Abstracts
OBJECTIVE: Patients with peripheral artery disease (PAD) or coronary artery disease (CAD) must have their risk factors rigorously controlled, but there is a gap between practice and ideal. This study aimed to demonstrate how cardiovascular prevention is performed for these patients in a Brazilian university hospital, and to identify predictors of good practice. METHODS: 192 patients with CAD or PAD were included in this transversal study. Six prevention goals were analyzed: 1) systolic blood pressure < 140 mmHg; 2) diastolic blood pressure < 90 mmHg; 3) LDL < 100 mg/dL; 4) HDL > 40 mg/dL for men/ > 50 mg/dL for women; 5) not smoking; 6) regular practice of aerobic exercise. RESULTS: The mean age of the patients was 65.7 years, and 60% were men. The percentage of patients that achieved goals 1 to 6 was 57.3%, 67.2%, 40.1%, 27.6%, 88.5%, and 25%, respectively. The average number of goals achieved by patients was 3.06 ± 1.31. When asked about the reason for being treated, 182(94.8%) patients claimed to know about their disease, but when the diagnosis reported by the patients with the physician's diagnosis were compared, it was discordant in 12% of cases. The average number of goals achieved by patients was 2.67 and 3.46 for the PAD and the CAD group, respectively. The independent predictors of a higher number of goals/patient were: male gender (p = 0.011), hospitalization (p < 0.0001), CAD diagnosis (p = 0.011), knowing the reason for treatment (p = 0.028), and receiving prescription of β -blocker (p = 0.011). CONCLUSION: Even in an university hospital, prevention is far from ideal. Efforts to increase patients' awareness should be stimulated, and can possibly improve the effectiveness of preventive measures.
Atherosclerosis; risk factors; peripheral arterial disease; coronary disease; prevention
OBJETIVO: Pacientes com doença arterial periférica (DAP) ou doença arterial coronariana (DAC) necessitam de um controle rigoroso dos seus fatores de risco, mas essa prática ainda está muito aquém da ideal. O objetivo deste estudo foi verificar como é feita a prevenção cardiovascular nesses pacientes em um hospital universitário no Brasil e identificar os preditores de melhor prevenção secundária. MÉTODOS: Trata-se de estudo transversal, com 192 pacientes portadores de DAC ou DAP. Foram analisadas seis metas a serem atingidas: 1) pressão arterial sistólica < 140 mmHg; 2) pressão arterial diastólica < 90 mmHg; 3) LDL < 100 mg/dL; 4) HDL > 40 mg/dL para homens/> 50 mg/dL para mulheres; 5) não fumar; 6) prática de exercício físico aeróbico regular. RESULTADOS: A idade média dos pacientes é 65,7 anos e 60% são do sexo masculino. A porcentagem dos pacientes que atingiram de 1 a 6 metas foi 57,3%; 67,2%; 40,1%; 27,6%; 88,5% e 25%, respectivamente. O número médio de metas atingidas por paciente foi 2,67 e 3,46 para os pacientes com DAP e DAC, respectivamente. Os preditores independentes de maior número de metas/paciente foram: sexo masculino (p = 0,011), estar internado (p < 0,001), diagnóstico de DAC (p = 0,011), saber o motivo do tratamento (p = 0,028) e receber prescrição de β-bloqueador (p = 0,011). CONCLUSÃO: Mesmo em um hospital universitário, a prevenção encontra-se longe da ideal. Esforços para aumentar a conscientização do paciente devem ser estimulados e podem possivelmente melhorar a efetividade das medidas preventivas.
Aterosclerose; fatores de risco; doença arterial periférica; doenças da coronária; prevenção
ARTIGO ORIGINAL
Improving cardiovascular prevention through patient awareness
Melhora da prevenção cardiovascular pelo conhecimento do paciente
Veronica Y. P. Chang; Karen K. Handa; Marcos Fernandes; Carolina Yacoub; Adriana Pastana; Bruno Caramelli; Daniela Calderaro
Interdisciplinary Medicine in Cardiology Unit, Instituto do Coração (InCor), São Paulo, SP, Brazil
Correspondence to Correspondence to: Veronica Y.P. Chang Unidade de Medicina Interdisciplinar em Cardiologia Instituto do Coração Av. Dr. Eneas Carvalho de Aguiar, 44 São Paulo, SP, Brazil CEP: 05403-000 vero_yulin@hotmail.com
SUMMARY
OBJECTIVE: Patients with peripheral artery disease (PAD) or coronary artery disease (CAD) must have their risk factors rigorously controlled, but there is a gap between practice and ideal. This study aimed to demonstrate how cardiovascular prevention is performed for these patients in a Brazilian university hospital, and to identify predictors of good practice.
METHODS: 192 patients with CAD or PAD were included in this transversal study. Six prevention goals were analyzed: 1) systolic blood pressure < 140 mmHg; 2) diastolic blood pressure < 90 mmHg; 3) LDL < 100 mg/dL; 4) HDL > 40 mg/dL for men/ > 50 mg/dL for women; 5) not smoking; 6) regular practice of aerobic exercise.
RESULTS: The mean age of the patients was 65.7 years, and 60% were men. The percentage of patients that achieved goals 1 to 6 was 57.3%, 67.2%, 40.1%, 27.6%, 88.5%, and 25%, respectively. The average number of goals achieved by patients was 3.06 ± 1.31. When asked about the reason for being treated, 182(94.8%) patients claimed to know about their disease, but when the diagnosis reported by the patients with the physician's diagnosis were compared, it was discordant in 12% of cases. The average number of goals achieved by patients was 2.67 and 3.46 for the PAD and the CAD group, respectively. The independent predictors of a higher number of goals/patient were: male gender (p = 0.011), hospitalization (p < 0.0001), CAD diagnosis (p = 0.011), knowing the reason for treatment (p = 0.028), and receiving prescription of β-blocker (p = 0.011).
CONCLUSION: Even in an university hospital, prevention is far from ideal. Efforts to increase patients' awareness should be stimulated, and can possibly improve the effectiveness of preventive measures.
Keywords: Atherosclerosis; risk factors; peripheral arterial disease; coronary disease; prevention.
RESUMO
OBJETIVO: Pacientes com doença arterial periférica (DAP) ou doença arterial coronariana (DAC) necessitam de um controle rigoroso dos seus fatores de risco, mas essa prática ainda está muito aquém da ideal. O objetivo deste estudo foi verificar como é feita a prevenção cardiovascular nesses pacientes em um hospital universitário no Brasil e identificar os preditores de melhor prevenção secundária.
MÉTODOS: Trata-se de estudo transversal, com 192 pacientes portadores de DAC ou DAP. Foram analisadas seis metas a serem atingidas: 1) pressão arterial sistólica < 140 mmHg; 2) pressão arterial diastólica < 90 mmHg; 3) LDL < 100 mg/dL; 4) HDL > 40 mg/dL para homens/> 50 mg/dL para mulheres; 5) não fumar; 6) prática de exercício físico aeróbico regular.
RESULTADOS: A idade média dos pacientes é 65,7 anos e 60% são do sexo masculino. A porcentagem dos pacientes que atingiram de 1 a 6 metas foi 57,3%; 67,2%; 40,1%; 27,6%; 88,5% e 25%, respectivamente. O número médio de metas atingidas por paciente foi 2,67 e 3,46 para os pacientes com DAP e DAC, respectivamente. Os preditores independentes de maior número de metas/paciente foram: sexo masculino (p = 0,011), estar internado (p < 0,001), diagnóstico de DAC (p = 0,011), saber o motivo do tratamento (p = 0,028) e receber prescrição de β-bloqueador (p = 0,011).
CONCLUSÃO: Mesmo em um hospital universitário, a prevenção encontra-se longe da ideal. Esforços para aumentar a conscientização do paciente devem ser estimulados e podem possivelmente melhorar a efetividade das medidas preventivas.
Unitermos: Aterosclerose; fatores de risco; doença arterial periférica; doenças da coronária; prevenção.
INTRODUCTION
Patients with peripheral artery disease (PAD) or significant coronary artery disease (CAD) are considered at high-risk for cardiac and cerebrovascular events1. The common underlying atherosclerotic process and the concomitance of advanced stages in diverse arterial systems justify why patients with PAD are in the same risk category of patients with known CAD. Actually, it has been suggested that the long-term prognosis of PAD patients can be even worse than that of CAD patients'2.
The worldwide prevalence of PAD is high, ranging from 10.5% to 20% in the elderly population3-5. Considering that even asymptomatic patients with confirmed PAD have a substantial increase in their cardiovascular risk, PAD is a major public health problem. The high importance of this disease has influenced many different medical societies to develop guidelines for appropriate risk factor control1,6,7. However, those recommendations are frequently not translated into clinical practice, as already demonstrated in this context 8-13, and in other clinical situations14,15.
Several studies display multifactorial reasons for this gap, varying from bad medical practice to poor patient treatment adherence8-11,16,17. Moreover, it has been speculated that the patient's awareness of their condition may influence the effectiveness of secondary prevention18.
There is a lack of information regarding the implementation of cardiovascular prevention guidelines for specific populations in Brazil. Hence, the objectives of this study were to analyze the quality of secondary prevention in PAD and in CAD patients, and to identify the predictors of better quality, at the Clinics Hospital of the Medical School of the Universidade de São Paulo in São Paulo - Brazil.
METHODS
This is an observational and transversal study that was conducted at the Medical School of the Universidade de São Paulo, in the vascular surgery service, and in the heart institute of the Clinics Hospital. The protocol had been previously approved by the local ethics committee.
The selection criteria were the presence of stable CAD for the cardiology patients, whereas at the vascular surgery, it was stable aortic disease (aneurysm/ dissection), carotid obstruction, or peripheral obstructive arterial disease. Patients were randomly selected at the outpatient clinic and at the hospital wards and were invited by medical students to participate in the study. After signing an informed consent, patients were interviewed and had their medical charts analyzed.
The questionnaire was designed to identify the self-reported rate of the traditional risk factors for atherosclerosis (hypertension, dyslipidemia, diabetes, smoking, physical inactivity) and whether patients had received medical counseling regarding lifestyle modification.
Patients were also asked to report their medical diagnosis ("Do you know the main reason why you are treated for in this clinic?") and whether they knew the importance of cardiovascular prevention (e.g.:, vascular patients were asked "Do you know that if you exercise, quit smoking, control your blood pressure and cholesterol levels, besides the benefits for your vascular problem, you can also prevent stroke and myocardial infarction?").
The diagnosis registered in the medical chart was compared to the patient's self reported diagnosis. The last available data in the past two years for blood pressure levels, lipid profile, fasting glucose, glycated hemoglobin (HbA1c), and prescription of anti-platelet agents, β-blockers, statins, and angiotensin conversion enzyme-inhibitors (ACE-i) were recorded.
Six desirable prevention goals were defined for every patient: (1) systolic blood pressure < 140 mmHg, (2) diastolic blood pressure < 90 mmHg, (3) LDL-cholesterol < 100 mg/dL, (4) HDL-cholesterol > 40 mg/dL for men and > 50 mg/dL for women, (5) not smoking, and (6) practice of aerobic exercise1,7. For diabetic patients, the HbA1c goal was < 7%. Considering that lipid profile and blood pressure should ideally be checked at least every six months, patients who had not been tested in the past two years were considered as not achieving the blood pressure and/or lipid goals. The number of goals achieved per patient was calculated and statistical analysis was performed to identify the predictors of a greater average number of goals.
STATISTICAL ANALYSIS
A linear regression model was applied to identify the predictors of a greater number of goals achieved by patient. Variables with a previously assumed association to the independent factor (e.g. gender18,19) or those with a statistical significance level that reached a pre-defined p < 0.10 in the univariate test were included in the multivariate analysis.
Statistical significance was considered as a two-tailed probability of less than 0.05. All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) 17.0 software.
RESULTS
Between March and November of 2010, 200 patients were analyzed, and eight were excluded for not having atherosclerosis as the primary cause for cardiovascular disease. From the remaining 192, 93 were selected from the vascular surgery clinic (PAD), and 99 from the cardiology clinic (CAD). Their mean age was 65.66 ± 10.50 years, 77 patients (40%) were women; 77.6% had hypertension, 75% of them were sedentary, 65.7% were current or former smokers, 57.3% had dyslipidemia, and 39.1% had diabetes. Nearly half of them were hospitalized (49%) for elective myocardial revascularization or elective vascular surgical procedures. For PAD patients, the main clinical manifestation of atherosclerotic disease was aortic disease (aneurysm or dissection) in 50%, followed by peripheral artery disease in 22.6%, and carotid obstruction in 20.4% of the cases. The remaining 7% were treated by vascular surgeons because of other atherosclerotic problems, such as popliteal aneurysm or renovascular disease. Almost 60% of the patients were treated by two or more physicians.
Although 70.8% of the patients have reported that they had received dietary counseling, only 44.8% reported following a balanced diet. As for aerobic exercise, 57.8% were encouraged to exercise but only 25% reported practicing it on a regular basis. Regarding medical advice for smoking cessation, 65% of the current and former smokers informed they were encouraged to quit smoking by their physicians.
Statin was the most prescribed class of medication (91.1% of the patients were receiving statins), followed by aspirin (87.5%), beta-blockers (67.2%), angiotensin conversion enzyme inhibitor (54.7%), and clopidogrel (5.2%). 16 patients (8.3%) reported that they did not take medications regularly.
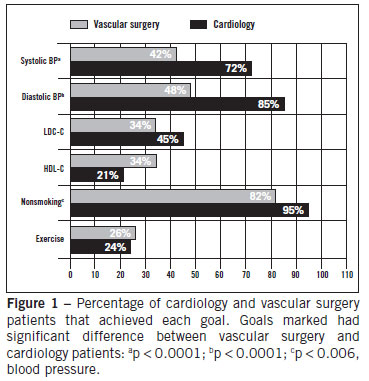
The six prevention goals previously defined for this study (1) systolic blood pressure < 140 mmHg, (2) diastolic blood pressure < 90 mmHg, (3) LDL-cholesterol < 100 mg/dL, (4) HDL-cholesterol > 40 mg/dL for men and > 50 mg/dL for women, (5) not smoking, and (6) practice of aerobic exercise, were achieved in 57.3%, 67.2%, 40.1%, 27.6%, 88.5%, and 25%, respectively. The average number of goals achieved by patient was 3.06 ± 1.31. Only 17.3% of the diabetic patients had HbA1c < 7%.
When asked about the reason for being treated, 182 (94.8%) patients claimed to know their disease, but when the diagnosis reported by the patients were compared with the diagnosis recorded by the physicians in medical charts, it was discordant for 24 patients (12%). Almost 23% of the patients were not aware of the importance of cardiovascular prevention.
The comparison of the demographic characteristics between vascular and cardiology patients is represented on Table 1. There were more diabetic patients in the cardiology group, and cardiology patients received dietary counseling and protective medications more frequently than vascular patients. In the vascular group, there were more current smokers, and patients were more frequently treated by another physician. The rate of discordance between the patients self-reported diagnosis and thaton medical charts was greater in the vascular surgery group.
Twenty- two (23.6%) patients in the PAD group and 14 (14.1%) cardiology (CAD) patients did not have laboratorial exams for the past two years; 46 (49.5%) vascular patients did not have blood pressure measurement, in contrast with the cardiology group, in which only one patient (1%) did not have blood pressure measurement. However, when comparing diabetes monitoring, namely HbA1c, there was an inversion: 16% of the diabetics from vascular surgery did not have HbA1c measurement, while 30% of the diabetics in the cardiology group did not have this test for the past two years. The average values of blood pressure and lipid profile are displayed on Table 1.
As represented on Figure 1, except for the HDL-cholesterol goal, all other goals were more frequently achieved by cardiology patients. There was a significant difference between the two groups regarding the average number of goals achieved per patient (vascular = 2.67 and cardiology = 3.40; p < 0.001).
A series of univariate analysis were performed to determine the predictors that might have contributed to a major number of goals achieved per patient. The following variables were tested: male gender (p = 0.105), age > 50 years (p = 0.149), diabetes (p = 0.188), dyslipidemia (p = 0.392), hypertension (p = 0.321), hospitalization (p < 0.0001), patient from cardiology (p < 0.0001), being treated by another physician (p = 0.687), awareness about the importance of secondary prevention (p = 0.264), knowledge of reason for treatment (p = 0.001), reporting the right diagnosis (p = 0.005), adherence to medical prescription (p = 0.430), physician's advice to undergo aerobic exercise (p = 0.080), physician's dietary counseling (p = 0.528), prescription of acetylsalicylic acid (p = 0.016), prescription of statin (p < 0.0001), prescription of β-blocker (p < 0.0001), and prescription of ACE inhibitors (p = 0.320). Knowing the reason for treatment, reporting the right diagnosis, being hospitalized, being from cardiology clinic, and receiving the prescription of statin, β-blocker or acetylsalicylic acid (ASA) were the factors associated with a greater number of goals per patient.
The variables "knowledge of reason for treatment" and "reporting the right diagnosis" were both significantly associated to the independent variable, but considering their collinearity, only the first one was included in the linear regression model. According to the multivariate analysis, the independent predictors that contributed to a higher number of goals per patient were: male gender, hospitalization, being from cardiology clinic, knowing the reason for treatment, and receiving prescription of β-blocker.
DISCUSSION
In this study, the prevalence of traditional risk factors was similar to that previously found in other populations; for example, the 77.6% hypertension rate observed is compatible with the range from 46% to 82.5% reported in five other studies that included patients with atherosclerosis10,11,16,17,20. In the REACH Registry, where a total of 55.499 patients with symptomatic CAD, PAD or cerebrovascular disease from 44 different countries were analyzed, the authors found a prevalence of hypertension, hypercholesterolemia, diabetes, and smoking of 80%, 70.2%, 37.5%, and 14.4%, respectively8. These findings indicate the great potential of prevention practices in high-risk populations.
Although it is well recognized that lifestyle modification is one of the most important interventions for cardiovascular risk reduction, it is often neglected and less translated into clinical practice than medication prescription9,10,20. In the present study, only 44.8% of the patients reported following a balanced diet, and only 25% exercised on a regular basis. The poor adherence of patients to prescription usually is the first factor considered to justify gaps between theory and practice, but in the present study, physicians' adherence to guidelines recommendations comes first, as only 70.8% of the patients reported receiving dietary advice and only 57.85% were encouraged by their physicians to exercise. Regarding medical advice for smoking cessation, 65% of the current and former smokers reported they were encouraged to quit smoking by their physicians; the 11.6% rate of current smokers in this study's population, although not ideal, can be considered below the smoking prevalence in other populations with atherosclerotic disease (22%20 to 44% in patients with PAD)17.
The prescription of medications that improve secondary prevention showed better results. According to the reference guidelines for management of CAD and PAD patients1,6,7, antiplatelet therapy is the only medication that should be prescribed for every patient included in the study (unless contra-indicated): the 87.5% ASA combined with the 5.2% clopidogrel prescription rates were satisfactory. Statins were prescribed to 91.1% of the patients, 67.2% of them were under β -blocker therapy, and 54.7% were on ACE inhibitors (ACEi). Considering that systolic blood pressure levels were not well controlled in almost 43% of the patients, the ACEi and β -blockers certainly were underused, and probably there was also a inadequacy in dose titration. The same concern is applicable to lipid control; despite that 91.1% of the patients received statin therapy, only 40.1% had LDL-cholesterol level below 100 mg/dL. The 8.3% rate of poor adherence to medication prescription can also contribute to the lack of efficacy in achieving the desired blood pressure and lipid levels.
Even though this reality is far from ideal, it is equal to or even better than reports in the literature. In the largest systematic review regarding secondary prevention measures for patients with PAD, published by Flu et al. in 2010, from the 671 analyzed patients with PAD, only 23% were prescribed walking exercise and only 39% of the 1.963 patients who were current smokers received smoking cessation advice9. Only 63% received antiplatelet agents, 45% received lipid-lowering medications, and 46% were under anti-hypertensive medication therapy. In the study published by Lloyd et al.11, among 313 patients with abdominal aortic aneurysm (80% of them had concomitant peripheral arterial obstructive disease) only 60% received antiplatelet medication, 41% statin, 39% ACEi, and 38% β-blockers11.
The average number of 3.06 out of six target goals achieved per patient represents an overview of the unsatisfactory practice of secondary prevention in this population. Still, it is consistent with previous studies. This instrument of evaluation had been previously applied by Kinikini et al.10 to analyze the adequacy of nine prevention goals to the American College of Cardiology/American Heart Association (ACC/AHA) secondary prevention guidelines recommendations in patients with peripheral arterial disease. In this study, 54% met the goal for blood pressure, 35% reported exercising, and 36% met the LDL cholesterol goal. These results are very similar to the present study's: 57% and 67% achieved the goal for systolic and diastolic blood pressure, 25% exercised, and 40.1% presented LDL cholesterol < 100 mg/dL. Among patients with diabetes, 17.3% had HbA1c < 7% in the present study and 24% in Kinikini's10. Notwithstanding, in that study there were almost seven times more current smokers than in the present study. The mean number of goals achieved per patient was 4.8 ± 1.5, and their 53% rate of goal compliance is similar to the 51% rate of this population, also very low.
In the present study, male gender was related to a greater number of goals achieved per patient. Gender has already been pointed in literature as an important prognostic factor in the specific field of secondary prevention for cardiovascular events. Previous data have also suggested that the suboptimal management of risk factors occurs mainly in women19,21,22.
The prescription of β-blockers was another independent factor related to the number of goals achieved per patient. There is possibly a direct influence of the medication in two of the six pre-defined goals (systolic and diastolic blood pressure control), but a β-blocker prescription could possibly be a marker of better medical practice.
Although secondary prevention was unsatisfactory both for PAD and CAD patients, it was significantly better in the latter group. After controlling for potential confounding variables, such as differences between groups in patient's knowledge about their disease and different rates of medication prescription, CAD group remained an independent predictor of a greater number of goals achievement per patient. There are other studies that showed that CAD patients have better risk factor control than patients with other forms of atherothrombotic disease manifestation16,17,20,23. This difference is certainly related to many reasons, which come from physicians' attitudes, such as the surgeon's focus to procedures concerns, up to patients' responsibility for their care, but the putative role of each of these factors remains speculative.
In the cardiology clinic, the link between risk factor control and coronary artery disease management is more incorporated into practice; one possible reason is that, besides the long-term prognostic impact of the preventive measures, there is also a short-term benefit in the control of ischemia-related symptoms, such as dyspnea and angina. Vascular surgeons frequently spend too much time on very specific procedures' concerns rather than secondary prevention. It has already been shown, in a study with general practitioners, that physicians underestimate the cardiovascular risk of PAD patients17, but the present study does not provide enough information to conclude whether there is a difference between cardiologists and vascular surgeons regarding knowledge about secondary prevention.
Better cardiovascular prevention delivered for hospitalized patients can reflect not only on the immediate correction of eventual poor patient adherence to medications dosage and schedule, but also on an improvement in the medical care, motivated by the illness severity and facilitated by the longer time that physicians can spend with their patients.
Knowing the reason for treatment was identified as a predictor of better secondary prevention. Undoubtedly, the patients' responsibility and adherence to physician recommendations depend on the degree of perception they have regarding their disease. Moreover, when patients have access to information, they can discuss with their physicians and improve the resultant prescription of preventive practices. McDermott el al. has previously suggested that patients with peripheral arterial disease underestimate their cardiovascular risk when compared to CAD patients20. They compared the awareness of cardiovascular risk and knowledge of the importance of prevention among patients with PAD, patients with CAD, and patients without atherosclerotic disease. The belief regarding risks of adverse cardiovascular events for hypothetical patients with PAD was the lowest, right among those who had PAD, even when they were compared to patients without atherosclerosis. Hirsch et al. have also found in their United States population-based survey a low familiarity with PAD; only 25% of the 2.501 participants showed an awareness of PAD, in contrast to the 67.1% and 73.9% awareness of coronary artery disease and stroke, respectively18. An analysis focused on the subgroup of responders that claimed to know about PAD demonstrated that only 14% recognized an increased risk of death in this group18. Although it has already been suggested that patients' awareness of their condition may influence the effectiveness of secondary prevention, to the authors' knowledge, this is the first time that the association between patient's awareness and better prevention goals has been statistically demonstrated18,20,23.
This was a transversal study and did not provide prospective information regarding the implications of the poor secondary prevention practice. Moreover another limitation of this study is the fact that the only source of information for assessment of variables such as risk factors prevalence, rates of physician advice for lifestyle modification, and patient adherence to treatment, was the patients' answer during the interview. Therefore, it is possible that some of these rates are underestimated. In this study, patients without blood pressure measurement and lipid profile for the past two years were considered as not achieving blood pressure control or lipid goals, based upon the recommendations for its periodical assessment. The authors consider that not checking these parameters can be even worse than obtaining a borderline value.
The gap between real and ideal practice observed in a Brazilian reference university hospital certainly reflects the public health problem faced worldwide. Physicians' attention to prevention goals must be enhanced, but the close relation between patients' knowledge about the importance of preventive measures and the status of risk factors control provides an important insight to plan population based intervention programs and to improve the disturbing reality of secondary cardiovascular prevention.
Submitted on: 10/26/2011
Approved on: 04/11/2012
Conflict of interest: None.
Study conducted at the Interdisciplinary Medicine in Cardiology Unit, InCor, São Paulo, SP, Brazil
- 1. Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, et al. American Association for Vascular Surgery; Society for Vascular Surgery; Society for Cardiovascular Angiography and Interventions; Society for Vascular Medicine and Biology; Society of Interventional Radiology; ACC/AHA Task Force on Practice Guidelines Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease; American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; Transatlantic Inter-Society Consensus; Vascular Disease Foundation. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to develop guidelines for the management of patients with peripheral arterial disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006;113(11):e463-654.
- 2. Welten GM, Schouten O, Hoeks SE, Chonchol M, Vidakovic R, van Domburg RT, et al. Long-term prognosis of patients with peripheral arterial disease: a comparison in patients with coronary artery disease. J Am Coll Cardiol. 2008; 51(16):1588-96.
- 3. Makdisse M, Pereira AC, Brasil DP, Borges JL, Machado-Coelho GL, Krieger JE, et al. Hearts of Brazil Study and Peripheral Arterial Disease Committee of the Brazilian Society of Cardiology/Funcor. Prevalence and risk factors associated with peripheral arterial disease in the Hearts of Brazil Project. Arq Bras Cardiol. 2008;91(6):370-82.
- 4. Criqui MH. Peripheral arterial disease - epidemiological aspects. Vasc Med. 2001;6(3 Suppl):3-7.
- 5. Diehm C, Schuster A, Allenberg JR, Darius H, Haberl R, Lange S, et al. High prevalence of peripheral arterial disease and co-morbidity in 6880 primary care patients: cross-sectional study. Atherosclerosis. 2004;172(1):95-105.
- 6. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, TASC II Working Group, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33(Suppl 1):S1-75.
- 7. Sposito AC, Caramelli B, Fonseca FA, Bertolami MC, Afiune Neto A, Souza AD, Sociedade Brasileira de Cardiologia. IV Brazilian guideline for dyslipidemia and atherosclerosis prevention: Department of Atherosclerosis of Brazilian Society of Cardiology. Arq Bras Cardiol. 2007;88(Suppl 1):2-19.
- 8. Bhatt DL, Steg PG, Ohman EM, Hirsch AT, Ikeda Y, Mas JL, et al. REACH Registry Investigators International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA. 2006; 295(2):180-9.
- 9. Flu HC, Tamsma JT, Lindeman JHN, Hamming JF, Lardenoye JHP. A systematic review of implementation of established recommended secondary prevention measures in patients with PAOD. Eur J Vasc Endovasc Surg. 2010; 39(1):70-86.
- 10. Kinikini D, Sarfati MR, Mueller MT, Kraiss LW, American Heart Association, American College of Cardiology. Meeting AHA/ACC secondary prevention goals in a vascular surgery practice: an opportunity we cannot afford to miss. J Vasc Surg. 2006;43(4):781-7.
- 11. Lloyd GM, Newton JD, Norwood MG, Franks SC, Bown MJ, Sayers RD. Patients with abdominal aortic aneurysm: are we missing the opportunity for cardiovascular risk reduction? J Vasc Surg. 2004;40(4):691-7.
- 12. Hoeks SE, Scholte op Reimer WJ, van Gestel YR, Schouten O, Lenzen MJ, Flu WJ, et al. Medication underuse during long-term follow-up in patients with peripheral arterial disease. Circ Cardiovasc Qual Outcomes. 2009;2(4):338-43.
- 13. Rehring TF, Sandhoff BG, Stolcpart RS, Merenich JA, Hollis HW Jr. Atherosclerotic risk factor control in patients with peripheral arterial disease. J Vasc Surg. 2005;41(5):816-22.
- 14. Deheinzelin D, Braga AL, Martins LC, Martins MA, Hernandez A, Yoshida WB, et al. Trombo Risc Investigators. Incorrect use of thromboprophylaxis for venous thromboembolism in medical and surgical patients: results of a multicentric, observational and cross-sectional study in Brazil. J Thromb Haemost. 2006;4(6):1266-70.
- 15. Fornari LS, Calderaro D, Nassar IB, Lauretti C, Nakamura L, Bagnatori R, et al. Misuse of antithrombotic therapy in atrial fibrillation patients: frequent, pervasive and persistent. J Thromb Thrombolysis. 2007;23(1):65-71.
- 16. Zeymer U, Parhofer KG, Pittrow D, Binz C, Schwertfeger M, Limbourg T, et al. Risk factor profile, management and prognosis of patients with peripheral arterial disease with or without coronary artery disease: results of the prospective German REACH registry cohort. Clin Res Cardiol. 2009;98(4):249-56.
- 17. Blacher J, Cacoub P, Luizy F, Mourad JJ, Levesque H, Benelbaz J, et al. Peripheral arterial disease versus other localizations of vascular disease: the ATTEST study. J Vasc Surg. 2006;44(2):314-8.
- 18. Hirsch AT, Murphy TP, Lovell MB, Twillman G, Treat-Jacobson D, Harwood EM, et al. Peripheral Arterial Disease Coalition. Gaps in public knowledge of peripheral arterial disease the first national pad public awareness survey. Circulation. 2007;116(18):2086-94.
- 19.Pâquet M, Pilon D, Tétrault JP, Carrier N. Protective vascular treatment of patients with peripheral arterial disease: guideline adherence according to year, age and gender. Can J Public Health. 2010;101(1):96-100.
- 20. McDermott MM, Mandapat AL, Moates A, Albay M, Chiou E, Celic L, et al. Knowledge and attitudes regarding cardiovascular disease risk and prevention in patients with coronary or peripheral arterial disease. Arch Intern Med. 2003;163(18):2157-62.
- 21. Driscoll A, Beauchamp A, Lyubomirsky G, Demos L, McNeil J, Tonkin A. Suboptimal management of cardiovascular risk factors in coronary heart disease patients in primary care occurs particularly in females. Intern Med J. 2011;41(10):730-6.
- 22. Jarvie JL, Foody JM. Recognizing and improving health care disparities in the prevention of cardiovascular disease in women. Curr Cardiol Rep. 2010;12(6):488-96.
- 23. Cacoub PP, Zeymer U, Limbourg T, Baumgartner I, Poldermans D, Röther J, Bhatt DL, Steg PG; REACH Registry Investigators. Effects of adherence to guidelines for the control of major cardiovascular risk factors on outcomes in the Reduction of Atherothrombosis for Continued Health (REACH) Registry Europe. Heart. 2011;97(8):660-7.
Correspondence to:
Publication Dates
-
Publication in this collection
17 Oct 2012 -
Date of issue
Oct 2012
History
-
Received
26 Oct 2011 -
Accepted
11 Apr 2012