Abstract
Introduction
Head and neck specialists and otorhinolaryngologists are greatly exposed to coronavirus disease 2019 (COVID-19) transmission in their everyday praxis. Many articles are being published regarding medical staff protection and patient management during the pandemic.
Objective
To provide an easy access to and a trustful review of the main aspects that have changed in the head and neck surgery and otorhinolaryngology practice due to the COVID-19 pandemic.
Data Synthesis
The search terms used were: (head and neck or otorhinolaryngology or ORL or thyroid) AND (severe acute respiratory syndrome coronavirus 2 [SARS-COV-2] or COVID-19 or CORONAVIRUS). The results were limited to the year of 2020. Articles were read in English, Portuguese, French, German, and Spanish or translated from Chinese. All included articles were read by at least two authors. Thirty-five articles were included. Most articles suggest postponing elective surgeries, with exception to cancer surgeries, which should be evaluated separately. Twenty-five articles recommended some kind of screening prior to surgery, using polymerase chain reaction (PCR) tests and epidemiological data. Extra precautions, such as use of personal protective equipment (PPE), are suggested for both tracheostomies and endoscopies. Fifteen articles give recommendation on how to use telemedicine.
Conclusion
The use of PPE (N95 or powered air-purifying respirator [PAPR]) during procedures should be mandatory. Patients should be evaluated about their COVID-19 status before hospital admission. Cancer should be treated. Tracheostomy tube cuff should be inflated inside the tracheal incision. All COVID-19 precautions should be kept until there is a validated antiviral treatment or an available vaccine.
Keywords:
head and neck; otorhinolaryngology; COVID-19; surgery; SARS-CoV-2
Introduction
The coronavirus disease 2019 (COVID-19) pandemic started in China, and, in March 11th, it was declared a pandemic.11 Coronavirus disease. COVID-19. Situation Report 2019;51: 2020Mar. From its first registered case up to now—May 26th—5,404,512 confirmed cases were registered and 343,514 patients have died.22 Coronavirus disease (COVID-19) Situation Report-127. 2020 The pandemic not only represents a threat to each country's health system infection control, but to all aspects of its healthcare, as workforces are being transferred to COVID-19 combat areas, and many usual clinical workflows have changed in an effort to achieve pandemic control.33 Zangrillo A, Beretta L, Silvani P, et al. Fast reshaping of intensive care unit facilities in a large metropolitan hospital in Milan, Italy: facing the COVID-19 pandemic emergency. Crit Care Resusc 2020 This represent an indirect impact in people's health, as it affects different medical specialties.
In many hospitals, elective treatments have been canceled to avoid exposing patients and medical staff to unnecessary risks.44 Zheng MH, Boni L, Fingerhut A. Minimally Invasive Surgery and the Novel Coronavirus Outbreak: Lessons Learned in China and Italy. Ann Surg 2020;272(01):e5-e6 55 Hu XH, Niu WB, Zhang JF, et al. [Treatment strategies for colorectal cancer patients in tumor hospitals under the background of corona virus disease 2019]. Zhonghua Wei Chang Wai Ke Za Zhi 2020;23(03):201-208 Even so, emergency and urgent procedures were still being performed with extra precaution. Elective surgeries, when considered time-sensitive, were also, in many cases, still performed after medical group evaluation.66 Zou J, Yu H, Song D, Niu J, Yang H. Advice on Standardized Diagnosis and Treatment for Spinal Diseases during the Coronavirus Disease 2019 Pandemic. Asian Spine J 2020;14(02):258-263 In many areas, a patient-to-patient approach was also suggested with the use of telemedicine, which offers a way to maintain medical support for regular situations as well as allowing the staff to analyze the patient's condition and to evaluate surgery necessity without bringing risk of infection for both professional and patient.77 Di Saverio S, Pata F, Gallo G, et al. Coronavirus pandemic and Colorectal surgery: practical advicebasedon the Italian experience. Color Dis 2020 88 Zhao L, Zhang L, Liu JW, Yang ZF, Shen WZ, Li XR. [The treatment proposal for the patients with breast diseases in the central epidemic area of 2019 coronavirus disease]. Zhonghua Wai Ke Za Zhi 2020;58(05):331-336
In otorhinolaryngology and in head and neck surgery, professionals are at a greater risk of infection. Many usual clinical procedures, such as laryngoscopy, generate a great volume of aerosol, which can lead to great exposure to high virus concentration area.99 Chew M-H, Koh FH, Ng KH. A call to arms: a perspective of safe general surgery in Singapore during the COVID-19 pandemic. Singapore Med J 2020 At the same time, many patients, even without symptoms, may carry the virus, presenting a threat to professionals and incapacitating the continuity of many procedures, even for those asymptomatic individual.1010 Gandhi M, Yokoe DS, Havlir DV. Asymptomatic Transmission, the Achilles' Heel of Current Strategies to Control Covid-19. N Engl J Med 2020;382(22):2158-2160 Many elective surgeries, on the other hand, are cancer-related, and, therefore, the evaluation of their urgency in the pandemic scenario becomes very challenging.1111 Civantos AM, Carey RM, Lichtenstein GR, Lukens JN, Cohen RB, Rassekh CH. Care of immunocompromised patients with head and neck cancer during the COVID-19 pandemic: Two challenging and informative clinical cases. Head Neck 2020;42(06):1131-1136
Our review proposes to organize the current knowledge on the specific characteristics for otorhinolaryngology. Our objective is to bring together the main recommendations regarding surgery indication, use of protective equipment during procedures, endoscopy precautions, and telemedicine application.
Methods
We performed a systematic literature review based on online search in the following databases: PubMed of the National Center for Biotechnology (NCBI), Scientific Electronic Library Online, and Scopus. The terms used in the search for any correspondence were (head and neck or otorhinolaryngology or ORL or thyroid) AND (severe acute respiratory syndrome coronavirus 2 [SARS-COV-2] or COVID-19 or coronavirus). Search results were limited to articles from the year 2020. Duplicates were excluded using the EndNote X9 application (Clarivate Analytics, Philadelphia, PA, USA) and Rayyan platform (Qatar Computing Research Institute, Doha, Ad-Dawhah, Qtar). The authors selected the articles for full reading according to the content of the title and abstract, evaluating if they were related to the scope of the present work.
Before reading all the articles selected by title and abstract, we also included articles that contained surgical recommendations related to otorhinolaryngological surgery or head and neck surgery from another review made by the same group.1212 Hojaij FC, Chinelatto LA, Boog GHP, Kasmirski JA, Lopes JVZ, Sacramento FM. Surgical Practice in the Current COVID-19 Pandemic: A Rapid Systematic Review. Clinics (São Paulo) 2020;75: e1923 EndNote was used again to exclude duplicates. All selected articles were read in full by two authors. Articles were read in their original language if in Portuguese, English, French, Spanish, or German. Chinese articles were translated using online websites. Articles in other languages were excluded. After full-reading, articles were included if they brought opinions or information on any of the following topics: (a) postponement of procedures; (b) performance of endoscopic exams; (c) use of telemedicine, and (d) thyroid cancer management. In cases of disagreement between the two authors about the relevance of the study, all authors discussed the inclusion of the reference. Manual search was also performed during the manuscript writing to add relevant papers published during the period of elaboration of the present article. Articles were excluded if (a) not focused on head and neck surgery OR othorhynolaryngology; (b) focused on specific COVID-19 treatment, or (c) focused on airway management for COVID-19 cases.
Each of the above listed topics has been subclassified according to main characteristics after qualitative analyses of references. Specific interest regarding thyroid cancer is related to its prevalence in the ordinary head and neck surgery clinic. Recommendations regarding patient and professional safety have also been collected. We also analyzed specifically recommendations concerning tracheostomies, as it is a subject of great interest in this epidemy.
Data analysis was performed by Google Sheets application (Google LLC, Menlo Park, CA, USA).
Review of Literature
Records
We found 204 papers (202 on databases; 2 through other sources) in our initial search. Of them, 35 filled the eligibility criteria after a systematic evaluation (Fig. 1). These selected records basically consisted of editorials, original articles, reviews, case reports, opinion/commentary papers, and letters (Fig. 2).
Selection Diagram Six papers that were included in our main results have not been specifically cited in our findings but were considered in our main results.1313 Tysome JR, Bhutta MF. COVID-19: Protecting our ENT Workforce. Clin Otolaryngol 2020;45(03):311-312 1414 Crossley J, Clark C, Brody F, Maxwell JH. Surgical Considerations for an Awake Tracheotomy During the COVID-19 Pandemic. J Laparoendosc Adv Surg Tech A 2020;30(05):477-480 1515 Kligerman MP, Vukkadala N, Tsang RKY, et al. Managing head and neck cancer patients with tracheostomy or laryngectomy during the COVID-19 pandemic. Head Neck 2020;42(06):1209-1213 1616 Schultz P, Morvan JB, Fakhry N, et al; French Society of Otorhinolaryngology, Head, Neck Surgery (SFORL); French Society of Head, Neck Carcinology (SFCCF). French consensus regarding precautions during tracheostomy and post-tracheostomy care in the context of COVID-19 pandemic. Eur Ann Otorhinolaryngol Head Neck Dis 2020;137(03):167-169 1717 Cheng X, Liu J, Li N, et al. Otolaryngology Providers Must Be Alert for Patients with Mild and Asymptomatic COVID-19. Vol. 162, Otolaryngology - Head and Neck Surgery (United States). SAGE Publications Inc.; 2020:809-10 1818 Saadi RA, Bann DV, Patel VA, Goldenberg D, May J, Isildak H. A Commentary on Safety Precautions for Otologic Surgery during the COVID-19 Pandemic. Vol. 162, Otolaryngology - Head and Neck Surgery (United States). SAGE Publications Inc.; 2020. p. 797-9.
Surgical Routine
Twenty-seven articles provided recommendations concerning adaptations of surgery routine and criteria to operate non-cancer surgery cases. Twenty articles suggested postponing all elective procedures or examinations. Only 2 articles disagreed with this guidance. The use of negative-pressure room was endorsed by 10 studies; other 2 also recommended the use of high efficiency particulate (HEPA) filters in the operation room (OR) to decrease hospital airborne transmission. Nine papers reported staff restrictions during procedures, and 6 of them suggested that surgeries should be performed by the most experienced professionals available, avoiding the presence of non-senior residents and medical students. Four articles described contact restriction between older assistants and patients as a measure to decrease high-risk group exposure.
The use of personal protective equipment (PPE) is a central recommendation of the majority (n= 21) of the reviewed articles. Gloves, N95 or filtering facepiece 2 (FFP2) masks, gown, and eye protection are the minimum essential pieces of equipment to protect the health care provider in the OR. Three studies still stratify the use of PPE in two groups: enhanced airborne precautions and extreme airborne precaution. They differ between type of mask used: the first one recommends N95 masks, in context of intermediate risk of infection; and the second one suggests the use of powered air purifying respirators (PAPRs), in scenario of high-risk of infection.
Surgical Screening for SARS-CoV-2
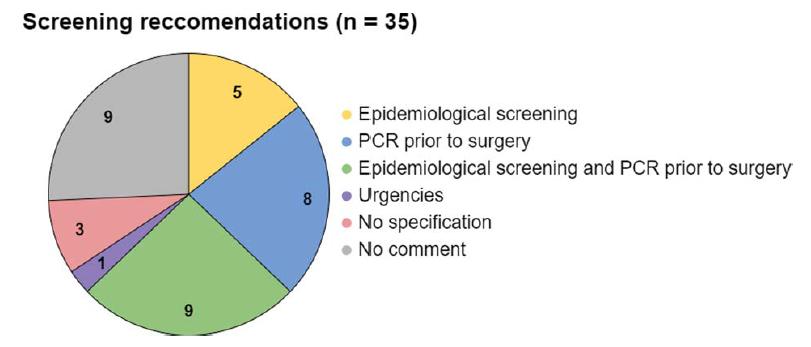
From the 35 articles included in the present review, the majority (n= 25) recommended some kind of evaluation for any surgery patient (Fig. 3). The most prevalent method was an epidemiological (recent travel and symptoms) questionnaire applied before the patient's consult or entry to the hospital combined with polymerase chain reaction (PCR) prior to surgery. Other recommendations split this method: only epidemiological screening or PCR prior to surgery. Three articles adopted some kind of screening but did not specify which one.
Screening Recommendations The articles selected were distributed in six categories according to the findings related to screening for coronavirus 2019 (COVID-19): those that recommended only epidemiological screening (n= 5), those that recommended nasopharynx swab polymerase chain reaction (PCR) prior to surgery (n= 8), those that recommended epidemiological screening prior to consult combined with nasopharynx swab PCR prior to surgery (n= 9), those that recommended PCR in urgent situations (n= 1), those that recommended some kind of screening but did not specify the type (n= 3), and those that did not have any kind of recommendation (n= 9).
Cancer Management
Thirteen articles proposed recommendations for cancer management in this pandemic scenario. There is consensus that cancer should be treated if their prognosis can get worse by a delay of minimally 60 days. Two articles also suggest using chemo and/or radiotherapy to mitigate surgery delay impacts, if this approach is already a validated option in the tumor of concern treatment.1919 Bann DV, Patel VA, Saadi R, et al. Impact ofcoronavirus (COVID-19) on otolaryngologic surgery: Brief commentary. Head Neck 2020; 42(06):1227-1234 2020 Day AT, Sher DJ, Lee RC, et al. Head and neck oncology during the COVID-19 pandemic: Reconsidering traditional treatment paradigms in light of new surgical and other multilevel risks. Oral Oncol 2020;105:104684
Six articles mentioned how to specifically treat thyroid cancer. Three articles were from the United States of America, one from Italy, one from China, and one from France. Three of them suggested that each case should be individually assessed regarding surgical treatment postponement. The other three already specified that all low-risk thyroid cancers, especially papillary thyroid carcinoma, should have their surgical treatment delayed.
Endoscopic Exams
Regarding endoscopic examinations, one of the most common procedures performed by otolaryngologists, 18 papers had specific recommendations to improve safety. Of them, 11 articles endorsed avoiding the performance of this exam, unless medically necessary,1919 Bann DV, Patel VA, Saadi R, et al. Impact ofcoronavirus (COVID-19) on otolaryngologic surgery: Brief commentary. Head Neck 2020; 42(06):1227-1234 2121 Chaves ALF, Castro AF, Marta GN, et al. Emergency changes in international guidelines on treatment for head and neck cancer patients during the COVID-19 pandemic. Oral Oncol 2020; 107:104734 2222 Hennessy M, Bann DV, Patel VA, et al. Commentary on the management of total laryngectomy patients during the COVID19 pandemic. Head Neck 2020;42(06):1137-1143 2323 Fakhry N, Schultz P, Morinière S, et al; French Society of Otorhinolaryngology, Head and Neck Surgery (SFORL); French Society of Head and Neck Carcinology (SFCCF). French consensus on management of head and neck cancer surgery during COVID-19 pandemic. Eur Ann Otorhinolaryngol Head Neck Dis 2020;137 (03):159-160 2424 Frauenfelder C, Butler C, Hartley B, et al. Practical insights for paediatric otolaryngology surgical cases and performing microlaryngobronchoscopy during the COVID-19 pandemic. Int J Pediatr Otorhinolaryngol 2020;134:110030 2525 Givi B, Schiff BA, Chinn SB, et al. Safety Recommendations for Evaluation and Surgery of the Head and Neck During the COVID19 Pandemic. JAMA Otolaryngol Neck Surg 2020 2626 Hsieh TY, Dedhia RD, Chiao W, et al. A Guide to Facial Trauma Triage and Precautions in the COVID-19 Pandemic. Facial Plast Surg Aesthet Med 2020;22(03):164-169 2727 Krajewska J, Krajewski W, Zub K, Zatonski T. COVID-19 in otolaryngologist practice: a review of current knowledge. Eur Arch Otorhinolaryngol 2020;277(07):1885-1897 2828 Leboulanger N, Sagardoy T, Akkari M, et al; French Association of Pediatric Otorhinolaryngology (AFOP); French Society of Otorhinolaryngology; Head, Neck Surgery (SFORL); Guidelines of the French Association of Pediatric Otorhinolaryngology (AFOP) and French Society of Otorhinolaryngology (SFORL). COVID-19 and ENT Pediatric otolaryngology during the COVID-19 pandemic. Eur Ann Otorhinolaryngol Head Neck Dis 2020;137(03): 177-181 2929 Topf MC, Shenson JA, Holsinger FC, et al. Framework for prioritizing head and neck surgery during the COVID-19 pandemic. Head Neck 2020;42(06):1159-1167 3030 Vukkadala N, Qian ZJ, Holsinger FC, Patel ZM, Rosenthal E. COVID. 19 and the Otolaryngologist: Preliminary Evidence-Based Review. Laryngoscope 2020 and 7 just had general suggestions.3131 Chan JYK, Tsang RKY, Yeung KW, et al. There is no routine head and neck exam during the COVID-19 pandemic. Head Neck 2020; 42(06):1235-1239 3232 Kowalski LP, Sanabria A, Ridge JA, et al. COVID-19 pandemic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practice. Head Neck 2020;42(06): 1259-1267 3333 Lu D, Wang H, Yu R, Yang H, Zhao Y. Integrated infection control strategy to minimize nosocomial infection of coronavirus disease 2019 among ENT healthcare workers. J Hosp Infect 2020;104(04): 454-455 3434 Lüers J-C, Klußmann JP, Guntinas-Lichius O. Die COVID-19-Pandemie und das HNO-Fachgebiet: Worauf kommt es aktuell an? Laryngorhinootologie 2020;99(05):287-291 3535 Parikh SR, Bly RA, Bonilla-Velez J, et al. Pediatric Otolaryngology Divisional and Institutional Preparatory Response at Seattle Children's Hospital after COVID-19 Regional Exposure. Otolaryngol Neck Surg 2020 3636 Rameau A, Young VN, Amin MR, Sulica L. Flexible Laryngoscopy and COVID-19. Otolaryngol Neck Surg 2020 3737 Xu K, Lai X, Liu Z. Suggestions on the prevention of COVID-19 for health care workers in department of otorhinolaryngology head and neck surgery. World J Otorhinolaryngol -. Head Neck Surg 2020 Some practical recommendations found in our review regarding endoscopic examinations are listed below:
-
(a) Hand hygiene before and after contact with patients or other potentially infected sources.3636 Rameau A, Young VN, Amin MR, Sulica L. Flexible Laryngoscopy and COVID-19. Otolaryngol Neck Surg 2020
-
(b) Screening of staff3232 Kowalski LP, Sanabria A, Ridge JA, et al. COVID-19 pandemic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practice. Head Neck 2020;42(06): 1259-1267 and patients in communities with a high prevalence of COVID-19, even asymptomatic patients should be managed with suspicion.3636 Rameau A, Young VN, Amin MR, Sulica L. Flexible Laryngoscopy and COVID-19. Otolaryngol Neck Surg 2020
-
(c) Performing the examination in an isolated room, preferably with negative pressure.3535 Parikh SR, Bly RA, Bonilla-Velez J, et al. Pediatric Otolaryngology Divisional and Institutional Preparatory Response at Seattle Children's Hospital after COVID-19 Regional Exposure. Otolaryngol Neck Surg 2020 3838 Balakrishnan K, Schechtman S, Hogikyan ND, Teoh AYB, McGrath B, Brenner MJ. COVID-19 Pandemic: What Every Otolaryngologist-Head and Neck Surgeon Needs to Know for Safe Airway Management. Otolaryngol Neck Surg 2020
-
(d) Choosing anesthetic gels over anesthetic sprays, and ensuring adequate surface anesthesia to reduce cough and sneeze reflexes.3333 Lu D, Wang H, Yu R, Yang H, Zhao Y. Integrated infection control strategy to minimize nosocomial infection of coronavirus disease 2019 among ENT healthcare workers. J Hosp Infect 2020;104(04): 454-455
-
(e) Practicing high-level disinfection of the endoscopes and decontamination of all surface areas of the examination room.2828 Leboulanger N, Sagardoy T, Akkari M, et al; French Association of Pediatric Otorhinolaryngology (AFOP); French Society of Otorhinolaryngology; Head, Neck Surgery (SFORL); Guidelines of the French Association of Pediatric Otorhinolaryngology (AFOP) and French Society of Otorhinolaryngology (SFORL). COVID-19 and ENT Pediatric otolaryngology during the COVID-19 pandemic. Eur Ann Otorhinolaryngol Head Neck Dis 2020;137(03): 177-181 3636 Rameau A, Young VN, Amin MR, Sulica L. Flexible Laryngoscopy and COVID-19. Otolaryngol Neck Surg 2020
-
(f) Using disposable nasal pledgets for decongestion.1919 Bann DV, Patel VA, Saadi R, et al. Impact ofcoronavirus (COVID-19) on otolaryngologic surgery: Brief commentary. Head Neck 2020; 42(06):1227-1234
Tracheostomy
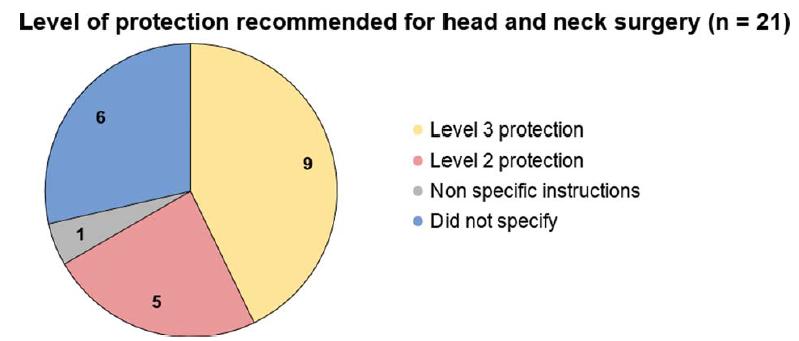
Twenty-two articles mentioned instructions on general measures to perform safe tracheostomies. Applying anesthetics on high respiratory tract found to be useful to diminish the possibility of virus spread by coughing during the surgery, 7 of the articles answered positive to the technique, 14 of them did not mention the subject. Fourteen articles agreed that establishing negative pressure inside the OR is important to reduce the contagion between multiple patients frequenting the surgical floor, 7 of them did not mention the subject. Thirteen articles believed that insufflating the cuff under the opening incision during tracheostomy procedure, to form a closed system is adequate to limit the virus, 8 of them did not mention the subject. The level of protection PPE needed to protect health workers was different in several articles, as it is possible to see in Fig. 4.
Level of protection recommended for head and neck surgery in the context of COVID-19 pandemic Level 3 consists of complete gown and powered air purifying respirator (PAPR); level 2 consists of complete gown and N95 mask, and non-specific instructions consist of a combination of levels 2 and 3 recommendations based on polymerase chain reaction results.
Telemedicine
Fifteen articles from the 35 selected recommended the use of telemedicine for triage, routine consults or patient revaluation (Fig. 5). Four articles recommended the use of telemedicine but did not specify the situations to be used. The other 16 articles did not comment about telemedicine.
Telemedicine Recommendations The graphic divides into categories the articles that recommended the use of telemedicine specifically for triage, routine consults, and patient revaluation (n= 15); the ones that recommended the use of telemedicine, but did not specify for what situations (n= 4), and those that did not have any comment related to telemedicine (n= 16).
Discussion
Surgical Routine
The risk of aerosolization and droplets made the Otorhinolaryngology and Head and Neck surgery setting as an extreme high-risk area for contamination and transmission of SARS-CoV-2. Because of that, there is an important concern with reducing transmission between staff and patients, which should guide the readaptation of surgery routines in the recent pandemic scenario. Besides that, there is evidence that surgery or chemotherapy are isolated risk factor to negative outcomes in patients diagnosed with COVID-19, amplifying the difficulties to managing surgical conditions.2121 Chaves ALF, Castro AF, Marta GN, et al. Emergency changes in international guidelines on treatment for head and neck cancer patients during the COVID-19 pandemic. Oral Oncol 2020; 107:104734
In this context, surgery indication should be restricted to procedures that can impact disease prognosis. Except for cancer management, whose recommendations are discussed below, there is a consensus that only emergency/urgency situations, mainly bleeding or high-risk obstructive airway situations, should be assessed by surgery.1111 Civantos AM, Carey RM, Lichtenstein GR, Lukens JN, Cohen RB, Rassekh CH. Care of immunocompromised patients with head and neck cancer during the COVID-19 pandemic: Two challenging and informative clinical cases. Head Neck 2020;42(06):1131-1136 Other studies extended the roll of procedures to treat to conditions in which the delay of intervention could worsen functional and aesthetic outcomes.2626 Hsieh TY, Dedhia RD, Chiao W, et al. A Guide to Facial Trauma Triage and Precautions in the COVID-19 Pandemic. Facial Plast Surg Aesthet Med 2020;22(03):164-169 3030 Vukkadala N, Qian ZJ, Holsinger FC, Patel ZM, Rosenthal E. COVID. 19 and the Otolaryngologist: Preliminary Evidence-Based Review. Laryngoscope 2020 Other procedures should be postponed for 30 days or more, with frequent revaluations. Only two reports distinguish about this guidance. One Chinese hospital reported to have maintained operations in all circumstances after a readaptation of its infrastructure.3333 Lu D, Wang H, Yu R, Yang H, Zhao Y. Integrated infection control strategy to minimize nosocomial infection of coronavirus disease 2019 among ENT healthcare workers. J Hosp Infect 2020;104(04): 454-455 Another paper clarifies that they did not postpone interventions in patients with negative status for COVID-19.2121 Chaves ALF, Castro AF, Marta GN, et al. Emergency changes in international guidelines on treatment for head and neck cancer patients during the COVID-19 pandemic. Oral Oncol 2020; 107:104734 These situations, however, represent a minority (10%) of the reviewed literature. Our vision is that every case should be individualized.
Staff protection is a major concern. There is a consensus that the minimum PPE include use of gloves, gown, eye protection, and N95 mask or PFF2. Some articles showed superiority of PAPR over other masks.2626 Hsieh TY, Dedhia RD, Chiao W, et al. A Guide to Facial Trauma Triage and Precautions in the COVID-19 Pandemic. Facial Plast Surg Aesthet Med 2020;22(03):164-169 3030 Vukkadala N, Qian ZJ, Holsinger FC, Patel ZM, Rosenthal E. COVID. 19 and the Otolaryngologist: Preliminary Evidence-Based Review. Laryngoscope 2020 3535 Parikh SR, Bly RA, Bonilla-Velez J, et al. Pediatric Otolaryngology Divisional and Institutional Preparatory Response at Seattle Children's Hospital after COVID-19 Regional Exposure. Otolaryngol Neck Surg 2020 It was demonstrated that PAPR has a higher assigned protective factor than N95 (25–100 versus 10).2525 Givi B, Schiff BA, Chinn SB, et al. Safety Recommendations for Evaluation and Surgery of the Head and Neck During the COVID19 Pandemic. JAMA Otolaryngol Neck Surg 2020 However, due to management of resources and disponibility of these devices, two articles presented a stratification of risk status; thus, they reserve the use of PAPR only in situations of higher risk of aerosolization and viral exposure. The suggested workflow indicates two categories: 1) extreme airborne protection that demands the use of PAPR and is reserved to high aerosolization procedures (e.g., tracheostomy, endoscopy and the access of aerodigestive mucous), and 2) enhanced airborne protection, which allows the use of N95 masks and is indicated for cases of mild-risk of contamination.2626 Hsieh TY, Dedhia RD, Chiao W, et al. A Guide to Facial Trauma Triage and Precautions in the COVID-19 Pandemic. Facial Plast Surg Aesthet Med 2020;22(03):164-169 3030 Vukkadala N, Qian ZJ, Holsinger FC, Patel ZM, Rosenthal E. COVID. 19 and the Otolaryngologist: Preliminary Evidence-Based Review. Laryngoscope 2020 Nevertheless, PAPR can be incompatible with some procedures, because it does not allow the use of instruments by the surgeon, for instance, loupes, headlight, and microscope.2020 Day AT, Sher DJ, Lee RC, et al. Head and neck oncology during the COVID-19 pandemic: Reconsidering traditional treatment paradigms in light of new surgical and other multilevel risks. Oral Oncol 2020;105:104684 3535 Parikh SR, Bly RA, Bonilla-Velez J, et al. Pediatric Otolaryngology Divisional and Institutional Preparatory Response at Seattle Children's Hospital after COVID-19 Regional Exposure. Otolaryngol Neck Surg 2020 It is also necessary to emphasize the importance of correct use and disposal of PPE, as some literature brings to evidence that failure in these steps can be related to high infection rates in health care workers.3939 Kulcsar MA, Montenegro FL, Arap SS, Tavares MR, Kowalski LP. High Risk of COVID-19 Infection for Head and Neck Surgeons. Int Arch Otorhinolaryngol 2020;24(02):e129-e130 An article even advised doing specific training to perform a surgery using PPE.2424 Frauenfelder C, Butler C, Hartley B, et al. Practical insights for paediatric otolaryngology surgical cases and performing microlaryngobronchoscopy during the COVID-19 pandemic. Int J Pediatr Otorhinolaryngol 2020;134:110030 It is our understanding that these precautions should become a habit until there is scientifical proved control over the coronavirus pandemics, such as vacines or antiviral drugs.
Other aspects concerning team surgery are raised. To minimize the exposure of the surgical teams, most articles agree in limiting nurse and medical staff to the minimum possible and excluding students and non-senior residents from the OR. Procedures should be performed by the most experienced and skilled surgeon in the team to reduce time of aerosolized air exposure. Furthermore, an article suggested briefing before every surgery, to make it more efficient.2424 Frauenfelder C, Butler C, Hartley B, et al. Practical insights for paediatric otolaryngology surgical cases and performing microlaryngobronchoscopy during the COVID-19 pandemic. Int J Pediatr Otorhinolaryngol 2020;134:110030 There are also concerns about the vulnerability of some work care professionals. Four articles recommend to save attendants older than 55 years of age from contact with patients, and one of them3232 Kowalski LP, Sanabria A, Ridge JA, et al. COVID-19 pandemic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practice. Head Neck 2020;42(06): 1259-1267 extends this advice to pregnant workers and/or those who have chronic diseases.
Some precautions should be addressed regarding surgical setting and use of instruments. There is a need to contain aerosolized air produced by surgery and avoid the contamination of other hospital sites and areas classified as non-infected. Therefore, procedures should be performed in negative pressure rooms and, if possible, equipped with a HEPA filter. A professional must be allocated to be available for eventual needs, thus avoiding the exit of any OR staff member before conclusion of the procedure. The use of powered devices, like drills, microdebriders, saws, or ultrasonic shears, ought to avoided, and if they are used, irrigation pressure must be kept to a minimum.2626 Hsieh TY, Dedhia RD, Chiao W, et al. A Guide to Facial Trauma Triage and Precautions in the COVID-19 Pandemic. Facial Plast Surg Aesthet Med 2020;22(03):164-169
Surgical Screening for SARS-CoV2
Another aspect that should be considered when trying to determine the need for medical attendance or surgery is the possibility that the patient is already contaminated. With this possibility, the predominant recommendation—26 articles of the pool—is to screen the patient prior to the procedure, such as applying a questionnaire about recent travels, clinical manifestations, or even performing a PCR test. These surgical screening procedures should be part of institutional protocols until the current pandemic is safely contained.
With most countries presenting community transmission, allied with the possibility of asymptomatic contamination, the exclusive use of questionnaire about recent travels or contact with suspected COVID-19 patients is not enough to guarantee that the patient does not carry the virus. Most articles suggested a combined epidemiological and PCR screening, with questionnaire about recent travels, contact with suspected COVID-19 patients, and clinical manifestations being applied before the patients enter the hospital, and reverse transcription polymerase chain reaction (RT-PCR) being performed 2 to 3 days prior to surgery or as part of the preoperative care.
Some articles suggested, if possible, other kinds of screening allied with the above, such as doing blood count and lactate dehydrogenase (LDH) together with PCR and, if there is any alteration, a tomography is recommended.4040 Ansarin M. Surgical management of head and neck tumours during the SARS-CoV (COVID-19) pandemic. Acta Otorhinolaryngol Ital 2020;40(02):87-89 Given recent findings,4141 Liang W, Liang H, Ou L, et al; China Medical Treatment Expert Group for COVID-19. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Intern Med 2020 this parameter could come in handy for those patients that test positive for SARS-CoV-2. Other articles recommended similar approaches, for example doing a computed tomography (CT) along with PCR.2727 Krajewska J, Krajewski W, Zub K, Zatonski T. COVID-19 in otolaryngologist practice: a review of current knowledge. Eur Arch Otorhinolaryngol 2020;277(07):1885-1897 2828 Leboulanger N, Sagardoy T, Akkari M, et al; French Association of Pediatric Otorhinolaryngology (AFOP); French Society of Otorhinolaryngology; Head, Neck Surgery (SFORL); Guidelines of the French Association of Pediatric Otorhinolaryngology (AFOP) and French Society of Otorhinolaryngology (SFORL). COVID-19 and ENT Pediatric otolaryngology during the COVID-19 pandemic. Eur Ann Otorhinolaryngol Head Neck Dis 2020;137(03): 177-181 3333 Lu D, Wang H, Yu R, Yang H, Zhao Y. Integrated infection control strategy to minimize nosocomial infection of coronavirus disease 2019 among ENT healthcare workers. J Hosp Infect 2020;104(04): 454-455 4242 Sun Y, Hu YJ, Xiao HJ. [Suggestions for emergency operation of otorhinolaryngology head and neck during the period of prevention and control of 2019 novel coronavirus]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2020;55(04):322-325 It must also be taken in consideration that children are usually less symptomatic; therefore, pediatric cases should always be treated as if they were COVID-19 + or PCR testing should be done.2424 Frauenfelder C, Butler C, Hartley B, et al. Practical insights for paediatric otolaryngology surgical cases and performing microlaryngobronchoscopy during the COVID-19 pandemic. Int J Pediatr Otorhinolaryngol 2020;134:110030
For situations in which PCR testing is not possible due to lack of resources, a three-level triage for emergencies and clinics could be of good use.4343 Cai YC, Wang W, Li C, et al. Treating head and neck tumors during the SARS-CoV-2 epidemic, 2019 to 2020: Sichuan Cancer Hospital. Head Neck 2020;42(06):1153-1158 This method poses questions about clinical symptons and epidemiological data in diferent times of inpatient admission and procedures. Another possibility—especially in emergency situations—is for centers with sufficient PPE to consider patients to be contaminated with the virus, regardless of symptoms, which reduces the demand of PCR testing and allows a quick approach to patient care while decreasing the chance of infection in head and neck procedures.
Cancer Management
There is little debate on the urgency of operating head and neck cancers, and, therefore, even during the COVID-19 pandemic, high-risk cancer surgeries should still be performed.2121 Chaves ALF, Castro AF, Marta GN, et al. Emergency changes in international guidelines on treatment for head and neck cancer patients during the COVID-19 pandemic. Oral Oncol 2020; 107:104734 2929 Topf MC, Shenson JA, Holsinger FC, et al. Framework for prioritizing head and neck surgery during the COVID-19 pandemic. Head Neck 2020;42(06):1159-1167 4040 Ansarin M. Surgical management of head and neck tumours during the SARS-CoV (COVID-19) pandemic. Acta Otorhinolaryngol Ital 2020;40(02):87-89 4343 Cai YC, Wang W, Li C, et al. Treating head and neck tumors during the SARS-CoV-2 epidemic, 2019 to 2020: Sichuan Cancer Hospital. Head Neck 2020;42(06):1153-1158 Dealing with cancer patients during this pandemic brings great anxiety for the patient and distress for the doctor. Otherwise, a possible delay, especially if longer than 2 months, could change the cancer staging.4444 Murphy CT, Galloway TJ, Handorf EA, et al. Survival Impact of Increasing Time to Treatment Initiation for Patients With Head and Neck Cancer in the United States. J Clin Oncol 2016;34(02): 169-178 4545 Kowalski LP, Carvalho AL. Influence of time delay and clinical upstaging in the prognosis of head and neck cancer. Oral Oncol 2001;37(01):94-98 Even so, this is not universal. Low-risk cancers, such as papilary thyroid carcinoma, can be postponed. Some authors defend a guideline-based approach,2929 Topf MC, Shenson JA, Holsinger FC, et al. Framework for prioritizing head and neck surgery during the COVID-19 pandemic. Head Neck 2020;42(06):1159-1167 4040 Ansarin M. Surgical management of head and neck tumours during the SARS-CoV (COVID-19) pandemic. Acta Otorhinolaryngol Ital 2020;40(02):87-89 4343 Cai YC, Wang W, Li C, et al. Treating head and neck tumors during the SARS-CoV-2 epidemic, 2019 to 2020: Sichuan Cancer Hospital. Head Neck 2020;42(06):1153-1158 while others suggest evaluating each case individually.1919 Bann DV, Patel VA, Saadi R, et al. Impact ofcoronavirus (COVID-19) on otolaryngologic surgery: Brief commentary. Head Neck 2020; 42(06):1227-1234 2020 Day AT, Sher DJ, Lee RC, et al. Head and neck oncology during the COVID-19 pandemic: Reconsidering traditional treatment paradigms in light of new surgical and other multilevel risks. Oral Oncol 2020;105:104684 2323 Fakhry N, Schultz P, Morinière S, et al; French Society of Otorhinolaryngology, Head and Neck Surgery (SFORL); French Society of Head and Neck Carcinology (SFCCF). French consensus on management of head and neck cancer surgery during COVID-19 pandemic. Eur Ann Otorhinolaryngol Head Neck Dis 2020;137 (03):159-160
There are also other aspects related to cancer treatment during the COVID-19 pandemic that should be noted. Concentrating treatment in non-COVID-19 care hospitals is advisable.4040 Ansarin M. Surgical management of head and neck tumours during the SARS-CoV (COVID-19) pandemic. Acta Otorhinolaryngol Ital 2020;40(02):87-89 To reduce nosocomial infection risk, some authors suggested limiting the number of accompanying persons allowed,4343 Cai YC, Wang W, Li C, et al. Treating head and neck tumors during the SARS-CoV-2 epidemic, 2019 to 2020: Sichuan Cancer Hospital. Head Neck 2020;42(06):1153-1158 or even prohibiting them,4040 Ansarin M. Surgical management of head and neck tumours during the SARS-CoV (COVID-19) pandemic. Acta Otorhinolaryngol Ital 2020;40(02):87-89 as we have done in our institution. All patients should be checked for symptoms before entering the hospital, and procedures are only made after either a PCR test or a chest CT is done.1919 Bann DV, Patel VA, Saadi R, et al. Impact ofcoronavirus (COVID-19) on otolaryngologic surgery: Brief commentary. Head Neck 2020; 42(06):1227-1234 2323 Fakhry N, Schultz P, Morinière S, et al; French Society of Otorhinolaryngology, Head and Neck Surgery (SFORL); French Society of Head and Neck Carcinology (SFCCF). French consensus on management of head and neck cancer surgery during COVID-19 pandemic. Eur Ann Otorhinolaryngol Head Neck Dis 2020;137 (03):159-160 4343 Cai YC, Wang W, Li C, et al. Treating head and neck tumors during the SARS-CoV-2 epidemic, 2019 to 2020: Sichuan Cancer Hospital. Head Neck 2020;42(06):1153-1158
Treatment choice should take many factors into consideration, such as: patient hospital exposure, duration of treatment, complexity of treatment, and health care staff infection risk.2020 Day AT, Sher DJ, Lee RC, et al. Head and neck oncology during the COVID-19 pandemic: Reconsidering traditional treatment paradigms in light of new surgical and other multilevel risks. Oral Oncol 2020;105:104684 4646 De Felice F, Polimeni A, Tombolini V. The impact of Coronavirus (COVID-19) on head and neck cancer patients' care. Radiother Oncol 2020;147:84-85 Evaluating more complex cases in multidisciplinary conferences is recommended,1919 Bann DV, Patel VA, Saadi R, et al. Impact ofcoronavirus (COVID-19) on otolaryngologic surgery: Brief commentary. Head Neck 2020; 42(06):1227-1234 4040 Ansarin M. Surgical management of head and neck tumours during the SARS-CoV (COVID-19) pandemic. Acta Otorhinolaryngol Ital 2020;40(02):87-89 as there is no simple guideline on how to best postpone treatment.2121 Chaves ALF, Castro AF, Marta GN, et al. Emergency changes in international guidelines on treatment for head and neck cancer patients during the COVID-19 pandemic. Oral Oncol 2020; 107:104734 For instance, there was a report of an immunodeficient patient with tongue squamous cell carcinoma, in which case it was decided to keep track of the lesion size through photos and only operate after the pandemic.1111 Civantos AM, Carey RM, Lichtenstein GR, Lukens JN, Cohen RB, Rassekh CH. Care of immunocompromised patients with head and neck cancer during the COVID-19 pandemic: Two challenging and informative clinical cases. Head Neck 2020;42(06):1131-1136 Despite the decision taken, it is recommended to monitor and reevaluate the patients, if possible through telemedicine services, every 30 days.1919 Bann DV, Patel VA, Saadi R, et al. Impact ofcoronavirus (COVID-19) on otolaryngologic surgery: Brief commentary. Head Neck 2020; 42(06):1227-1234 4343 Cai YC, Wang W, Li C, et al. Treating head and neck tumors during the SARS-CoV-2 epidemic, 2019 to 2020: Sichuan Cancer Hospital. Head Neck 2020;42(06):1153-1158 4646 De Felice F, Polimeni A, Tombolini V. The impact of Coronavirus (COVID-19) on head and neck cancer patients' care. Radiother Oncol 2020;147:84-85
Endoscopic Examinations
The upper airway endoscopy is a very important diagnostic tool for the otolaryngologist physician. Nonetheless, during this procedure, there is a high risk of SARS-CoV-2 transmission, specially via aerosolization.3232 Kowalski LP, Sanabria A, Ridge JA, et al. COVID-19 pandemic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practice. Head Neck 2020;42(06): 1259-1267 For this reason, it consists of an occupational hazard to the professionals involved in this examination. Moreover, 11 of the 18 papers that mentioned endoscopic examinations explicitly suggested postponing the procedure unless it is considered critically necessary for the medical condition of the patients. Indications of urgent need endoscopies are, for instance, hemoptysis; airway compromise; odynophagia that limits hydration and nutrition; and malignant conditions.3636 Rameau A, Young VN, Amin MR, Sulica L. Flexible Laryngoscopy and COVID-19. Otolaryngol Neck Surg 2020 Alternatives, such as CT, ultrasound, and X-ray, should be considered for other cases, depending on the diagnostic hypothesis.2222 Hennessy M, Bann DV, Patel VA, et al. Commentary on the management of total laryngectomy patients during the COVID19 pandemic. Head Neck 2020;42(06):1137-1143 3636 Rameau A, Young VN, Amin MR, Sulica L. Flexible Laryngoscopy and COVID-19. Otolaryngol Neck Surg 2020
An aspect of remarkable relevance is the PPE that should be used. Chan et al published the Hong Kong recommendations regarding PPE use.3131 Chan JYK, Tsang RKY, Yeung KW, et al. There is no routine head and neck exam during the COVID-19 pandemic. Head Neck 2020; 42(06):1235-1239 This guidance is especially valuable because of the SARS-CoV-1 experience of this country, and it endorses the use of N95, isolation gown, gloves, and face shield for the procedures in the endoscopy room. Powered air-purifying respirators were also recommended, despite it is being cumbersome to use.2525 Givi B, Schiff BA, Chinn SB, et al. Safety Recommendations for Evaluation and Surgery of the Head and Neck During the COVID19 Pandemic. JAMA Otolaryngol Neck Surg 2020 3030 Vukkadala N, Qian ZJ, Holsinger FC, Patel ZM, Rosenthal E. COVID. 19 and the Otolaryngologist: Preliminary Evidence-Based Review. Laryngoscope 2020 3232 Kowalski LP, Sanabria A, Ridge JA, et al. COVID-19 pandemic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practice. Head Neck 2020;42(06): 1259-1267 The use of PPE for endoscopic examinations should be mandatory until the coronavirus pandemic is over.
Tracheostomy
Tracheostomy is one of the most performed procedures in emergency facilities all around the world, especially in trauma units for desobstruction of respiratory tract. However, it became a complex subject in the COVID-19 pandemic, once it easily contaminates health workers and surgical centers at a greater degree than other surgeries that do not require direct contact with mucosa. One health care center radically reduced tracheostomies done on patients with positive PCR for COVID-19 and without airway obstruction, once there was no extra benefit from intubation.3030 Vukkadala N, Qian ZJ, Holsinger FC, Patel ZM, Rosenthal E. COVID. 19 and the Otolaryngologist: Preliminary Evidence-Based Review. Laryngoscope 2020 Some articles advise to avoid the use chlorhexidine for antisepsia, once it is not as effective as materials with peroxide hydrogen and ethanol included.4747 Zimmermann M, Nkenke E. Approaches to the management of patients in oral and maxillofacial surgery during COVID-19 pandemic. J Craniomaxillofac Surg 2020;48(05):521-526
A complete protocol on how to perform a secure tracheostomy can use the mnemonic CORONA to divide the procedure in 4 steps.4848 Pichi B, Mazzola F, Bonsembiante A, et al. CORONA-steps for tracheotomy in COVID-19 patients: A staff-safe method for airway management. Oral Oncol 2020;105:104682 C for covering, as in use of cap, shoe covers, mask (FFP3 if possible), goggles, face shield, gown, gloves, and surgical hood; OR standing for operation room setting: a negative pressure room, with closed doors and window, fewer nurses and doctors, who should be experienced, to optimize surgical time; O standing for open the trachea: apply a deep neuromuscular blockade to avoid swallowing and cough reflexes,3030 Vukkadala N, Qian ZJ, Holsinger FC, Patel ZM, Rosenthal E. COVID. 19 and the Otolaryngologist: Preliminary Evidence-Based Review. Laryngoscope 2020 push the tube as caudally as possible to avoid cuff breach and huper-inflate the tube cuff to form airway isolation; and NA standing for nursing and airway management, that is, performing safe suction of secretions, checking cuff-pressure regularly, and closing wound as soon as possible.
Transportation of patients inside the hospital facility and transfer from OR and intensive care unit (ICU) have to be as secure as possible, and it is advisable that the elevator used for SARS-CoV-2 patients is exclusive to them and all halls used in transfer should be closed 30 minutes4949 BroderickD,KyzasP,SandersK,SawyerrA,KatreC,VassiliouL.Surgical tracheostomies in Covid-19 patients: important considerations and the "5Ts" of safety. Br J Oral Maxillofac Surg 2020;58(05):585-589 after transportation, so that proper disinfection can occur.
Telemedicine Use
With the postponement of most consultation and evaluations, a resource that started to gain notice is the use of telemedicine for regular attendances. Online consultations can reduce health system pressure by offering patient recommendations and evaluating situations regarding the need to go to a hospital. Furthermore, telemedicine reduces the risk of infection for the patient and staff, which comes in hand especially for head and neck interventions. It also allows health care workers to discuss cases without having risk of close contact contamination. More than half of the articles presented in the pool recommended the use of telemedicine, with 15 of those specifying the use for triage, routine consults, and revaluation, which shows the increased demand of this resource in different specialities. Some of them also suggest specific applications—such as Zoom, All American Platform, and WeChat—for use, which could be useful for centers with the intent to start the use of telemedicine.4343 Cai YC, Wang W, Li C, et al. Treating head and neck tumors during the SARS-CoV-2 epidemic, 2019 to 2020: Sichuan Cancer Hospital. Head Neck 2020;42(06):1153-1158 5050 Shokri T, Lighthall JG. Telemedicine in the Era of the COVID-19 Pandemic: Implications in Facial Plastic Surgery. Facial Plast Surg Aesthet Med 2020;22(03):155-156
With the increase of cases and demand of health services, it is recommended that each center evaluates its resources and considers the remodeling of attendance via telemedicine as a way to accommodate mild and moderate cases.
Final Comments
Head and neck surgeons and othorhynolaryngologis are very exposed to COVID-19 transmission during their practice, even if not dealing specifically with the disease. The use of adequate PPE (N95 mask or PAPR) with complete gown in aerosol-producing procedures should become mandatory until there is control of the epidemy, that is, vacine or effective antiviral drugs. Endoscopic exams should only be performed if their result may change the patient's treatment; otherwise, patient's evaluation should be restricted to clinical exam. Evaluation of the COVID-19 status of all inpatients, especially surgery patients, should be performed to acess transmission risk. Cancer should be treated, and each case should be assessed individually. Tracheostomies should be performed with extreme caution and the cuff should be always insufflated below the opening area. Telemedicine can help reduce hospital and outpatient visits. All the recommendations should become standard as long as there is no treatment or vaccine for the SARS-CoV-2.
References
-
1Coronavirus disease. COVID-19. Situation Report 2019;51: 2020Mar.
-
2Coronavirus disease (COVID-19) Situation Report-127. 2020
-
3Zangrillo A, Beretta L, Silvani P, et al. Fast reshaping of intensive care unit facilities in a large metropolitan hospital in Milan, Italy: facing the COVID-19 pandemic emergency. Crit Care Resusc 2020
-
4Zheng MH, Boni L, Fingerhut A. Minimally Invasive Surgery and the Novel Coronavirus Outbreak: Lessons Learned in China and Italy. Ann Surg 2020;272(01):e5-e6
-
5Hu XH, Niu WB, Zhang JF, et al. [Treatment strategies for colorectal cancer patients in tumor hospitals under the background of corona virus disease 2019]. Zhonghua Wei Chang Wai Ke Za Zhi 2020;23(03):201-208
-
6Zou J, Yu H, Song D, Niu J, Yang H. Advice on Standardized Diagnosis and Treatment for Spinal Diseases during the Coronavirus Disease 2019 Pandemic. Asian Spine J 2020;14(02):258-263
-
7Di Saverio S, Pata F, Gallo G, et al. Coronavirus pandemic and Colorectal surgery: practical advicebasedon the Italian experience. Color Dis 2020
-
8Zhao L, Zhang L, Liu JW, Yang ZF, Shen WZ, Li XR. [The treatment proposal for the patients with breast diseases in the central epidemic area of 2019 coronavirus disease]. Zhonghua Wai Ke Za Zhi 2020;58(05):331-336
-
9Chew M-H, Koh FH, Ng KH. A call to arms: a perspective of safe general surgery in Singapore during the COVID-19 pandemic. Singapore Med J 2020
-
10Gandhi M, Yokoe DS, Havlir DV. Asymptomatic Transmission, the Achilles' Heel of Current Strategies to Control Covid-19. N Engl J Med 2020;382(22):2158-2160
-
11Civantos AM, Carey RM, Lichtenstein GR, Lukens JN, Cohen RB, Rassekh CH. Care of immunocompromised patients with head and neck cancer during the COVID-19 pandemic: Two challenging and informative clinical cases. Head Neck 2020;42(06):1131-1136
-
12Hojaij FC, Chinelatto LA, Boog GHP, Kasmirski JA, Lopes JVZ, Sacramento FM. Surgical Practice in the Current COVID-19 Pandemic: A Rapid Systematic Review. Clinics (São Paulo) 2020;75: e1923
-
13Tysome JR, Bhutta MF. COVID-19: Protecting our ENT Workforce. Clin Otolaryngol 2020;45(03):311-312
-
14Crossley J, Clark C, Brody F, Maxwell JH. Surgical Considerations for an Awake Tracheotomy During the COVID-19 Pandemic. J Laparoendosc Adv Surg Tech A 2020;30(05):477-480
-
15Kligerman MP, Vukkadala N, Tsang RKY, et al. Managing head and neck cancer patients with tracheostomy or laryngectomy during the COVID-19 pandemic. Head Neck 2020;42(06):1209-1213
-
16Schultz P, Morvan JB, Fakhry N, et al; French Society of Otorhinolaryngology, Head, Neck Surgery (SFORL); French Society of Head, Neck Carcinology (SFCCF). French consensus regarding precautions during tracheostomy and post-tracheostomy care in the context of COVID-19 pandemic. Eur Ann Otorhinolaryngol Head Neck Dis 2020;137(03):167-169
-
17Cheng X, Liu J, Li N, et al. Otolaryngology Providers Must Be Alert for Patients with Mild and Asymptomatic COVID-19. Vol. 162, Otolaryngology - Head and Neck Surgery (United States). SAGE Publications Inc.; 2020:809-10
-
18Saadi RA, Bann DV, Patel VA, Goldenberg D, May J, Isildak H. A Commentary on Safety Precautions for Otologic Surgery during the COVID-19 Pandemic. Vol. 162, Otolaryngology - Head and Neck Surgery (United States). SAGE Publications Inc.; 2020. p. 797-9.
-
19Bann DV, Patel VA, Saadi R, et al. Impact ofcoronavirus (COVID-19) on otolaryngologic surgery: Brief commentary. Head Neck 2020; 42(06):1227-1234
-
20Day AT, Sher DJ, Lee RC, et al. Head and neck oncology during the COVID-19 pandemic: Reconsidering traditional treatment paradigms in light of new surgical and other multilevel risks. Oral Oncol 2020;105:104684
-
21Chaves ALF, Castro AF, Marta GN, et al. Emergency changes in international guidelines on treatment for head and neck cancer patients during the COVID-19 pandemic. Oral Oncol 2020; 107:104734
-
22Hennessy M, Bann DV, Patel VA, et al. Commentary on the management of total laryngectomy patients during the COVID19 pandemic. Head Neck 2020;42(06):1137-1143
-
23Fakhry N, Schultz P, Morinière S, et al; French Society of Otorhinolaryngology, Head and Neck Surgery (SFORL); French Society of Head and Neck Carcinology (SFCCF). French consensus on management of head and neck cancer surgery during COVID-19 pandemic. Eur Ann Otorhinolaryngol Head Neck Dis 2020;137 (03):159-160
-
24Frauenfelder C, Butler C, Hartley B, et al. Practical insights for paediatric otolaryngology surgical cases and performing microlaryngobronchoscopy during the COVID-19 pandemic. Int J Pediatr Otorhinolaryngol 2020;134:110030
-
25Givi B, Schiff BA, Chinn SB, et al. Safety Recommendations for Evaluation and Surgery of the Head and Neck During the COVID19 Pandemic. JAMA Otolaryngol Neck Surg 2020
-
26Hsieh TY, Dedhia RD, Chiao W, et al. A Guide to Facial Trauma Triage and Precautions in the COVID-19 Pandemic. Facial Plast Surg Aesthet Med 2020;22(03):164-169
-
27Krajewska J, Krajewski W, Zub K, Zatonski T. COVID-19 in otolaryngologist practice: a review of current knowledge. Eur Arch Otorhinolaryngol 2020;277(07):1885-1897
-
28Leboulanger N, Sagardoy T, Akkari M, et al; French Association of Pediatric Otorhinolaryngology (AFOP); French Society of Otorhinolaryngology; Head, Neck Surgery (SFORL); Guidelines of the French Association of Pediatric Otorhinolaryngology (AFOP) and French Society of Otorhinolaryngology (SFORL). COVID-19 and ENT Pediatric otolaryngology during the COVID-19 pandemic. Eur Ann Otorhinolaryngol Head Neck Dis 2020;137(03): 177-181
-
29Topf MC, Shenson JA, Holsinger FC, et al. Framework for prioritizing head and neck surgery during the COVID-19 pandemic. Head Neck 2020;42(06):1159-1167
-
30Vukkadala N, Qian ZJ, Holsinger FC, Patel ZM, Rosenthal E. COVID. 19 and the Otolaryngologist: Preliminary Evidence-Based Review. Laryngoscope 2020
-
31Chan JYK, Tsang RKY, Yeung KW, et al. There is no routine head and neck exam during the COVID-19 pandemic. Head Neck 2020; 42(06):1235-1239
-
32Kowalski LP, Sanabria A, Ridge JA, et al. COVID-19 pandemic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practice. Head Neck 2020;42(06): 1259-1267
-
33Lu D, Wang H, Yu R, Yang H, Zhao Y. Integrated infection control strategy to minimize nosocomial infection of coronavirus disease 2019 among ENT healthcare workers. J Hosp Infect 2020;104(04): 454-455
-
34Lüers J-C, Klußmann JP, Guntinas-Lichius O. Die COVID-19-Pandemie und das HNO-Fachgebiet: Worauf kommt es aktuell an? Laryngorhinootologie 2020;99(05):287-291
-
35Parikh SR, Bly RA, Bonilla-Velez J, et al. Pediatric Otolaryngology Divisional and Institutional Preparatory Response at Seattle Children's Hospital after COVID-19 Regional Exposure. Otolaryngol Neck Surg 2020
-
36Rameau A, Young VN, Amin MR, Sulica L. Flexible Laryngoscopy and COVID-19. Otolaryngol Neck Surg 2020
-
37Xu K, Lai X, Liu Z. Suggestions on the prevention of COVID-19 for health care workers in department of otorhinolaryngology head and neck surgery. World J Otorhinolaryngol -. Head Neck Surg 2020
-
38Balakrishnan K, Schechtman S, Hogikyan ND, Teoh AYB, McGrath B, Brenner MJ. COVID-19 Pandemic: What Every Otolaryngologist-Head and Neck Surgeon Needs to Know for Safe Airway Management. Otolaryngol Neck Surg 2020
-
39Kulcsar MA, Montenegro FL, Arap SS, Tavares MR, Kowalski LP. High Risk of COVID-19 Infection for Head and Neck Surgeons. Int Arch Otorhinolaryngol 2020;24(02):e129-e130
-
40Ansarin M. Surgical management of head and neck tumours during the SARS-CoV (COVID-19) pandemic. Acta Otorhinolaryngol Ital 2020;40(02):87-89
-
41Liang W, Liang H, Ou L, et al; China Medical Treatment Expert Group for COVID-19. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Intern Med 2020
-
42Sun Y, Hu YJ, Xiao HJ. [Suggestions for emergency operation of otorhinolaryngology head and neck during the period of prevention and control of 2019 novel coronavirus]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2020;55(04):322-325
-
43Cai YC, Wang W, Li C, et al. Treating head and neck tumors during the SARS-CoV-2 epidemic, 2019 to 2020: Sichuan Cancer Hospital. Head Neck 2020;42(06):1153-1158
-
44Murphy CT, Galloway TJ, Handorf EA, et al. Survival Impact of Increasing Time to Treatment Initiation for Patients With Head and Neck Cancer in the United States. J Clin Oncol 2016;34(02): 169-178
-
45Kowalski LP, Carvalho AL. Influence of time delay and clinical upstaging in the prognosis of head and neck cancer. Oral Oncol 2001;37(01):94-98
-
46De Felice F, Polimeni A, Tombolini V. The impact of Coronavirus (COVID-19) on head and neck cancer patients' care. Radiother Oncol 2020;147:84-85
-
47Zimmermann M, Nkenke E. Approaches to the management of patients in oral and maxillofacial surgery during COVID-19 pandemic. J Craniomaxillofac Surg 2020;48(05):521-526
-
48Pichi B, Mazzola F, Bonsembiante A, et al. CORONA-steps for tracheotomy in COVID-19 patients: A staff-safe method for airway management. Oral Oncol 2020;105:104682
-
49BroderickD,KyzasP,SandersK,SawyerrA,KatreC,VassiliouL.Surgical tracheostomies in Covid-19 patients: important considerations and the "5Ts" of safety. Br J Oral Maxillofac Surg 2020;58(05):585-589
-
50Shokri T, Lighthall JG. Telemedicine in the Era of the COVID-19 Pandemic: Implications in Facial Plastic Surgery. Facial Plast Surg Aesthet Med 2020;22(03):155-156
Publication Dates
-
Publication in this collection
16 Nov 2020 -
Date of issue
Oct-Dec 2020
History
-
Received
03 June 2020 -
Accepted
25 June 2020