Abstracts
BACKGROUND:
Cardiac vagal index (CVI) is supposedly higher in athletes and may differ between sports and/or between field positions.
OBJECTIVE:
To compare CVI: a) between elite football players vs. non-athletes and b) according to five football positions.
METHOD:
242 football players of the first Brazilian/Angolan division were divided in five positions (N): goalkeepers (17), defenders (44), wingers (34), midfielders (87) and forwarders (60) and compared with 303 age-matched healthy non-athletes. CVI was estimated from a 4-second exercise test by quantifying the ratio of two cardiac cycle durations, before and at the end of a fast unloaded cycling exercise.
RESULTS:
Football players had resting and maximal heart rates of, respectively, 59 and 190 bpm and measured VO2max of 62.2 mL/(kg.min). Players and non-athletes showed similar CVI results (median-[P25-P75]) - 1.63-[1.46-1.84] vs 1.61-[1.41-1.81] (p = 0.22). Wingers tended to have a higher CVI (1.84-[1.60-1.99]), especially when compared to defenders (1.53-[1.41-1.72] (p = 0.01). There was a modest non-physiologically relevant association between VO2max and CVI (r = 0.15).
CONCLUSIONS:
Football players did not differ from non-athletes in CVI; however, among players, wingers were more often vagotonic, which may represent a hemodynamic advantage for match situations, where rapid heart rate transitions and faster oxygen delivery to muscles are required.
KEYWORDS:
Sports; Autonomic nervous system; Heart rate; 4-second exercise test; Parasympathetic activity
FUNDAMENTOS:
O índice vagal cardíaco (IVC) é supostamente maior em atletas e pode diferir entre esportes e dentro do mesmo esporte.
OBJETIVO:
Comparar o IVC: a) entre futebolistas e não atletas e b) de acordo com cinco posições do futebol.
MÉTODO:
242 jogadores da primeira divisão brasileira/angolana foram divididos em cinco posições (N): goleiros (17), zagueiros (44), laterais (34), meio-campistas (87) e atacantes (60) e comparados com 303 não-atletas saudáveis da mesma idade. IVC foi estimado a partir do teste de exercício de 4 segundos, quantificando a relação entre as durações de dois ciclos cardíacos - antes e ao final de uma pedalada rápida e sem carga
RESULTADOS:
As frequências cardíacas de repouso e máxima dos futebolistas foram, respectivamente, 59 e 190 bpm e o VO2max de 62,2 mL/(kg.min). Futebolistas e não-atletas mostraram resultados semelhantes de IVC (mediana- [P25-P75]) - 1,63- [1,46-1,84] vs 1,61- [1,41-1,81] (p = 0,22). Os laterais tenderam a ter maior IVC (1,84- [1,60-1,99]), especialmente quando comparados aos defensores (1,53- [1,41-1,72] (p = 0,01). Houve uma modesta associação fisiologicamente irrelevante entre VO2max e IVC (r = 0,15).
CONCLUSÕES:
jogadores da elite do futebol não diferem de não-atletas em IVC; entretanto, entre eles, os alas se mostraram mais frequentemente vagotônicos, o que pode representar uma vantagem hemodinâmica para situações de jogo, onde são necessárias transições rápidas da frequência cardíaca e um aporte mais rápido de oxigênio para os músculos ativos.
PALAVRAS-CHAVE:
esportes; sistema nervoso autônomo; frequência cardíaca; teste de exercício de 4 segundos; atividade parassimpática
INTRODUCTION
Football is arguably the sport with the largest number of players worldwide. Founded in 1904, the Fédération Internationale de Football Association (FIFA) has currently 209 national member associations with more than 260 million registered players.11 Kunz M. 265 million playing football. FIFA Magazine. 2007:10-5. Major tournaments are held in big stadiums and broadcasted live to billions of spectators around the world. There is a considerable body of literature about medical and physiological aspects of football,22 Barnes C, Archer DT, Hogg B, Bush M, Bradley PS. The evolution of physical and technical performance parameters in the English Premier League. Int J Sports Med. 2014;35(13):1095-1100. DOI:10.1055/s-0034-1375695.
https://doi.org/10.1055/s-0034-1375695...
3 Dvorak J, Grimm K, Schmied C, Junge A. Feasibility of precompetition medical assessment at FIFA World Cups for female youth players. Brit J Sports Med. 2012;46(16):1132-3. DOI:10.1136/bjsports-2011-090374
https://doi.org/10.1136/bjsports-2011-09...
4 Reilly T, Bangsbo J, Franks A. Anthropometric and physiological predispositions for elite soccer. J Sport Sci. 2000;18(9):669-83. DOI:10.1080/02640410050120050
https://doi.org/10.1080/0264041005012005...
5 Dvorak J, Kramer EB, Schmied CM, Drezner JA, Zideman D, Patricios J, et al. The FIFA medical emergency bag and FIFA 11 steps to prevent sudden cardiac death: setting a global standard and promoting consistent football field emergency care. Brit J Sports Med. 2013;47(18):1199-202. DOI:10.1136/bjsports-2013-092767.
https://doi.org/10.1136/bjsports-2013-09...
6 Bessem B, de Bruijn MC, Nieuwland W. The ECG of high-level junior soccer players: comparing the ESC vs the Seattle criteria. Brit J Sports Med. 2015;49(15):1000-6. DPO:10.1136/bjsports-2013-093245
7 Signorelli GR, Perim RR, Santos TM, Araujo CG. A pre-season comparison of aerobic fitness and flexibility of younger and older professional soccer players. Int J Sports Med. 2012;33(11):867-72. DOI:10.1055/s-0032-1311597.
https://doi.org/10.1055/s-0032-1311597...
8 Clemente FM, Couceiro MS, Martins FM, Ivanova MO, Mendes R. Activity profiles of soccer players during the 2010 world cup. J Hum Kinet. 2013;38:201-11. DOI:10.2478/hukin-2013-0060.
https://doi.org/10.2478/hukin-2013-0060...
-99 Hoppe MW, Slomka M, Baumgart C, Weber H, Freiwald J. Match running performance and success across a season in German Bundesliga soccer teams. Int J Sports Med. 2015;36(7):563-6. DOI:10.1055/s-0034-1398578.
https://doi.org/10.1055/s-0034-1398578...
including data as diverse as sudden death incidence,55 Dvorak J, Kramer EB, Schmied CM, Drezner JA, Zideman D, Patricios J, et al. The FIFA medical emergency bag and FIFA 11 steps to prevent sudden cardiac death: setting a global standard and promoting consistent football field emergency care. Brit J Sports Med. 2013;47(18):1199-202. DOI:10.1136/bjsports-2013-092767.
https://doi.org/10.1136/bjsports-2013-09...
clinical data66 Bessem B, de Bruijn MC, Nieuwland W. The ECG of high-level junior soccer players: comparing the ESC vs the Seattle criteria. Brit J Sports Med. 2015;49(15):1000-6. DPO:10.1136/bjsports-2013-093245 and physiological testing.77 Signorelli GR, Perim RR, Santos TM, Araujo CG. A pre-season comparison of aerobic fitness and flexibility of younger and older professional soccer players. Int J Sports Med. 2012;33(11):867-72. DOI:10.1055/s-0032-1311597.
https://doi.org/10.1055/s-0032-1311597...
8 Clemente FM, Couceiro MS, Martins FM, Ivanova MO, Mendes R. Activity profiles of soccer players during the 2010 world cup. J Hum Kinet. 2013;38:201-11. DOI:10.2478/hukin-2013-0060.
https://doi.org/10.2478/hukin-2013-0060...
-99 Hoppe MW, Slomka M, Baumgart C, Weber H, Freiwald J. Match running performance and success across a season in German Bundesliga soccer teams. Int J Sports Med. 2015;36(7):563-6. DOI:10.1055/s-0034-1398578.
https://doi.org/10.1055/s-0034-1398578...
Physiologically speaking, football is an mixed anaerobic-aerobic or intermittent exercise, typically calling for an all-out effort sprint once every 90 seconds and high-intensity efforts every 30 seconds for each player, although substantial differences are to be expected according to player’s style/ability and position/role in the field.44 Reilly T, Bangsbo J, Franks A. Anthropometric and physiological predispositions for elite soccer. J Sport Sci. 2000;18(9):669-83. DOI:10.1080/02640410050120050
https://doi.org/10.1080/0264041005012005...
Because “athlete” is a quite unspecific label in terms of actual physical fitness (aerobic fitness, flexibility, muscle strength/power, balance and body composition), encompassing subjects with remarkably different physical and physiological profiles,1010 Araujo CG, Scharhag J. Athlete: a working definition for medical and health sciences research. Scand J Med Sci Sports. 2016;26(1):4-7. DOI:10.1111/sms.12632
https://doi.org/10.1111/sms.12632...
significant controversy exists regarding cardiac autonomic modulation in “athletes”.1111 Dixon EM, Kamath MV, McCartney N, Fallen EL. Neural regulation of heart rate variability in endurance athletes and sedentary controls. Cardiovasc Res. 1992;26(7):713-9.
12 Araujo CG, Nóbrega AC, Castro CL. Vagal activity: effect of age, sex and physical activity pattern. Braz J Med Biol Res. 1989;22(7):909-11.
13 Boyett MR, D'Souza A, Zhang H, Morris GM, Dobrzynski H, Monfredi O. Viewpoint: is the resting bradycardia in athletes the result of remodeling of the sinoatrial node rather than high vagal tone? J Appl Physiol (1985). 2013;114(9):1351-5. DOI:10.1152/japplphysiol.01126.2012
https://doi.org/10.1152/japplphysiol.011...
14 Coote JH, White MJ. CrossTalk proposal: bradycardia in the trained athlete is attributable to high vagal tone. J Physiol. 2015;593(8):1745-7. DOI:10.1113/jphysiol.2014.284364
https://doi.org/10.1113/jphysiol.2014.28...
15 Aubert AE, Seps B, Beckers F. Heart rate variability in athletes. Sports Med. 2003;33(12):889-919.-1616 Hettinga FJ, Monden PG, van Meeteren NL, Daanen HA. Cardiac acceleration at the onset of exercise: a potential parameter for monitoring progress during physical training in sports and rehabilitation. Sports Med. 2014;44(5):591-602. DOI:10.1007/s40279-013-0141-y
https://doi.org/10.1007/s40279-013-0141-...
While some studies describe a tendency to a higher cardiac vagal modulation in athletes,1111 Dixon EM, Kamath MV, McCartney N, Fallen EL. Neural regulation of heart rate variability in endurance athletes and sedentary controls. Cardiovasc Res. 1992;26(7):713-9.,1212 Araujo CG, Nóbrega AC, Castro CL. Vagal activity: effect of age, sex and physical activity pattern. Braz J Med Biol Res. 1989;22(7):909-11.,1717 Abad CC, do Nascimento AM, Gil S, Kobal R, Loturco I, Nakamura FY, et al. Cardiac autonomic control in high level Brazilian power and endurance track-and-field athletes. Int J Sports Med. 2014;35(9):772-8. DOI:10.1055/s-0033-1363268.
https://doi.org/10.1055/s-0033-1363268...
18 Carter JB, Banister EW, Blaber AP. Effect of endurance exercise on autonomic control of heart rate. Sports Med. 2003;33(1):33-46.-1919 Proietti R, di Fronso S, Pereira LA, Bortoli L, Robazza C, Nakamura FY, et al. Heart rate variability discriminates competitive levels in professional soccer players. J Strength Cond Res. 2017;31(6):1719-25. DOI:10.1519/JSC.0000000000001795
https://doi.org/10.1519/JSC.000000000000...
this has not been uniformly confirmed by others;1313 Boyett MR, D'Souza A, Zhang H, Morris GM, Dobrzynski H, Monfredi O. Viewpoint: is the resting bradycardia in athletes the result of remodeling of the sinoatrial node rather than high vagal tone? J Appl Physiol (1985). 2013;114(9):1351-5. DOI:10.1152/japplphysiol.01126.2012
https://doi.org/10.1152/japplphysiol.011...
14 Coote JH, White MJ. CrossTalk proposal: bradycardia in the trained athlete is attributable to high vagal tone. J Physiol. 2015;593(8):1745-7. DOI:10.1113/jphysiol.2014.284364
https://doi.org/10.1113/jphysiol.2014.28...
-1515 Aubert AE, Seps B, Beckers F. Heart rate variability in athletes. Sports Med. 2003;33(12):889-919. indeed, this controversy is not surprising, as it is possible that distinct moments of testing along the competitive season and, most importantly, differences between sport modalities or specializations within the same modality, could be the reason for these discrepancies.1212 Araujo CG, Nóbrega AC, Castro CL. Vagal activity: effect of age, sex and physical activity pattern. Braz J Med Biol Res. 1989;22(7):909-11.,2020 Michailidis Y. Stress hormonal analysis in elite soccer players during a season. J Sport Health Sci. 2014;3:279-83. DOI:10.1016/j.jshs.2014.03.016
https://doi.org/10.1016/j.jshs.2014.03.0...
Within this context, a protocol for routine pre-participation screening of elite athletes repeated in several consecutive years would provide a unique opportunity to study the behavior of some of these variables. An ideal scenario would be to have all athletes uniformly assessed at the same pre-season time, when more comparable information regarding physiology, morphology and clinical data could be collected. More specifically, as previously suggested by researchers44 Reilly T, Bangsbo J, Franks A. Anthropometric and physiological predispositions for elite soccer. J Sport Sci. 2000;18(9):669-83. DOI:10.1080/02640410050120050
https://doi.org/10.1080/0264041005012005...
and noted by specialized sport news reporters,2121 Wilson J. The question: why is full-back the most important position on the pitch? The Guardian. 2009; 2009/03/25. it is probable that among elite football players , the wingers are the ones presenting physiological advantages, which may include a higher cardiac vagal index (CVI).
The objectives of this study were: a) to compare CVI between male National (Brazil and Angola) elite football players and non-athletes, b) to evaluate if CVI differs according to football’s field position; c) to assess the relationship between CVI with some other major physiological variables in football players and d) to assess CVI’s two-year stability in football players.
MATERIALS AND METHODS
Participants. From 2005 to 2014, 278 adult male elite football players from two teams of Football National First Division of Brazil (Botafogo) and Angola (Santos) visited, at the request of the teams’ physicians, our Sports & Exercise Medicine Center for a comprehensive pre-season medical-functional evaluation comprising: clinical examination, resting electrocardiogram (ECG) & spirometry, kinanthropometric evaluation (somatotyping, flexibility and muscle strength/power) and maximal treadmill cardiopulmonary exercise testing (CPET), under ECG monitoring. All athletes were regularly competing at national and international levels, including some FIFA World Cup participants. All participants of the study read and signed an informed consent form and agreed to participate in the evaluation protocol and in having their data used for scientific purposes. The research protocol follows national and international standards and regulations and was approved by the institutional ethics committee (case # 0166.0.000.399-11).
We included 242 (205 Brazilians and 37 Angolans) players who successfully completed a maximal CPET and a CVI evaluation, during a single visit to our facility: this represents the test sample of the study (table 1). A control sample was obtained from 303 age-matched male healthy non-athlete subjects (HS) evaluated at the same Medical Centre for routine check-ups and/or exercise prescription advice.2222 Araujo CG, Castro CL, Franca JF, Ramos PS. 4-Second exercise test: reference values for ages 18-81 years. Arq Bras Cardiol. 2015;104(5):366-74. DOI:10.5935/abc.20150026
https://doi.org/10.5935/abc.20150026...
Data collection was carried out by five sports & exercise medicine’s physicians along the 10-year period of the study.
Main characteristics of the 242 male elite football players - all group - and by 5 field positions.
In order to evaluate potential CVI differences related to field positions, players were classified as: goalkeepers (n = 17), defenders (n = 44), wing-back or wingers (n = 34), midfielders (n = 87) and forwarders (n = 60). For the main data analysis, each player was entered just once; however, in order to study the stability of CVI measurements separated by a one-year interval, data obtained from 81 players were compared.
The 4-second exercise test (cardiac vagal assessment). A 4-second exercise test (4sET) was performed to quantify the magnitude of heart rate (HR) increase induced by cardiac vagal withdrawal at very beginning of exercise (first four seconds). Initially proposed in 1989,1212 Araujo CG, Nóbrega AC, Castro CL. Vagal activity: effect of age, sex and physical activity pattern. Braz J Med Biol Res. 1989;22(7):909-11. the 4sET consists of cycling against no added resistance from the fifth to the ninth second of a 12-second bout of apnea at total lung capacity. Four consecutive verbal commands were given at each 4-s intervals: (1) inspire as deep and as quickly as possible through the mouth; (2) cycle as fast as possible; (3) stop cycling; (4) breathe naturally. The 4sET has been validated by dual pharmacologic blockade for the assessment of cardiac vagal withdrawal at the onset of exercise2323 Araujo CG, Nobrega AC, Castro CL. Heart rate responses to deep breathing and 4-seconds of exercise before and after pharmacological blockade with atropine and propranolol. Clinical Auton Res. 1992;2(1):35-40.,2424 Nobrega AC, Castro CL, Araujo CG. Relative roles of the sympathetic and parasympathetic systems in the 4-s exercise test. Braz J Med Biol Res. 1990;23(12):1259-62. and has been shown to be highly reliable as assessed by intraclass correlation coefficients from 0.77 to 0.92 in intra- and inter-days studies.2525 Araujo CG, Ricardo DR, Almeida MB. Intra and interdays reliability of the 4-second exercise test. Rev Bras Med Esporte. 2003;9(5):293-8. DOI:10.1590/S1517-86922003000500005
https://doi.org/10.1590/S1517-8692200300...
It is worth noting that since the validation of the 4sET two decades ago,2323 Araujo CG, Nobrega AC, Castro CL. Heart rate responses to deep breathing and 4-seconds of exercise before and after pharmacological blockade with atropine and propranolol. Clinical Auton Res. 1992;2(1):35-40. it has been widely used in various physiological and clinical investigations.2626 Knopfli BH, Bar-Or O. Vagal activity and airway response to ipratropium bromide before and after exercise in ambient and cold conditions in healthy cross-country runners. Clin J Sports Med. 1999;9(3):170-6.
27 Teixeira FP, Ricardo DR, Castro CLB, Araújo CGS. Evaluating cardiac vagal activity on a conventional electrocardiogram. Arq Bras Cardiol. 2007;88(4):373-8. DOI:10.1590/S0066-782X2007000400002
https://doi.org/10.1590/S0066-782X200700...
28 Millar PJ, MacDonald MJ, Bray SR, McCartney N. Isometric handgrip exercise improves acute neurocardiac regulation. Eur J Appl Physiol. 2009;107(5):509-15. DOI:10.1007/s00421-009-1142-2
https://doi.org/10.1007/s00421-009-1142-...
-2929 Stang J, Couto M, Stensrud T, Mowinckel P, Moreira A, Carlsen KH. Assessment of parasympathetic activity in athletes: comparing two different methods. Med Sci Sports Exerc. 2016;48(2):316-22. DOI:10.1249/MSS.0000000000000769
https://doi.org/10.1249/MSS.000000000000...
The 4sET protocol has fully been described elsewhere.2222 Araujo CG, Castro CL, Franca JF, Ramos PS. 4-Second exercise test: reference values for ages 18-81 years. Arq Bras Cardiol. 2015;104(5):366-74. DOI:10.5935/abc.20150026
https://doi.org/10.5935/abc.20150026...
,3030 Duarte CV, Araujo CG. Cardiac vagal index does not explain age-independent maximal heart rate. Int J Sports Med. 2013;34(6):502-6. DOI:10.1055/s-0032-1323818.
https://doi.org/10.1055/s-0032-1323818...
,3131 Ricardo DR, Almeida MB, Franklin BA, Araújo CGS. Initial and final exercise heart rate transients: influence of gender, aerobic fitness, and clinical status. Chest. 2005;127(1):318-27. DOI:10.1378/chest.127.1.318
https://doi.org/10.1378/chest.127.1.318...
In brief, the duration of two specific RR intervals were identified and measured at 10 ms resolution in digital ECG tracings (Elite PC, Micromed, Brazil): (a) the longest RR interval (either the interval obtained immediately before the onset of exercise or the first one after the onset) and (b) the shortest RR interval during exercise (generally, the last one). A cardiac vagal index (CVI) is, per definition, the ratio between these two RR intervals. Thus, the CVI is a dimensionless variable and represents HR variation induced by the full inspiration (decrease in heart rate) followed by the onset of fast cycling exercise (increase in heart rate), reflecting the magnitude of cardiac vagal modulation. Based on a large sample of healthy subjects,2222 Araujo CG, Castro CL, Franca JF, Ramos PS. 4-Second exercise test: reference values for ages 18-81 years. Arq Bras Cardiol. 2015;104(5):366-74. DOI:10.5935/abc.20150026
https://doi.org/10.5935/abc.20150026...
a CVI value ≥ 2 (a doubling or more of the heart rate) has been empirically considered to reflect a vagotonic state. Two 4sET maneuvers were performed and the highest CVI chosen as representative of the player’s result.
Maximal cardiopulmonary exercise testing. A maximal treadmill CPET was performed, following a ramp running protocol, in which, after a one-minute walk at 5.5 km/h, the speed was increased to 8 km/h e thereafter at 0.1 km/h increments at each 7.5 s (0.8 km/h increment per minute) until volitional fatigue under strong verbal encouragement. The following physiological data were selected to assess the association with CVI: (a) resting HR obtained from a supine 12-lead digital ECG; (b); (b) maximal HR, read from the digital ECG tracings (average value from last 7s of exercise) and (c) maximum VO2 derived from the average of the last six 10-second readings obtained by expired ventilatory gas analysis (VO2000 - MedGraphics, USA).
Statistical analysis. Standard descriptive statistics were calculated for all relevant variables. The Shapiro-Wilk test showed that CVI had a non-gaussian distribution, leading to inferential analyses through a Mann-Whitney test (unpaired two-group analysis), or a Wilcoxon test (paired one-group analysis), or a Kruskal-Wallis ANOVA (more than two group analysis) as appropriate. A Dunn post-hoc test was employed for all pair comparisons, as required. The Chi-square statistic was used for comparing frequency of vagotonic (i.e. CVI > 2) football players according to different field positions and between athletes and non-athletes. Spearman-Rank correlation coefficients were calculated between physiological variables and CVI. Significance level was set at p < 0.05. Statistical analysis was carried out by Prism 6.02 (GraphPad, USA).
RESULTS
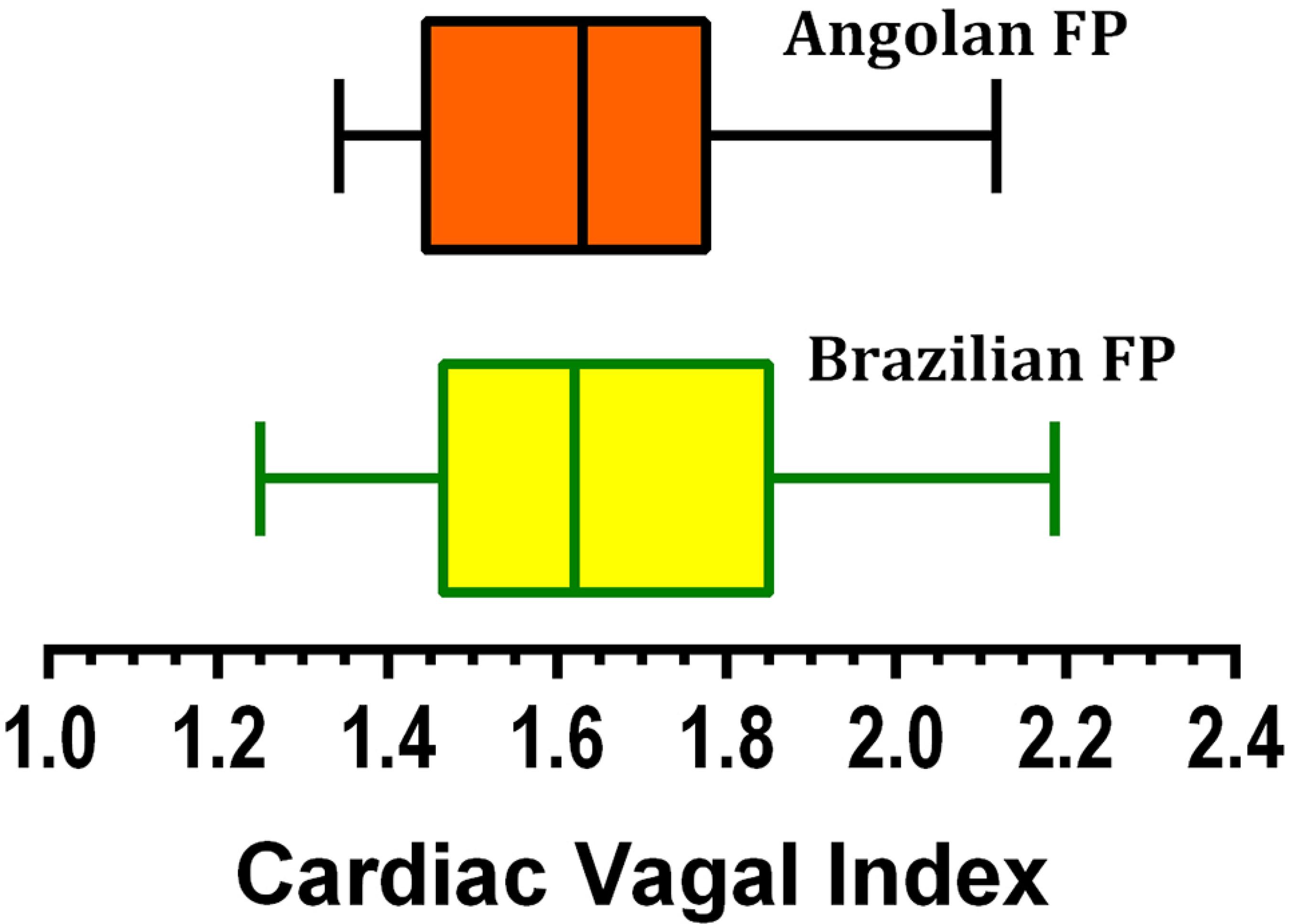
After evaluation, all the football players were found to be medically eligible for competition and training. Differences between Brazilian and Angolans players were minimal with respect to age (24 ± 4 vs 23 ± 3 years) and significant but most likely physiologically irrelevant for body weight (77 ± 8 vs 71 ± 8 kg - p<0.05). CVI (median and [percentiles 25-75]), the main study variable, was similar (p = 0.58) for Brazilian (1.62 [1.46-1.85] vs. Angolan players (1.63 [1.44-1.78], as illustrated in Figure 1. Because of this similarity, the data for Brazilian and Angolan players were combined in a single sample for further analysis. Additionally, there was no difference (p = 0.220) for CVI between football players and age-matched healthy subjects, respectively, 1.625 [1.46-1.84] and 1.633 [1.41-1.81]. Moreover, the proportion of vagotonic cases did not differ between FP and HS (p=0.91).
Comparison of cardiac vagal index (4sET results) for 205 Brazilian and 37 Angolan male elite football players.
When classified according field positions, wingers were significantly (p < 0.05) more vagotonic (CVI median 1.84) than the other four field positions as shown in Figure 2. In fact, the CVI P25 for wingers (1.62) was almost identical to the CVI median values for the other positions, which ranged from 1.51 to 1.65. Goalkeepers, defenders, midfielders and forwarders showed similar CVI results (p > 0.05), although a somewhat larger variability was observed among forwarders. The Chi-square statistic showed that vagotonic state was unevenly distributed between the field positions. A total of 24 (12%) players presented CVI values reflecting a vagotonic state, being largely represented by wingers (35% of them) and to a lesser extent by forwarders (16% of them). It is interesting to note that none of the 17 goalkeepers exceed a CVI of 2 and could be classified as vagotonic.
Comparison of cardiac vagal index (4sET results) for 242 male elite football players according five different field positions.
Regarding the association between CVI and selected physiological variables, (a) no relationship was found between CVI and maximal HR (189 ± 10 bpm - ABREITALICrFECHAITALIC = -0.01; p = 0.82); (b) only a minimal and poorly relevant relationship with VO2 max (62 ± 7 mL.kg-1.min-1 - r = 0.15; p = 0.02), as shown in Figure 3. However, a partial moderate association (p < 0.05) was found between CVI and resting HR (58 ± 9 bpm - ABREITALICrFECHAITALIC = 0.38) as displayed in Figure 4.
Relationship between cardiac vagal index (4sET results) and maximum oxygen uptake in 242 male elite football players
Relationship between cardiac vagal index (4sET results) and maximal heart rate in 242 male elite football players
Analyzing the data from 81 football players who were retested with a one-year interval, no CVI differences (p = 0.52) were found between the first (1.63 [1.42-1.82]) and the second (1.65 [1.45-1.85]), indicating a one-year stability for CVI in adult male elite football players (Figure 5).
Comparison of cardiac vagal index (4sET results) one-year apart in 81 male elite football players.
DISCUSSION
Cardiac vagal modulation assessment. Different methods have been used for the study of cardiac vagal modulation in athletes.1111 Dixon EM, Kamath MV, McCartney N, Fallen EL. Neural regulation of heart rate variability in endurance athletes and sedentary controls. Cardiovasc Res. 1992;26(7):713-9.,3232 Flatt AA, Esco MR. Heart rate variability stabilization in athletes: towards more convenient data acquisition. Clin Physiol Funct Imag. 2016; 36(5):331-6. DOI:10.1111/cpf.12233.
https://doi.org/10.1111/cpf.12233...
,3333 Ueno LM, Moritani T. Effects of long-term exercise training on cardiac autonomic nervous activities and baroreflex sensitivity. Eur J Appl Physiol. 2003;89(2):109-14. DOI:10.1007/s00421-002-0777-z
https://doi.org/10.1007/s00421-002-0777-...
Unfortunately most, if not all, of the studies have presented one or more methodological limitations. In some, the sample size was too small,1111 Dixon EM, Kamath MV, McCartney N, Fallen EL. Neural regulation of heart rate variability in endurance athletes and sedentary controls. Cardiovasc Res. 1992;26(7):713-9.,3434 Martinelli FS, Chacon-Mikahil MP, Martins LE, Lima-Filho EC, Golfetti R, Paschoal MA, et al. Heart rate variability in athletes and nonathletes at rest and during head-up tilt. Braz J Med Biol Res. 2005;38(4):639-47. DOI:10.1590/S0100-879X2005000400019
https://doi.org/10.1590/S0100-879X200500...
while in others3333 Ueno LM, Moritani T. Effects of long-term exercise training on cardiac autonomic nervous activities and baroreflex sensitivity. Eur J Appl Physiol. 2003;89(2):109-14. DOI:10.1007/s00421-002-0777-z
https://doi.org/10.1007/s00421-002-0777-...
,3535 Bonaiuto M, Di Mauro D, Speciale F, Pagano F, Buda D, Vita G, et al. Evaluation of heart rate recovery in relation to playing position in professional soccer players. J Sports Med Phys Fitness. 2012;52(6):583-8. evaluation protocols were not fully or properly standardized or validated. When studying athletes, it is particularly relevant to provide sufficient detail about their competitive profile. This is especially relevant regarding age-group, sport modality and/or level of performance.1010 Araujo CG, Scharhag J. Athlete: a working definition for medical and health sciences research. Scand J Med Sci Sports. 2016;26(1):4-7. DOI:10.1111/sms.12632
https://doi.org/10.1111/sms.12632...
This could be even more relevant for football players, in which, the level of performance varies considerably around the world. In addition, recent limited evidence3636 Oliveira RS, Leicht AS, Bishop D, Barbero-Alvarez JC, Nakamura FY. Seasonal changes in physical performance and heart rate variability in high level futsal players. Int J Sports Med. 2013;34(5):424-30. DOI:10.1055/s-0032-1323720
https://doi.org/10.1055/s-0032-1323720...
suggests that cardiac vagal activity may also vary throughout the season, pointing to the need of this standardization. Moreover, although changes in field positioning in elite football players during the same competitive season are rare, it is possible that the five-category field positions utilized in our study does not precisely reflect the current tactical stage of elite football and maybe some players were misclassified.
Our study considers all the above mentioned methodological constraints and aimed to control or minimize their influences. In contrast, the positive features of this study were: its retrospective analysis with a long period of data acquisition (10 years), allowing us to consolidate a quite large and well-controlled sample of elite players (242), as well as samples of sufficient size per each of the five field positions. Among the 242 players, 81 were reevaluated one year-apart and exhibited stable CVI results. All evaluations of CVI were performed with a pharmacologically validated method and carried out at the same phase of the competitive season under supervision of only five physicians.
We used the 4sET assessment method, a well-established protocol for the evaluation of cardiac vagal modulation. Since its inception in the mid-1980s, it has been applied to more than 7,000 subjects from five to 100 years of age, with various clinical conditions and/or experimental settings.3737 Duarte CV, Araujo CG. Treinamento para disfunção vagal cardíaca com repetições da transição repouso-exercício. Rev Bras Ativ Fis & Saúde. 2013;18(6):688-97. DOI:10.12820/rbafs.v.18n6p688
https://doi.org/10.12820/rbafs.v.18n6p68...
38 Furtado EC, Araujo CG. Cardiac arrhythmias triggered by sudden and dynamic efforts. Ann Noninvasive Electrocardiol 2010;15(2):151-6. DOI:10.1111/j.1542-474X.2010.00356.x
https://doi.org/10.1111/j.1542-474X.2010...
39 Nobrega AC, Araujo CG. Heart rate transient at the onset of active and passive dynamic exercise. Med Sci Sports Exerc. 1993;25(1):37-41.
40 Vianna LC, Oliveira RB, Silva BM, Ricardo DR, Araujo CG. Water intake accelerates post-exercise cardiac vagal reactivation in humans. Eur J Appl Physiol. 2008;102(3):283-8. DOI:10.1007/s00421-007-0584-7
https://doi.org/10.1007/s00421-007-0584-...
-4141 Ricardo DR, Silva BM, Vianna LC, Araujo CG. Cardiac vagal withdrawal and reactivation during repeated rest-exercise transitions. Eur J Appl Physiol. 2010;110:933-42. DOI:10.1007/s00421-010-1555-y
https://doi.org/10.1007/s00421-010-1555-...
As might be expected, 4sET results are only partially related to other proposed autonomic criteria of cardiac vagal modulation, such as resting HR and respiratory sinus arrhythmia,2323 Araujo CG, Nobrega AC, Castro CL. Heart rate responses to deep breathing and 4-seconds of exercise before and after pharmacological blockade with atropine and propranolol. Clinical Auton Res. 1992;2(1):35-40. HR recovery after a maximal exercise testing4242 Mattioli GM, Araujo CG. Association between initial and final transient heart rate responses in exercise testing. Arq Bras Cardiol. 2009;93(2):141-6. DOI:10.1590/S0066-782X2009000800012
https://doi.org/10.1590/S0066-782X200900...
and also to vagal activity measured in other body organs.2929 Stang J, Couto M, Stensrud T, Mowinckel P, Moreira A, Carlsen KH. Assessment of parasympathetic activity in athletes: comparing two different methods. Med Sci Sports Exerc. 2016;48(2):316-22. DOI:10.1249/MSS.0000000000000769
https://doi.org/10.1249/MSS.000000000000...
This partial association is likely due to the fact that, different from other autonomic testing protocols or criteria often used for vagal modulation assessment, 4sET results are exclusively explained by CVI, because the HR transient induced by the 4-second of unloaded cycling is fully abolished by atropine and unaffected by propranolol.2323 Araujo CG, Nobrega AC, Castro CL. Heart rate responses to deep breathing and 4-seconds of exercise before and after pharmacological blockade with atropine and propranolol. Clinical Auton Res. 1992;2(1):35-40.,4343 Lazzoli JK, Soares PP, da Nobrega AC, de Araujo CG. Electrocardiographic criteria for vagotonia-validation with pharmacological parasympathetic blockade in healthy subjects. Int J Cardiol. 2003;87(2-3):231-6. DOI:10.1016/S0167-5273(02)00330-3
https://doi.org/10.1016/S0167-5273(02)00...
Based on this, the 4sET results have also been successfully used as criteria for evaluate ECG signs of vagotonia in healthy subjects4444 Teixeira FP, Ricardo DR, de Castro CL, de Araujo CG. Evaluating cardiac vagal activity on a conventional electrocardiogram. Arq Bras Cardiol. 2007;88(4):378-83. DOI:10.1590/S0066-782X2007000400002.
https://doi.org/10.1590/S0066-782X200700...
and elite athletes.4545 Lazzoli JK, Castro CLB, Nóbrega ACL, Araújo CGS. Accuracy of vagotonia criteria in the 12-lead resting electrocardiogram: analysis with ROC curves. Rev Bras Med Esporte. 2002;8(2):50-8. DOI:10.1590/S1517-86922002000200004.
https://doi.org/10.1590/S1517-8692200200...
Interestingly, similar 4sET results have been obtained with upper or lower-limb cycling,4646 Silva BM, Vianna LC, Oliveira RB, Ricardo DR, Araujo CG. Similar cardiac vagal withdrawal at the onset of arm and leg dynamic exercise. Eur J Appl Physiol. 2008;102(6):695-701. DOI:10.1007/s00421-007-0640-3
https://doi.org/10.1007/s00421-007-0640-...
stationary running4747 Almeida MB, Ricardo DR, Araujo CG. Validation of the 4-second exercise test in the orthostatic position. Arq Bras Cardiol. 2004;83(2):155-9. DOI:10.1590/S0066-782X2004001400007.
https://doi.org/10.1590/S0066-782X200400...
or with active and passive exercises.3939 Nobrega AC, Araujo CG. Heart rate transient at the onset of active and passive dynamic exercise. Med Sci Sports Exerc. 1993;25(1):37-41. Apart from being shown to be reliable,2525 Araujo CG, Ricardo DR, Almeida MB. Intra and interdays reliability of the 4-second exercise test. Rev Bras Med Esporte. 2003;9(5):293-8. DOI:10.1590/S1517-86922003000500005
https://doi.org/10.1590/S1517-8692200300...
the 4sET protocol has been shown to be safe and simple to perform and to produce quantifiable results.2222 Araujo CG, Castro CL, Franca JF, Ramos PS. 4-Second exercise test: reference values for ages 18-81 years. Arq Bras Cardiol. 2015;104(5):366-74. DOI:10.5935/abc.20150026
https://doi.org/10.5935/abc.20150026...
Even more relevant, it remarkably resembles typical conditions occurring in during a football match, in which intermittent and sudden efforts are often seen.44 Reilly T, Bangsbo J, Franks A. Anthropometric and physiological predispositions for elite soccer. J Sport Sci. 2000;18(9):669-83. DOI:10.1080/02640410050120050
https://doi.org/10.1080/0264041005012005...
,99 Hoppe MW, Slomka M, Baumgart C, Weber H, Freiwald J. Match running performance and success across a season in German Bundesliga soccer teams. Int J Sports Med. 2015;36(7):563-6. DOI:10.1055/s-0034-1398578.
https://doi.org/10.1055/s-0034-1398578...
Interpreting the study findings. In a practical scenario, not very much information is available regarding physiological cardiac vagal behavior during “stop-and-go” sport activities. We have previously shown that among the 1988 Brazilian Olympic athletes, those competing in judo and fencing tended to show higher CVI values.1212 Araujo CG, Nóbrega AC, Castro CL. Vagal activity: effect of age, sex and physical activity pattern. Braz J Med Biol Res. 1989;22(7):909-11.
On a theoretical basis, football players, who suddenly and often burst into short spells of high-intensity exercise, would benefit from being able to rapidly increase their HR and consequently cardiac output in order optimize oxygen delivery to the working muscles. This quasi instant response would be beneficial in delaying or diminishing the anaerobic contribution to the total exercise expenditure during the match situations, which, very likely, would represent a metabolic advantage for elite football performance. Along this line of thought, it is interesting to note that the magnitude of withdrawal of the cardiac vagal reflex induced by the 4sET showed a very modest association with VO2 max. Thus, this characteristic appears to be very specific, turning it into an interesting feature to be evaluated in addition to other physiological, morphological and clinical variables.
Because it is a well-established fact that resting HR is mainly under parasympathetic control4848 Robinson BF, Epstein SE, Beiser GD, Braunwald E. Control of heart rate by the autonomic nervous system. Studies in man on the interrelation between baroreceptor mechanisms and exercise. Circ Res. 1966;19(2):400-11. is not surprising that a significant correlation was found between HR and CVI in this study. However, the magnitude of the association is rather modest and did not allow us to precisely estimate one variable from the other. In fact, a previous study has shown that CVI is only partially associated with other and less precise HR measurements, which are believed to be partially dependent upon cardiac vagal modulation.2323 Araujo CG, Nobrega AC, Castro CL. Heart rate responses to deep breathing and 4-seconds of exercise before and after pharmacological blockade with atropine and propranolol. Clinical Auton Res. 1992;2(1):35-40.
Our results show that CVI was similar between elite football players and age-matched non-athletes, corroborating a previous study with Olympic athletes.1212 Araujo CG, Nóbrega AC, Castro CL. Vagal activity: effect of age, sex and physical activity pattern. Braz J Med Biol Res. 1989;22(7):909-11. On the other hand, an interesting finding was a significant difference in CVI according to the different field positions of the players (Figure 2). In the only other study that has analyzed autonomic modulation in players from different positions,3535 Bonaiuto M, Di Mauro D, Speciale F, Pagano F, Buda D, Vita G, et al. Evaluation of heart rate recovery in relation to playing position in professional soccer players. J Sports Med Phys Fitness. 2012;52(6):583-8. some differences were also found, with the goalkeepers presenting lower vagal activity, a finding that was partially confirmed by our results.
The relative CVI stability observed in the 81 players who were retested one-year apart, indication that most of those elite footballers were already at stable levels for CVI at their first evaluation. Notwithstanding, this information should not be extrapolated to other populations or patients with chronic diseases that are submitted to a period of regular training, in whom, substantial improvements from low values can be reached, either measured by 4sET,3737 Duarte CV, Araujo CG. Treinamento para disfunção vagal cardíaca com repetições da transição repouso-exercício. Rev Bras Ativ Fis & Saúde. 2013;18(6):688-97. DOI:10.12820/rbafs.v.18n6p688
https://doi.org/10.12820/rbafs.v.18n6p68...
or by other cardiac vagal indexes.4949 Clarke BF, Ewing DJ. Cardiovascular reflex tests; in the natural history of diabetic autonomic neuropathy. N Y State J Med. 1982;82(6):903-8.
Moving from physiological to psychological aspects, there are considerable data relating sympathetic and parasympathetic activity and attention to task performance.5050 Park G, Vasey MW, Van Bavel JJ, Thayer JF. Cardiac vagal tone is correlated with selective attention to neutral distractors under load. Psychophysiology. 2013;50(4):398-406. DOI:10.1111/psyp.12029.
https://doi.org/10.1111/psyp.12029...
To the best of our knowledge, this interaction has not been studied in elite football players; however, the fact that some forwarders were vagotonic and that none of the goalkeepers presented this profile, could be potentially relevant.
Practical implications. It has long been known44 Reilly T, Bangsbo J, Franks A. Anthropometric and physiological predispositions for elite soccer. J Sport Sci. 2000;18(9):669-83. DOI:10.1080/02640410050120050
https://doi.org/10.1080/0264041005012005...
that wingers are those with an “upper” physiological profile among football players. Indeed, an interesting text entitled “The Question: why is full-back the most important position on the pitch?”, appearing in 2009 in The Guardian,2121 Wilson J. The question: why is full-back the most important position on the pitch? The Guardian. 2009; 2009/03/25. stated that from 1994-2006 every FIFA World Cup has been won by the team with the best pair of attacking full-backs, the wingers as defined in the five-field position system utilized in our study. Nowadays, football players usually run somewhere between 6 to 12 km per 90-min match,22 Barnes C, Archer DT, Hogg B, Bush M, Bradley PS. The evolution of physical and technical performance parameters in the English Premier League. Int J Sports Med. 2014;35(13):1095-1100. DOI:10.1055/s-0034-1375695.
https://doi.org/10.1055/s-0034-1375695...
,88 Clemente FM, Couceiro MS, Martins FM, Ivanova MO, Mendes R. Activity profiles of soccer players during the 2010 world cup. J Hum Kinet. 2013;38:201-11. DOI:10.2478/hukin-2013-0060.
https://doi.org/10.2478/hukin-2013-0060...
,99 Hoppe MW, Slomka M, Baumgart C, Weber H, Freiwald J. Match running performance and success across a season in German Bundesliga soccer teams. Int J Sports Med. 2015;36(7):563-6. DOI:10.1055/s-0034-1398578.
https://doi.org/10.1055/s-0034-1398578...
but wingers, with a dual defense-attack role, are likely to be those who cover the largest part of the field of play and for whom more stop-and-go actions are expected to occur during the match.44 Reilly T, Bangsbo J, Franks A. Anthropometric and physiological predispositions for elite soccer. J Sport Sci. 2000;18(9):669-83. DOI:10.1080/02640410050120050
https://doi.org/10.1080/0264041005012005...
This practical and empirical observation corroborates our finding that the wingers are more often vagotonic among the football players.
On the other hand, it is reasonable to suppose that football players able to rapidly adjust their HR to exercise intensity changes would be better fitted to be positioned as wingers. This capability may represent a hemodynamic advantage for intermittent match situations where fast HR transitions (and consequently quicker increments in oxygen delivery to the active muscles) are required. It also enhances the potential utility of the 4sET test as a tool for identifying or selecting potentially better wingers.
Nevertheless, other relevant questions remain to be answered. Would CVI values change along the season? If so, would the CVI reflect specific training-induced physiological adaptations?
CONCLUSIONS
From our data it is possible to extract five conclusions: (a) CVI in elite football players did not substantially differ from age-matched healthy non-athletes; (b) among elite football players, the wingers are those with the higher CVIs and therefore more often vagotonic; (c) differences in the magnitude of exercise-induced cardiac vagal withdrawal reflex among elite football players are not strongly related or good predictors of other classical indicators of sports performance or training, such as maximal HR and VO2 max; (d) resting supine HR in elite football players, at least when obtained at pre-season evaluation, are only partially mediated by CVI; (e) CVI values tend to be quite stable in one-year apart evaluations of elite football players; (f) in agreement with previously published studies, some (but not all) specific groups of athletes exhibit higher CVIs, as compared to non-athletes.
ACKNOWLEDGMENTS
This study was partially funded by research grants from CNPq (Conselho Nacional de Pesquisa e Desenvolvimento Científico) and FAPERJ (Fundação de Amparo a Pesquisa do Estado do Rio de Janeiro) agencies.
REFERENCES
-
1Kunz M. 265 million playing football. FIFA Magazine. 2007:10-5.
-
2Barnes C, Archer DT, Hogg B, Bush M, Bradley PS. The evolution of physical and technical performance parameters in the English Premier League. Int J Sports Med. 2014;35(13):1095-1100. DOI:10.1055/s-0034-1375695.
» https://doi.org/10.1055/s-0034-1375695 -
3Dvorak J, Grimm K, Schmied C, Junge A. Feasibility of precompetition medical assessment at FIFA World Cups for female youth players. Brit J Sports Med. 2012;46(16):1132-3. DOI:10.1136/bjsports-2011-090374
» https://doi.org/10.1136/bjsports-2011-090374 -
4Reilly T, Bangsbo J, Franks A. Anthropometric and physiological predispositions for elite soccer. J Sport Sci. 2000;18(9):669-83. DOI:10.1080/02640410050120050
» https://doi.org/10.1080/02640410050120050 -
5Dvorak J, Kramer EB, Schmied CM, Drezner JA, Zideman D, Patricios J, et al. The FIFA medical emergency bag and FIFA 11 steps to prevent sudden cardiac death: setting a global standard and promoting consistent football field emergency care. Brit J Sports Med. 2013;47(18):1199-202. DOI:10.1136/bjsports-2013-092767.
» https://doi.org/10.1136/bjsports-2013-092767 -
6Bessem B, de Bruijn MC, Nieuwland W. The ECG of high-level junior soccer players: comparing the ESC vs the Seattle criteria. Brit J Sports Med. 2015;49(15):1000-6. DPO:10.1136/bjsports-2013-093245
-
7Signorelli GR, Perim RR, Santos TM, Araujo CG. A pre-season comparison of aerobic fitness and flexibility of younger and older professional soccer players. Int J Sports Med. 2012;33(11):867-72. DOI:10.1055/s-0032-1311597.
» https://doi.org/10.1055/s-0032-1311597 -
8Clemente FM, Couceiro MS, Martins FM, Ivanova MO, Mendes R. Activity profiles of soccer players during the 2010 world cup. J Hum Kinet. 2013;38:201-11. DOI:10.2478/hukin-2013-0060.
» https://doi.org/10.2478/hukin-2013-0060 -
9Hoppe MW, Slomka M, Baumgart C, Weber H, Freiwald J. Match running performance and success across a season in German Bundesliga soccer teams. Int J Sports Med. 2015;36(7):563-6. DOI:10.1055/s-0034-1398578.
» https://doi.org/10.1055/s-0034-1398578 -
10Araujo CG, Scharhag J. Athlete: a working definition for medical and health sciences research. Scand J Med Sci Sports. 2016;26(1):4-7. DOI:10.1111/sms.12632
» https://doi.org/10.1111/sms.12632 -
11Dixon EM, Kamath MV, McCartney N, Fallen EL. Neural regulation of heart rate variability in endurance athletes and sedentary controls. Cardiovasc Res. 1992;26(7):713-9.
-
12Araujo CG, Nóbrega AC, Castro CL. Vagal activity: effect of age, sex and physical activity pattern. Braz J Med Biol Res. 1989;22(7):909-11.
-
13Boyett MR, D'Souza A, Zhang H, Morris GM, Dobrzynski H, Monfredi O. Viewpoint: is the resting bradycardia in athletes the result of remodeling of the sinoatrial node rather than high vagal tone? J Appl Physiol (1985). 2013;114(9):1351-5. DOI:10.1152/japplphysiol.01126.2012
» https://doi.org/10.1152/japplphysiol.01126.2012 -
14Coote JH, White MJ. CrossTalk proposal: bradycardia in the trained athlete is attributable to high vagal tone. J Physiol. 2015;593(8):1745-7. DOI:10.1113/jphysiol.2014.284364
» https://doi.org/10.1113/jphysiol.2014.284364 -
15Aubert AE, Seps B, Beckers F. Heart rate variability in athletes. Sports Med. 2003;33(12):889-919.
-
16Hettinga FJ, Monden PG, van Meeteren NL, Daanen HA. Cardiac acceleration at the onset of exercise: a potential parameter for monitoring progress during physical training in sports and rehabilitation. Sports Med. 2014;44(5):591-602. DOI:10.1007/s40279-013-0141-y
» https://doi.org/10.1007/s40279-013-0141-y -
17Abad CC, do Nascimento AM, Gil S, Kobal R, Loturco I, Nakamura FY, et al. Cardiac autonomic control in high level Brazilian power and endurance track-and-field athletes. Int J Sports Med. 2014;35(9):772-8. DOI:10.1055/s-0033-1363268.
» https://doi.org/10.1055/s-0033-1363268 -
18Carter JB, Banister EW, Blaber AP. Effect of endurance exercise on autonomic control of heart rate. Sports Med. 2003;33(1):33-46.
-
19Proietti R, di Fronso S, Pereira LA, Bortoli L, Robazza C, Nakamura FY, et al. Heart rate variability discriminates competitive levels in professional soccer players. J Strength Cond Res. 2017;31(6):1719-25. DOI:10.1519/JSC.0000000000001795
» https://doi.org/10.1519/JSC.0000000000001795 -
20Michailidis Y. Stress hormonal analysis in elite soccer players during a season. J Sport Health Sci. 2014;3:279-83. DOI:10.1016/j.jshs.2014.03.016
» https://doi.org/10.1016/j.jshs.2014.03.016 -
21Wilson J. The question: why is full-back the most important position on the pitch? The Guardian. 2009; 2009/03/25.
-
22Araujo CG, Castro CL, Franca JF, Ramos PS. 4-Second exercise test: reference values for ages 18-81 years. Arq Bras Cardiol. 2015;104(5):366-74. DOI:10.5935/abc.20150026
» https://doi.org/10.5935/abc.20150026 -
23Araujo CG, Nobrega AC, Castro CL. Heart rate responses to deep breathing and 4-seconds of exercise before and after pharmacological blockade with atropine and propranolol. Clinical Auton Res. 1992;2(1):35-40.
-
24Nobrega AC, Castro CL, Araujo CG. Relative roles of the sympathetic and parasympathetic systems in the 4-s exercise test. Braz J Med Biol Res. 1990;23(12):1259-62.
-
25Araujo CG, Ricardo DR, Almeida MB. Intra and interdays reliability of the 4-second exercise test. Rev Bras Med Esporte. 2003;9(5):293-8. DOI:10.1590/S1517-86922003000500005
» https://doi.org/10.1590/S1517-86922003000500005 -
26Knopfli BH, Bar-Or O. Vagal activity and airway response to ipratropium bromide before and after exercise in ambient and cold conditions in healthy cross-country runners. Clin J Sports Med. 1999;9(3):170-6.
-
27Teixeira FP, Ricardo DR, Castro CLB, Araújo CGS. Evaluating cardiac vagal activity on a conventional electrocardiogram. Arq Bras Cardiol. 2007;88(4):373-8. DOI:10.1590/S0066-782X2007000400002
» https://doi.org/10.1590/S0066-782X2007000400002 -
28Millar PJ, MacDonald MJ, Bray SR, McCartney N. Isometric handgrip exercise improves acute neurocardiac regulation. Eur J Appl Physiol. 2009;107(5):509-15. DOI:10.1007/s00421-009-1142-2
» https://doi.org/10.1007/s00421-009-1142-2 -
29Stang J, Couto M, Stensrud T, Mowinckel P, Moreira A, Carlsen KH. Assessment of parasympathetic activity in athletes: comparing two different methods. Med Sci Sports Exerc. 2016;48(2):316-22. DOI:10.1249/MSS.0000000000000769
» https://doi.org/10.1249/MSS.0000000000000769 -
30Duarte CV, Araujo CG. Cardiac vagal index does not explain age-independent maximal heart rate. Int J Sports Med. 2013;34(6):502-6. DOI:10.1055/s-0032-1323818.
» https://doi.org/10.1055/s-0032-1323818 -
31Ricardo DR, Almeida MB, Franklin BA, Araújo CGS. Initial and final exercise heart rate transients: influence of gender, aerobic fitness, and clinical status. Chest. 2005;127(1):318-27. DOI:10.1378/chest.127.1.318
» https://doi.org/10.1378/chest.127.1.318 -
32Flatt AA, Esco MR. Heart rate variability stabilization in athletes: towards more convenient data acquisition. Clin Physiol Funct Imag. 2016; 36(5):331-6. DOI:10.1111/cpf.12233.
» https://doi.org/10.1111/cpf.12233 -
33Ueno LM, Moritani T. Effects of long-term exercise training on cardiac autonomic nervous activities and baroreflex sensitivity. Eur J Appl Physiol. 2003;89(2):109-14. DOI:10.1007/s00421-002-0777-z
» https://doi.org/10.1007/s00421-002-0777-z -
34Martinelli FS, Chacon-Mikahil MP, Martins LE, Lima-Filho EC, Golfetti R, Paschoal MA, et al. Heart rate variability in athletes and nonathletes at rest and during head-up tilt. Braz J Med Biol Res. 2005;38(4):639-47. DOI:10.1590/S0100-879X2005000400019
» https://doi.org/10.1590/S0100-879X2005000400019 -
35Bonaiuto M, Di Mauro D, Speciale F, Pagano F, Buda D, Vita G, et al. Evaluation of heart rate recovery in relation to playing position in professional soccer players. J Sports Med Phys Fitness. 2012;52(6):583-8.
-
36Oliveira RS, Leicht AS, Bishop D, Barbero-Alvarez JC, Nakamura FY. Seasonal changes in physical performance and heart rate variability in high level futsal players. Int J Sports Med. 2013;34(5):424-30. DOI:10.1055/s-0032-1323720
» https://doi.org/10.1055/s-0032-1323720 -
37Duarte CV, Araujo CG. Treinamento para disfunção vagal cardíaca com repetições da transição repouso-exercício. Rev Bras Ativ Fis & Saúde. 2013;18(6):688-97. DOI:10.12820/rbafs.v.18n6p688
» https://doi.org/10.12820/rbafs.v.18n6p688 -
38Furtado EC, Araujo CG. Cardiac arrhythmias triggered by sudden and dynamic efforts. Ann Noninvasive Electrocardiol 2010;15(2):151-6. DOI:10.1111/j.1542-474X.2010.00356.x
» https://doi.org/10.1111/j.1542-474X.2010.00356.x -
39Nobrega AC, Araujo CG. Heart rate transient at the onset of active and passive dynamic exercise. Med Sci Sports Exerc. 1993;25(1):37-41.
-
40Vianna LC, Oliveira RB, Silva BM, Ricardo DR, Araujo CG. Water intake accelerates post-exercise cardiac vagal reactivation in humans. Eur J Appl Physiol. 2008;102(3):283-8. DOI:10.1007/s00421-007-0584-7
» https://doi.org/10.1007/s00421-007-0584-7 -
41Ricardo DR, Silva BM, Vianna LC, Araujo CG. Cardiac vagal withdrawal and reactivation during repeated rest-exercise transitions. Eur J Appl Physiol. 2010;110:933-42. DOI:10.1007/s00421-010-1555-y
» https://doi.org/10.1007/s00421-010-1555-y -
42Mattioli GM, Araujo CG. Association between initial and final transient heart rate responses in exercise testing. Arq Bras Cardiol. 2009;93(2):141-6. DOI:10.1590/S0066-782X2009000800012
» https://doi.org/10.1590/S0066-782X2009000800012 -
43Lazzoli JK, Soares PP, da Nobrega AC, de Araujo CG. Electrocardiographic criteria for vagotonia-validation with pharmacological parasympathetic blockade in healthy subjects. Int J Cardiol. 2003;87(2-3):231-6. DOI:10.1016/S0167-5273(02)00330-3
» https://doi.org/10.1016/S0167-5273(02)00330-3 -
44Teixeira FP, Ricardo DR, de Castro CL, de Araujo CG. Evaluating cardiac vagal activity on a conventional electrocardiogram. Arq Bras Cardiol. 2007;88(4):378-83. DOI:10.1590/S0066-782X2007000400002.
» https://doi.org/10.1590/S0066-782X2007000400002 -
45Lazzoli JK, Castro CLB, Nóbrega ACL, Araújo CGS. Accuracy of vagotonia criteria in the 12-lead resting electrocardiogram: analysis with ROC curves. Rev Bras Med Esporte. 2002;8(2):50-8. DOI:10.1590/S1517-86922002000200004.
» https://doi.org/10.1590/S1517-86922002000200004 -
46Silva BM, Vianna LC, Oliveira RB, Ricardo DR, Araujo CG. Similar cardiac vagal withdrawal at the onset of arm and leg dynamic exercise. Eur J Appl Physiol. 2008;102(6):695-701. DOI:10.1007/s00421-007-0640-3
» https://doi.org/10.1007/s00421-007-0640-3 -
47Almeida MB, Ricardo DR, Araujo CG. Validation of the 4-second exercise test in the orthostatic position. Arq Bras Cardiol. 2004;83(2):155-9. DOI:10.1590/S0066-782X2004001400007.
» https://doi.org/10.1590/S0066-782X2004001400007 -
48Robinson BF, Epstein SE, Beiser GD, Braunwald E. Control of heart rate by the autonomic nervous system. Studies in man on the interrelation between baroreceptor mechanisms and exercise. Circ Res. 1966;19(2):400-11.
-
49Clarke BF, Ewing DJ. Cardiovascular reflex tests; in the natural history of diabetic autonomic neuropathy. N Y State J Med. 1982;82(6):903-8.
-
50Park G, Vasey MW, Van Bavel JJ, Thayer JF. Cardiac vagal tone is correlated with selective attention to neutral distractors under load. Psychophysiology. 2013;50(4):398-406. DOI:10.1111/psyp.12029.
» https://doi.org/10.1111/psyp.12029
Publication Dates
-
Publication in this collection
22 Oct 2018 -
Date of issue
2018
History
-
Received
09 Apr 2018 -
Reviewed
10 May 2018 -
Accepted
20 May 2018 -
Published
31 May 2018