Abstract
Introduction
Rhabdomyoma is a rare benign tumor derived from skeletal muscles. Laryngeal rhabdomyomas are even rarer, with only approximately 40 reported cases in world literature. Laryngeal rhabdomyomas usually are seen as masses covered by mucosa. They are often solitary asymptomatic tumors, but symptoms such as hoarseness can occur. The radiologic features are usually those typical of benign neoplasms, showing well-delineated borders. The differential diagnoses for laryngeal masses include cysts, laryngoceles, and benign and malignant neoplasms. The diagnosis is usually made using histopathologic findings, but in some cases some difficulties can be found. Immunohistochemical staining is of great value in the differentiation of similar tumors. Treatment of rhabdomyoma is surgical excision.
Objective
To describe a case of rhabdomyoma of the larynx attended at Santa Casa de Misericórdia do Rio de Janeiro.
Case Report
A 35-year-old man presented with progressive hoarseness in the preceding year. Laryngoscopy showed a large submucosal tumor at the supraglottic region of the larynx. The neck computed tomography scan confirmed the submucosal mass, with distinct borders. The patient was taken to the operating suite, where endoscopic extirpation of the mass was performed. Initial histologic diagnosis was suggestive of paraganglioma, which was not confirmed by studies with immunohistochemical markers, and diagnosis was changed to adult-type rhabdomyoma. The patient recovered well. His voice returned to normal after 3 months.
Discussion
Although muscle tumors of the larynx are very rare, rhabdomyoma should be considered when there is a submucosal mass in the larynx.
Keywords
immunohistochemistry; laryngeal neoplasms; rhabdomyoma
Introduction
Rhabdomyomas (RMs) are rare lesions of striated muscle origin that can be found in cardiac and in extracardiac locations. The latter can be divided into two distinct categories: adult and fetal. Of these two, in the head and neck, the adult type is more common. Laryngeal RMs are extremely rare, with only ∼40 cases being reported worldwide.11 Farboud A, Pratap R, Helquist H, Montgomery P. An unusual cause of obstructive sleep apnoea. J Laryngol Otol 2009;123:e22 Adult-type RMs show an absolutely benign behavior and never metastasize.22 Hamper K, Renninghoff J, Schäfer H. Rhabdomyoma of the larynx recurring after 12 years: immunocytochemistry and differential diagnosis. Arch Otorhinolaryngol 1989;246:222-226 The treatment is excision. Recurrences are rare.
Review of Literature with Differential Diagnosis
Two forms of RM exist: cardiac and extracardiac. Extracardiac RMs represent true rare neoplasms that contain muscle elements. Histologically, these tumors are subcategorized into adult and fetal forms according to their degree of cellular differentiation and maturity. Adult-type tumors are confined to the head and neck region and usually originate from musculature of the pharynx, oral cavity, or less commonly the larynx. RM occurs more frequently in men than women (4:1). The reported ages of affected patients have ranged from 16 to 76 years.33 Jensen K, Swartz K. A rare case of rhabdomyoma of the larynx causing airway obstruction. Ear Nose Throat J 2006;85:116-118 Most reported cases of extracardiac RM have involved solitary masses. Approximately 3 to 10% of adult RMs may be multiple.44 Zacharia TT, Som PM. Multiple adult rhabdomyomas of the oropharynx, base of the tongue, and floor of themouth:magnetic resonance findings. Arch Otolaryngol Head Neck Surg 2008;134:892-894 RM virtually has no malignant potential.
RMs of the larynx usually appear as mucosal covered masses that vary in size. They frequently are asymptomatic solitary lesions but progressive hoarseness, a foreign-body sensation, and airway obstruction may occur. Dysphagia is also a possible symptom.
The radiologic features are usually those typical of benign neoplasms, with well-circumscribed margins with no invasion of surrounding tissue.11 Farboud A, Pratap R, Helquist H, Montgomery P. An unusual cause of obstructive sleep apnoea. J Laryngol Otol 2009;123:e22 In a few cases, computed tomography (CT) findings may mimic the appearance of the malignant lesions with indistinct borders and blending with adjacent isodense muscle tissue. Magnetic resonance imaging is better at delineating RM from surrounding structures.
The differential diagnosis for laryngeal masses includes cysts, laryngoceles, malignant neoplasms such as squamous cell carcinoma and rhabdomyosarcoma, as well as benign neoplasms such as hemangiomas, lipomas, amyloidomas, neurofibromas, and granular cell tumors.55 Brys AK, Sakai O, DeRosa J, Shapshay SM. Rhabdomyoma of the larynx: case report and clinical and pathologic review. Ear Nose Throat J 2005;84:437-440
Histologic analysis is essential for diagnosis. Adult RM have been confused with many other benign tumors as hibernoma, oncocytoma, tumor of salivary glands, paraganglioma, and others,66 Pichi B, Manciocco V, Marchesi P, et al. Rhabdomyoma of the parapharyngeal space presenting with dysphagia. Dysphagia 2008;23:202-204 but mainly with granular cell tumor.11 Farboud A, Pratap R, Helquist H, Montgomery P. An unusual cause of obstructive sleep apnoea. J Laryngol Otol 2009;123:e22 Microscopically the adult RM is characterized by large, closely packed, elongated to polygonal cells with pink to bright eosinophilic and finely granular cytoplasm. The nuclei are round to oval, vesicular, usually peripherally located, but may be centrally located. Prominent nucleoli are frequently noted. Cross-striations are characteristic but are not an obligatory feature in light microscopic evaluation.22 Hamper K, Renninghoff J, Schäfer H. Rhabdomyoma of the larynx recurring after 12 years: immunocytochemistry and differential diagnosis. Arch Otorhinolaryngol 1989;246:222-226 They are more easily seen with phosphotungstic acid hematoxylin staining. Ultrastructural studies showed actin filament and Z bands.
The diagnosis of RM is histopathologic and can generally be well defined, but some cases can cause difficulties. Immunohistochemistry (IHC) reactions are of particular value in differentiating the similar lesions. The IHC features of RM are identical to those of normal skeletal muscle cells because it shows positivity to MSA (muscle-specific actin), desmin, and myoglobin.66 Pichi B, Manciocco V, Marchesi P, et al. Rhabdomyoma of the parapharyngeal space presenting with dysphagia. Dysphagia 2008;23:202-204 The positivity of these muscular markers is consistent with RM, as well as the positivity for vimentin, a marker of mesenchymal tissues.22 Hamper K, Renninghoff J, Schäfer H. Rhabdomyoma of the larynx recurring after 12 years: immunocytochemistry and differential diagnosis. Arch Otorhinolaryngol 1989;246:222-226 The main lesion to be differentiated from RM is the granular cell tumor that morphologically consists mainly of smaller cells, has no cross-striations, and is consistently positive for S-100 protein but negative for all myogenous markers IHC preparations.22 Hamper K, Renninghoff J, Schäfer H. Rhabdomyoma of the larynx recurring after 12 years: immunocytochemistry and differential diagnosis. Arch Otorhinolaryngol 1989;246:222-226
RM treatment is surgical resection. This procedure should be as conservative as possible. Local recurrence has been reported and usually results from incomplete resection.55 Brys AK, Sakai O, DeRosa J, Shapshay SM. Rhabdomyoma of the larynx: case report and clinical and pathologic review. Ear Nose Throat J 2005;84:437-440
Case Report
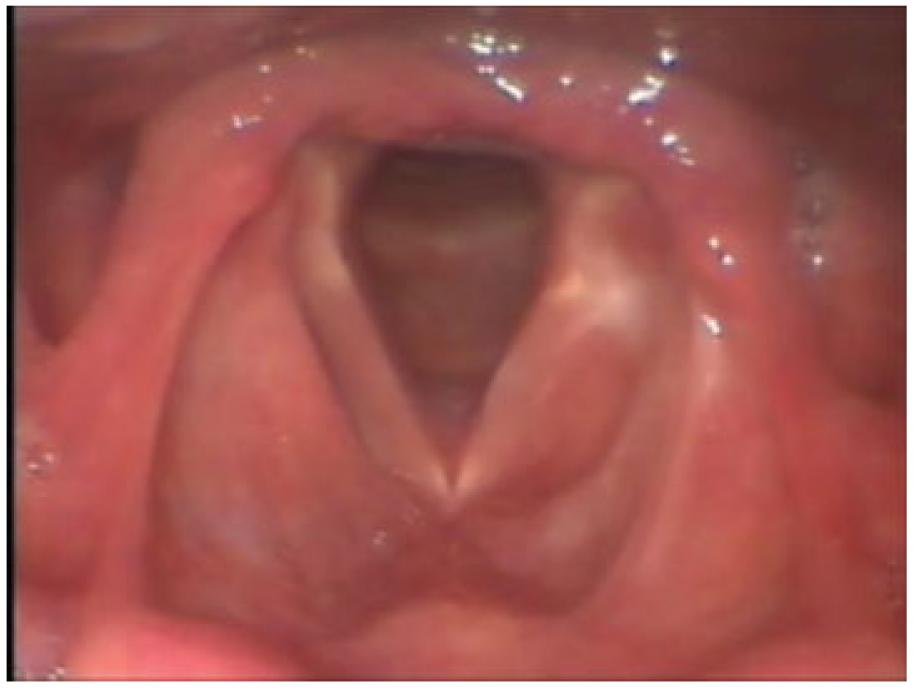
The 35-year-old white man complained of progressive hoarseness during a 1-year period. On indirect examination of the larynx, a large submucosal mass was noted in the left supra glottic larynx (Fig. 1). The contrast-enhanced CT of the neck revealed a well-demarcated diffusely hyperattenuating submucosal mass on the left supraglottic space (Fig. 2).
The patient was taken to the operating room where the mass was endoscopically dissected.
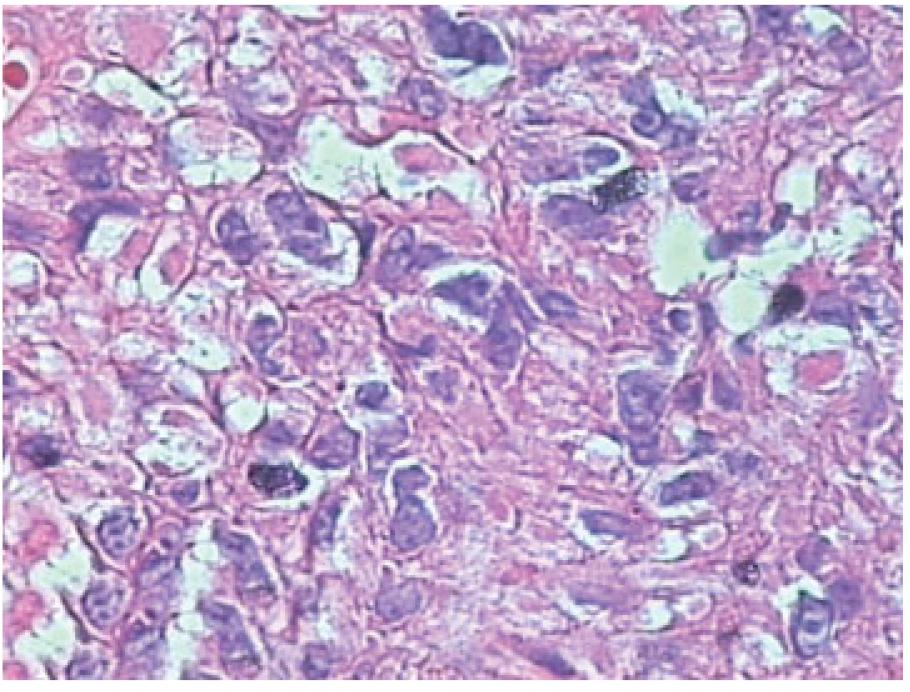
The histopathologic diagnosis was of polygonal cell neoplastic favorable to paraganglioma. The pathologist strongly suggested the complementation with IHC studies. IHC stains for desmin (Fig. 3) and vimentin (muscle and mesenchymal markers respectively) were positive. Markers for epithelium membrane tumors and S-100 protein for neuroectoderm tumors were negative, thus changing the diagnosis to RM adult type. At a careful revision of the slides, the hematoxylin and eosin sections revealed neoplastic closely packed polygonal cells with deeply eosinophilic vacuolated cytoplasm (Fig. 4). Nuclei were round, vesicular, centrally located, with prominent nucleoli. Intracytoplasmic and intranuclear hyaline inclusions were seen. Cross-striations, not noted before, were present in few cells (Fig. 5). Mitotic activity and necrosis were absent.
Histology of rhabdomyoma showing closely packed polygonal cells with deeply eosinophilic vacuolated cytoplasm. (Hematoxylin and eosin, × 400.)
The patient recovered well. His voice was normal after a period of 3 months. He is free of recurrence at 15 months of follow-up (Fig. 6).
Discussion
Certainly the adult-type RM of the larynx is an extremely rare benign tumor of myoblastic origin. A literature review allows us to say that only ∼40 well-documented cases have been reported until today worldwide. In the past, RM was confused with other similar tumors, especially with granular cell tumors. This confusion is due to granular eosinophilic cytoplasm that is common to both diagnoses, although they have a completely different histogenesis. Another important observation of the histologic point of view is that the RM should not be confused with rhabdomyosarcoma, which has a completely different prognosis. The histologic diagnosis should be no problem if adequately prepared slides are available, but as these tumors are very rare and many pathologists are not familiar with this type of tumor, there are reports of substantial difficulties to diagnose them on the first try. We present another case of laryngeal RM in a patient whose diagnosis was not initially set. Although the clinical and pathologic findings should be taken into consideration, we emphasize that IHC plays an important role in the differential diagnosis.
Symptoms of laryngeal RM do not differ from those caused by other benign tumors of the larynx, but one should keep in mind the possibility of local airway obstruction when the patient complains of breathing difficulties.
The tumor is usually described as a submucosal mass with a smooth surface that can resemble the appearance of a cyst. Laryngoscopy and imaging exams help locate and define the limits of the tumor, but the definitive diagnosis will always depend on the histopathologic studies.
The clinical outcome of laryngeal RM adult type is benign and no evidence of metastasis was reported in the literature. Treatment should always be surgical removal, via either endoscopic or external approach, but always preserving the adjacent structures such as the vocal folds and the swallowing apparatus. Recurrence can happen but usually is due to incomplete excision of the tumor.
Conclusion
Although muscle tumors of the larynx are very rare, the RM should be considered when there is a submucosal mass in the larynx. Because the establishment of definitive diagnosis can be difficult with routine histopathology, it is important to consider the realization of IHC studies.
References
-
1Farboud A, Pratap R, Helquist H, Montgomery P. An unusual cause of obstructive sleep apnoea. J Laryngol Otol 2009;123:e22
-
2Hamper K, Renninghoff J, Schäfer H. Rhabdomyoma of the larynx recurring after 12 years: immunocytochemistry and differential diagnosis. Arch Otorhinolaryngol 1989;246:222-226
-
3Jensen K, Swartz K. A rare case of rhabdomyoma of the larynx causing airway obstruction. Ear Nose Throat J 2006;85:116-118
-
4Zacharia TT, Som PM. Multiple adult rhabdomyomas of the oropharynx, base of the tongue, and floor of themouth:magnetic resonance findings. Arch Otolaryngol Head Neck Surg 2008;134:892-894
-
5Brys AK, Sakai O, DeRosa J, Shapshay SM. Rhabdomyoma of the larynx: case report and clinical and pathologic review. Ear Nose Throat J 2005;84:437-440
-
6Pichi B, Manciocco V, Marchesi P, et al. Rhabdomyoma of the parapharyngeal space presenting with dysphagia. Dysphagia 2008;23:202-204
Publication Dates
-
Publication in this collection
2013
History
-
Received
16 Nov 2011 -
Accepted
18 Mar 2012