. Z. Goldani, F. Lamy Filho, V. M. F. Simões, R. Fernandes, L. Batista, M. T. S. S. B. Alves and H. Bettiol performed a relevant critical review of the intellectual content and analyzed the article for final approval of this article.
Recebido em 30/Mai/2012
Versão final reapresentada em 16/Ago/2012
Aprovado em 30/Ago/2012
- 1. Kramer MS. Determinants of low birth weight: methodological assessment and meta-analysis. Bull World Health Organ 1987; 65:663-737.
-
2Organização Mundial da Saúde. Classificação estatística internacional de doenças e problemas relacionados à saúde, 10a revisão. São Paulo: Edusp; 1998.
- 3. Barker DJ, Winter PD, Osmond C, Margetts B, Simmonds SJ. Weight in infancy and death from ischaemic heart disease. Lancet 1989; 2:577-80.
- 4. Almond D, Chay KY, Lee DS. Does birth weight matter? Evidence from the U.S. Population of Twin Births. Berkeley: University of California; 2002.
- 5. Barker DJ, Gluckman PD, Godfrey KM, Harding JE, Owens JA, Robinson JS. Fetal nutrition and cardiovascular disease in adult life. Lancet 1993; 341:938-41.
- 6. Barker DJ, Osmond C. Infant mortality, childhood nutrition, and ischaemic heart disease in England and Wales. Lancet 1986; 1:1077-81.
- 7. Ohlsson A, Shah P. Determinants and prevention of low birth weight: a synopsis of the evidence. Alberta: Institute of Health Economics; 2008.
- 8. United Nations Children's Fund. The state of the World's Children 2009. New York: United Nations Children's Fund; 2009.
- 9. United Nations Children's Fund. The state of the World's Children 2011. New York: United Nations Children's Fund; 2011.
- 10. Branum AM, Schoendorf KC. Changing patterns of low birthweight and preterm birth in the United States, 1981-98. Paediatr Perinat Epidemiol 2002; 16:8-15.
- 11. Ohmi H, Hirooka K, Hata A, Mochizuki Y. Recent trend of increase in proportion of low birthweight infants in Japan. Int J Epidemiol 2001; 30:1269-71.
- 12. Koskinen R, Merilainen J, Gissler M, Virtanen M. Finnish perinatal statistics 1997-1998. Helsinki: National Research and Development Center for Welfare and Health; 1999. (Statistical Report, 41).
- 13. Papiernik E, Goffinet F. Prevention of preterm births, the French experience. Clin Obstet Gynecol 2004; 47:755-67.
- 14. Silva AAM, Silva LM, Barbieri MA, Bettiol H, Carvalho LM, Ribeiro VS, et al. The epidemiologic paradox of low birth weight in Brazil. Rev Saúde Pública 2010; 44:767-75.
- 15. Silva AAM, Bettiol H, Barbieri MA, Brito LG, Pereira MM, Aragão VM, et al. Which factors could explain the low birth weight paradox? Rev Saúde Pública 2006; 40:648-55.
- 16. Silva AAM, Bettiol H, Barbieri MA, Pereira MM, Brito LG, Ribeiro VS, et al. Why are the low birthweight rates in Brazil higher in richer than in poorer municipalities? Exploring the epidemiological paradox of low birthweight. Paediatr Perinat Epidemiol 2005; 19:43-9.
- 17. Homrich-da-Silva C, Goldani MZ, Moura Silva AA, Agranonik M, Bettiol H, Barbieri MA, et al. The rise of multiple births in Brazil. Acta Paediatr 2008; 97:1019-23.
- 18. Horta BL, Barros FC, Halpern R, Victora CG. Baixo peso ao nascer em duas coortes de base populacional no Sul do Brasil. Cad Saúde Pública 1996; 12:27-31.
- 19. Phelan ST, Goldenberg R, Alexander G, Cliver SP. Perinatal mortality and its relationship to the reporting of low-birthweight infants. Am J Public Health 1998; 88:1236-9.
- 20. National Cancer Institute. Joinpoint regression program, version 3.3. Rockfield: National Cancer Institute; 2009.
- 21. Barros FC, Victora CG, Barros AJ, Santos IS, Albernaz E, Matijasevich A, et al. The challenge of reducing neonatal mortality in middle-income countries: findings from three Brazilian birth cohorts in 1982, 1993, and 2004. Lancet 2005; 365:847-54.
- 22. Fanaroff AA, Hack M, Walsh MC. The NICHD neonatal research network: changes in practice and outcomes during the first 15 years. Semin Perinatol 2003; 27:281-7.
- 23. Duarte JLMB, Mendonça GAS. Fatores associados à morte neonatal em recém-nascidos de muito baixo peso em quatro maternidades no Município do Rio de Janeiro, Brasil. Cad Saúde Pública 2005; 21:181-91.
- 24. Power C. National trends in birth weight: implications for future adult disease. BMJ 1994; 308:1270-1.
- 25. Skjaerven R, Gjessing HK, Bakketeig LS. Birthweight by gestational age in Norway. Acta Obstet Gynecol Scand 2000; 79:440-9.
- 26. Joseph KS, Kramer MS. Recent versus historical trends in preterm birth in Canada. CMAJ 1999; 161:1409.
- 27. Ravelli AC, Tromp M, van Huis M, Steegers EA, Tamminga P, Eskes M, et al. Decreasing perinatal mortality in The Netherlands, 2000-2006: a record linkage study. J Epidemiol Community Health 2009; 63:761-5.
- 28. Draper ES, Zeitlin J, Fenton AC, Weber T, Gerrits J, Martens G, et al. Investigating the variations in survival rates for very preterm infants in 10 European regions: the MOSAIC birth cohort. Arch Dis Child Fetal Neonatal Ed 2009; 94:F158-63.
- 29. Murphy BP, Armstrong K, Ryan CA, Jenkins JG. Benchmarking care for very low birthweight infants in Ireland and Northern Ireland. Arch Dis Child Fetal Neonatal Ed 2010; 95:F30-5.
- 30. Silva CH, Agranonik M, Silva AA, Bettiol H, Barbieri MA, Goldani MZ. Secular trend of very low birth weight rate in Porto Alegre, Southern Brazil. J Biosoc Sci 2010; 42:243-53.
- 31. Méio MDBB, Lopes CS, Morsch DS. Fatores prognósticos para o desenvolvimento cognitivo de prematuros de muito baixo peso. Rev Saúde Pública 2003; 37:311-8.
- 32. Monteiro CA, Benício MHD'A, Ortiz LP. Tendência secular do peso ao nascer na cidade de São Paulo (1976-1998). Rev Saúde Pública 2000; 34:26-40.
- 33. Minuci EG, Almeida MF. Diferenciais intra-urbanos de peso ao nascer no município de São Paulo. Rev Saúde Pública 2009; 43:256-66.
- 34. Mariotoni GG, Barros Filho AA. Peso ao nascer e mortalidade hospitalar entre nascidos vivos, 1975-1996. Rev Saúde Pública 2000; 34:71-6.
- 35. Gomes MASM, Lopes JMA, Moreira MEL, Gianini NOM. Assistência e mortalidade neonatal no setor público do Município do Rio de Janeiro, Brasil: uma análise do período 1994/2000. Cad Saúde Pública 2005; 21:1269-77.
-
36Centers for Disease Control and Prevention; American Society for Reproductive Medicine; Society for Assisted Reproductive Technology. 2007 Assisted reproductive technology success rates: national summary and fertility clinic reports. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2009.
- 37. Reynolds MA, Schieve LA, Martin JA, Jeng G, Macaluso M. Trends in multiple births conceived using assisted reproductive technology, United States, 1997-2000. Pediatrics 2003; 111:1159-62.
- 38. Freitas M, Siqueira AA, Segre CAM. Avanços em reprodução assistida. Rev Bras Crescimento Desenvolv Hum 2008; 18:93-7.
- 39. Colletto GM, Segre CA, Rielli ST, Rosário H. Multiple birth rates according to different socioeconomic levels: an analysis of four hospitals from the city of São Paulo, Brazil. Twin Res 2003; 6:177-82.
- 40. Olivennes F, Kerbrat V, Rufat P, Blanchet V, Fanchin R, Frydman R. Follow-up of a cohort of 422 children aged 6 to 13 years conceived by in vitro fertilization. Fertil Steril 1997; 67:284-9.
- 41. Doyle P. The outcome of multiple pregnancy. Hum Reprod 1996; 11:110-7.
- 42. Silva AA, Ribeiro VS, Borba Jr. AF, Coimbra LC, Silva RA. Avaliação da qualidade dos dados do sistema de informações sobre nascidos vivos em 1997-1998. Rev Saúde Pública 2001; 35:508-14.
- 43. Silveira MF, Santos IS, Barros AJ, Matijasevich A, Barros FC, Victora CG. Increase in preterm births in Brazil: review of population-based studies. Rev Saúde Pública 2008; 42:957-64.
Correspondence:
Publication Dates
-
Publication in this collection
29 Jan 2013 -
Date of issue
Jan 2013
History
-
Received
30 May 2012 -
Accepted
30 Aug 2012 -
Reviewed
16 Aug 2012