Abstract
Objective:
To estimate the entrance surface air kerma (Ka,e) and air kerma in the region of radiosensitive organs in radiographs of pediatric paranasal sinuses.
Materials and Methods:
Patient data and irradiation parameters were collected in examinations of the paranasal sinuses in children from 0 to 15 years of age at two children's hospitals in the city of Recife, PE, Brazil. We estimated the Ka,e using the X-ray tube outputs and selected parameters. To estimate the air kerma values in the regions of the eyes and thyroid, we used thermoluminescent dosimeters.
Results:
The Ka,e values ranged from 0.065 to 1.446 mGy in cavum radiographs, from 0.104 to 7.298 mGy in Caldwell views, and from 0.113 to 7.824 mGy in Waters views. Air kerma values in the region of the eyes ranged from 0.001 to 0.968 mGy in cavum radiographs and from 0.011 to 0.422 mGy in Caldwell and Waters views . In the thyroid region, air kerma values ranged from 0.005 to 0.932 mGy in cavum radiographs and from 0.002 to 0.972 mGy in Caldwell and Waters views.
Conclusion:
The radiation levels used at the institutions under study were higher than those recommended in international protocols. We recommend that interventions be initiated in order to reduce patient exposure to radiation and therefore the risks associated with radiological examination of the paranasal sinuses.
Keywords:
Radiometry; Radiography; Paranasal sinuses; Pediatrics; Thermoluminescent dosimetry.
Resumo
Objetivo:
Estimar o kerma no ar na superfície de entrada (Ka,e) e o kerma no ar na região de órgãos radiossensíveis em radiografias pediátricas dos seios paranasais.
Materiais e Métodos:
Foram coletados os dados dos pacientes e parâmetros de irradiação em exames de seios paranasais de crianças com 0 a 15 anos, em dois hospitais infantis na cidade do Recife, PE. O Ka,e foi estimado utilizando os rendimentos dos tubos de raios X e os parâmetros selecionados. Os valores de kerma no ar nas regiões dos olhos e tireoide foram estimados utilizando dosímetros termoluminescentes.
Resultados:
Os valores de Ka,e variaram de 0,065 a 1,446 mGy para radiografias cavum, 0,104 a 7,298 mGy para Caldwell e 0,113 a 7,824 mGy para Waters. Os valores de kerma no ar na região dos olhos variaram de 0,001 a 0,968 mGy para cavum e 0,011 a 0,422 mGy para Caldwell e Waters. Na região tireóidea, os valores de kerma no ar variaram de 0,005 a 0,932 mGy para cavum e 0,002 a 0,972 mGy para Caldwell e Waters.
Conclusão:
Os parâmetros de irradiação utilizados pelas instituições foram mais elevados do que os recomendados em protocolos britânicos. Ações de otimização são recomendadas de modo a contribuir para a redução da radiação nos pacientes e, portanto, os riscos.
Unitermos:
Dosimetria; Radiografia; Seios paranasais; Pediatria; Dosimetria termoluminescente
INTRODUCTION
In radiological examinations of the face, radiosensitive anatomical structures, such as the eyes and thyroid, are exposed to ionizing radiation, representing a risk to the patient, due to the possibility of producing biological effects induced by the interaction of the radiation with the tissue. Special attention should be given to radiological examinations performed in pediatric patients, because, in comparison with those of adults, their cells are more radiosensitive and have a longer life expectancy, which increases the risk of stochastic effects(11 [No authors listed]. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Ann ICRP. 2007;37(2-4):1-332.).
Clinical requests for X-ray examinations of the sinuses are quite common in children(22 Tagaya M, Nakata S, Yasuma F, et al. Relationship between adenoid size and severity of obstructive sleep apnea in preschool children. Int J Pediatr Otorhinolaryngol. 2012;76:1827-30.,33 Feres MF, Hermann JS, Sallum AC, et al. Radiographic adenoid evaluation - suggestion of referral parameters. J Pediatr (Rio J). 2014;90:279-85.), in order to investigate diseases of the upper respiratory tract, such as hypertrophy of the adenoids, inflammatory diseases of the sinus cavities, sinus infections, tumors, and facial fractures(44 T-Ping C, Weckx LLM. ENT care of children and adolescents in the Brazilian public healthy system in three different municipalities. Braz J Otorhinolaryngol. 2008;74:571-8..55 Vogler RC, Ii FJ, Pilgram TK. Age-specific size of the normal adenoid pad on magnetic resonance imaging. Clin Otolaryngol Allied Sci. 2000;25:392-5.). Conventional radiography for the radiological study of the sinuses can be performed as follows(66 Jacomelli M, Souza R, Pedreira Júnior WL. Abordagem diagnóstica da tosse crônica em pacientes não-tabagistas. J Bras Pneumol. 2003;29:413-20.,77 Bontrager KL. Tratado de técnica radiológica e base anatômica. 4ª ed. Rio de Janeiro, RJ: Guanabara Koogan; 1999.): lateral X-rays (cavum radiographs); posteroanterior occipitomental X-rays (Waters view); and posteroanterior occipitofrontal X-rays (Caldwell view).
The objective of this study was to evaluate the entrance surface air kerma (Ka,e) for pediatric patients undergoing radiological examinations of the sinuses at two hospitals in Recife, PE, Brazil. We also estimated the air kerma values in the thyroid region and around the eyes.
MATERIALS AND METHODS
The study was conducted at two public hospitals (hereafter referred to as hospital A and hospital B), both of which specialized in the care of pediatric patients. Hospital A has approximately 112 beds, distributed among various clinical areas. Hospital B is a referral center for maternal and child health, with 714 beds and more than 600,000 annual visits to its various clinics. Both hospitals are philanthropic and provide services via the Brazilian Unified Health Care System. Hospital B has two rooms for performing X-ray examinations, both equipped with Philips Bucky Diagnost X-ray equipment, whereas hospital A has only one X-ray examination room, which is equipped with a Shimadzu R 20 X-ray system. None of the X-ray machines evaluated are equipped with automatic exposure control, and the image acquisition system is based on radiographic films at both institutions.
We created a form designed to collect data related to anthropometric characteristics of the patient (gender, weight and height), the type of examination/projection, and the irradiation parameters employed (kV, mAs, focus-to-skin distance, focus-to-film distance, and exposure time). Data were collected by the authors of the study, and neither institution maintains nested records of such information. We monitored the radiological examinations of patients ≤ 15 years of age. For data analysis, patients were divided into the following age groups: 0-1 year; 1-5 years; 5-10 years; and 10-15 years.
Determination of the K a,e
The Ka,e was determined on the basis of the yield of the X-ray tube and the irradiation parameters (indirect method). For that purpose, we used a Radcal ionization chamber, model 20X6-6, positioned in the center of the radiation field, 100 cm from the focal spot and 30 cm from the surface of the table. We measured the air kerma for different values of tube voltage (kV), using a fixed value for the current-time product (mAs). For each kV value, we made three measurements. The mean value obtained was corrected for the pressure-temperature factor and for the calibration factor of the ionization chamber. The calibrations were performed at the Laboratório de Metrologia das Radiações Ionizantes, Departamento de Energia Nuclear da Universidade Federal de Pernambuco (LMRI/DEN-UFPE, Ionizing Radiation Metrology Laboratory, Department of Nuclear Energy at the Federal University of Pernambuco), which follows the standards set by the National Laboratory for the Metrology of Ionizing Radiation at the Radioprotection and Dosimetry Institute of the Brazilian National Nuclear Energy Commission. The yield of X-ray equipment corresponds to the air kerma value (in mGy) per mAs, at a distance of 1 m from the focal spot. A curve for the yields of the different voltage values was constructed and used for determining the yield under the irradiation conditions employed in each of the examinations evaluated. For each patient, the Ka,e was determined by the following equation(88 Davies M, McCallum H, Whiter G, et al. Patient dose audit in diagnostic radiography using custom designed software. Radiography. 1997;3:17-25.):

where Ri is the yield of the X-ray tube for radiographic technique employed in the examination, interpolated from the yield curve in function of the voltage, of the Ri = a.(kV)b type, a and b being curve fitting parameters; Q is the product of tube current by exposure time (mAs) used in the examination; Dref is a distance of 1 m for which the yield has been adjusted; DFP is the distance between the focal point and the skin of the patient; and BSF is the backscatter factor, which is a function of the size of the field, the filtration of the equipment and the radiographic technique used in the examination. A fixed BSF value of 1.30 was adopted(99 Petoussi-Henss N, Zankl M, Drexler G, et al. Calculation of back-scatter factors for diagnostic radiology using Monte Carlo methods. Phys Med Biol. 1998;43:2237-50.).
Estimation of doses near radiosensitive organs using thermoluminescent dosimeters
Pairs of LiF:Mg,Ti (TLD-100) thermoluminescent dosimeters were encapsulated in thin plastic casings (one pair per casing) and placed on the skin of the patient around the eyes and thyroid. The dosimeter pair taken to each institution was always accompanied by another pair of dosimeters that were not irradiated. The reading from those dosimeters (in a white casing) was subtracted from the reading from the irradiated dosimeters. The mean reading of the two dosimeters contained in each casing was converted into air kerma using the calibration curve obtained with diagnostic quality X-ray beams at the LMRI/DEN-UFPE(1010 Associação Brasileira de Normas Técnicas. ABNT NBR ISO/IEC 17025:2005 - Requisitos gerais para a competência de laboratórios de ensaio e calibração. ABNT; 2005.).
RESULTS
Characteristics of the radiological examinations
Figures 1A and 1B show the age distribution of the patients who underwent radiological examinations with lateral and posteroanterior (occipitofrontal and occipitomental) X-rays, respectively. We evaluated 159 radiographs of the sinuses, of which 103 were lateral X-rays (cavum radiographs) and 56 were posteroanterior X-rays, including occipitofrontal and occipitomental X-rays (Caldwell and Waters views, respectively).
Distribution of patients undergoing radiological examination of the sinuses with lateral X-rays (A) and posteroanterior X-rays (B), by age group.
Approximately 60% of the patients undergoing radiological examination of the sinuses at either hospital were male. At hospital A, 72.8% of the patients in whom lateral X-rays were obtained were male, compared with 62.5% of those in whom posteroanterior (occipitofrontal and occipitomental) X-rays were obtained. At hospital B, males accounted for 50.0% of the patients undergoing radiological examination of the sinuses, in either view. Therefore, the gender distribution was much more balanced among the patients seen at hospital B.
Irradiation parameters
The minimum, mean, and maximum voltage used in lateral and posteroanterior (occipitofrontal and occipitomental) X-ray examinations of the sinuses are shown in Table 1. The accuracy and reproducibility of voltage (kV) values provided by the X-ray machines employed were previously evaluated using quality protocols devised by the Brazilian National Ministry of Health(1111 Brasil. Ministério da Saúde. Diretrizes de proteção radiológica em radiodiagnóstico médico e odontológico. Portaria nº 453-98. Brasília, DF: D.O.U. 02/06/1998.,1212 Brasil. Ministério da Saúde. Agência Nacional de Vigilância Sanitária. Radiodiagnóstico médico: desempenho de equipamentos e segurança. Brasília, DF: Editora Anvisa; 2005.). The variation in the reproducibility of the voltage value was 0.1% for the equipment at both hospitals. However, in tests of the variance between the voltage supplied to the X-ray tube and the value indicated on the panel, the equipment employed at hospital A showed a variance of 2.2%, whereas the equipment employed in the two separate X-ray examination rooms at hospital B showed variances of 2.0% and 4.0%, respectively. The minimum, mean, and maximum current-time product (mAs) of the X-ray tubes used in the radiological examinations of the sinuses (in lateral, occipitofrontal, or occipitomental X-rays) are shown in Table 2.
Ka,e measured from the X-ray tube yield
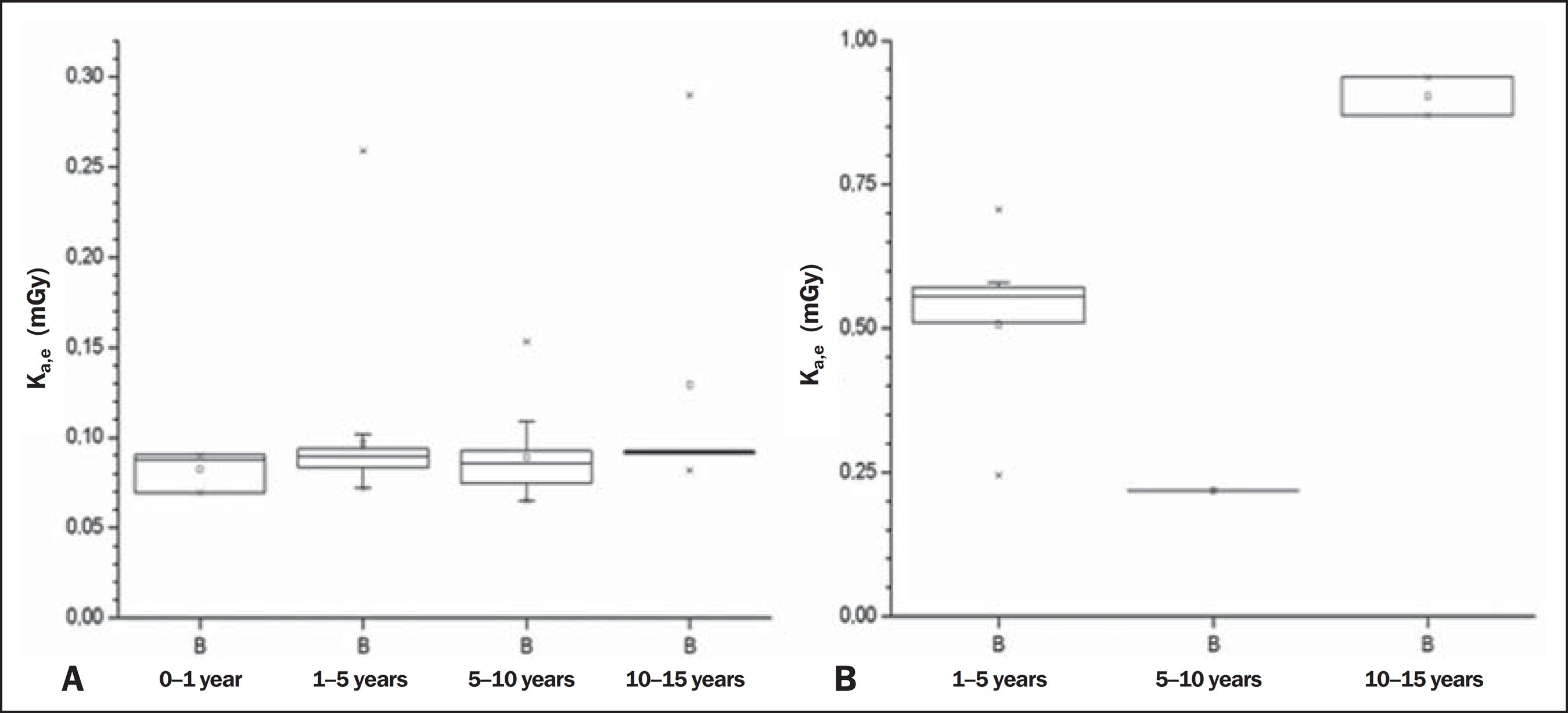
The distribution of the estimated Ka,e values in radiological examinations of the sinuses of pediatric patients is shown, by age group, in box and whisker plots in Figures 2A and 2B for lateral and posteroanterior (occipitofrontal or occipitomental) X-rays, respectively. In this distribution, the upper and lower borders of the rectangle correspond to the first and third quartiles (25% and 75% of the data, respectively). Therefore, the rectangle itself contains 50% of the data. The line inside the rectangle indicates the median and the rectangle indicates the mean. The whiskers indicate the maximum and minimum value of the data. Values outside the distribution (outliers) are indicated by asterisks. Posteroanterior X-rays of the sinuses are taken from two views-occipitofrontal and occipitomental-and the values shown correspond to the sum of the Ka,e for the two views in each patient. For better visualization, the distributions of the Ka,e values estimated for the lateral and posteroanterior X-rays of the sinuses obtained at hospital B are shown in Figures 3A and 3B, respectively.
Distribution of Ka,e values (in mGy) estimated for radiological examinations of the sinuses with lateral X-rays (A) and posteroanterior (occipitofrontal and occipitomental) X-rays (B), by age group, for the two hospitals participating in the study.
Distribution of Ka,e values (in mGy) estimated for radiological examinations of the sinuses in lateral (A) and posteroanterior (occipitofrontal and occipitomental) X-rays (B), by age group, for hospital B.
Doses near radiosensitive organs, as determined with thermoluminescent dosimeters
Figures 4A and 4B show the entrance and exit Ka,e values, respectively, for the area around the eyes of the patients in lateral (paranasal sinus) X-rays. Figures 5A and (5B show the estimated Ka,e values for the left and right eyes, respectively, in posteroanterior (occipitofrontal and occipitomental) X-rays. The distributions of the Ka,e values estimated for the thyroid region of pediatric patients submitted to lateral and posteroanterior (occipitofrontal and occipitomental) X-ray examinations of the sinuses are presented in Figures 6A and 6B, respectively.
Distribution of Ka,e values (in mGy) estimated for the area around the eyes, in relation to the primary X-ray beam entrance (A) and exit (B), in lateral X-rays of the sinuses.
Distribution of Ka,e values (in mGy) estimated for the area around the left eye (A) and the area around the right eye (B), in radiological examinations of the sinuses with posteroanterior (occipitofrontal and occipitomental) X-rays.
Distribution of Ka,e values (in mGy) estimated for the region of the thyroid in radiological examinations of the sinuses with lateral X-rays (A) and posteroanterior (occipitofrontal and occipitomental) X-rays (B).
DISCUSSION
For the sinus examinations evaluated, the irradiation parameters shown in Tables 1 and 2 were compared with the data presented in best practice guidelines developed in England(1313 Cook JV, Pettett A, Shah K, et al. Melhor prática em radiologia pediátrica: um manual para todos os serviços de radiologia. Rio de Janeiro, RJ: Editora Fiocruz; 2006.), which established quality criteria for such procedures. According to those guidelines, the voltage used for posteroanterior X-rays obtained in the occipitomental view should be 65 kV in patients 5-10 years of age and 78 kV for those 10-15 years of age, the use of such examinations not being recommended in patients under 5 years of age. The analysis of the results obtained in the present study showed that 25% of the posteroanterior X-rays obtained in the occipitomental view in patients 5-10 years of age, at both hospitals, were carried out at voltages higher than that recommended in the guidelines cited.
For lateral X-rays of the sinuses, the best practice guidelines advise the use of 62 kV for patients 1-5 years of age, 65 kV for those 5-10 years of age, and 70 kV for those 10- 15 years of age. The results of the present study show that the voltages employed were higher than the recommended values in over 80% of the examinations carried out at the two hospitals evaluated. That is attributable to the use of an antiscatter grid, which is not recommended for this age group, because there is no significant radiation scattering is such small patients. The use of an antiscatter grid requires the use of higher tube voltages to increase the penetrating power of the X-ray beam in order to achieve the same image quality.
Analyzing the Ka,e values estimated for lateral X-rays (Figure 2A), we observed that nearly all of the radiological examinations performed at hospital B were in accordance with the recommendations of the previously cited best practice guidelines, which recommends Ka,e values of 0 11 mGy, 0.16 mGy, and 0.37 mGy for patients 1-5 years of age, 5-10 years of age, and 10-15 years of age, respectively. Only 2% of the estimated Ka,e values for examinations performed at that hospital were above the recommended value, and all of those were in patients 1-5 years of age. However, all of the Ka,e values estimated for the radiological examinations performed at hospital A were above reference values specified in the best practice guidelines, up to 8 times higher in some cases.
For radiological examinations of the sinuses involving posteroanterior (occipitofrontal and occipitomental) X-rays Figures 2B and 3B), we also found the Ka,e values to be higher in the examinations performed at hospital A than in those performed at hospital B, and all of the values for the examinations performed at hospital A were higher than those recommended in the best practice guidelines, which suggest values of 0.34 mGy and 1.07 mGy for patients 5-10 years of age and 10-15 years of age, respectively.
The excessively high Ka,e values at hospital A, which were, in some cases, approximately 10 times higher than those observed for hospital B, are attributable to a number of factors. One such factor is the use of an antiscatter grid, which is not recommended for pediatric patients because it requires increases in voltage and current-time product, which can result in higher Ka,e values.
For every lateral X-ray of the sinuses requested at hospital A, the X-ray technicians obtained images of the patient in two conditions: with the mouth closed and with the mouth open. To our knowledge, there is no mention in the literature of any difference or benefit related to performing the examination with an open or closed mouth in terms of the visualization of structures or the facility of making a clinical diagnosis. The practice serves only to double the Ka,e.
It was noted also that the focus-to-skin distances employed were smaller at hospital A than at hospital B, which also contributed to the higher Ka,e values at the former. In the radiological examinations of the sinuses involving lateral X-rays in patients between 1 and 5 years of age, the mean focus-to-skin distance was 73.4 cm at hospital A, compared with 97.0 cm at hospital B.
Given that hospital A utilizes cylindrical collimators in examinations of the sinuses, we expected the air kerma values near the eyes to be lower at hospital A than at hospital B (Figures 4 and 5). However, our results show that, excluding the lateral X-rays in patients 10-15 years of age and posteroanterior X-rays in patients 1-5 years of age, the air kerma values near the eyes were actually higher at hospital A than at hospital B. That difference can be explained by the data in Table 2, which shows that, for posteroanterior (occipitomental and occipitofrontal) X-rays, the mAs values used at hospital A were approximately three times higher than those used at hospital B. We also found that, at hospital A, lateral X-rays of the sinuses were obtained in two conditions (open-mouth and closed-mouth).
Recent epidemiological studies of the effects of ionizing radiation have considered the occurrence of late, noncarcinogenic effects related to tissue changes. Consequently, the International Commission on Radiological Protection (ICRP) has issued new recommendations based on the latest knowledge on the biological effects of radiation(1414 International Commission on Radiological Protection. ICRP ref 4825-3093-1464. Statement on tissue reactions. Approved by the Commission on April 21, 2011.), notable among which is the new limit for the lens of the eye-0.5 Gy. Therefore, even though the air kerma values found in the present study were below the new limits established by the ICRP, it is always important to optimize the radiographic procedure in order to reduce the dose around the eyes, because of the high radiosensitivity of these organs.
Among the radiological examinations of the sinuses performed at hospital A, the air kerma values in the thyroid region were higher during lateral X-ray examinations (Figure 6A) than during posteroanterior X-ray examinations (Figure 6B). That is attributable to the fact that the location of the thyroid puts it directly in the path of the primary X-ray beam when the head of the patient is in profile.
As for the area around the eyes, air kerma values in the thyroid region during lateral X-rays were higher at hospital A than at hospital B, with the exception of those obtained for examinations performed in patients 10-15 years of age. This again contraindicates the use of cylindrical collimators (as were used at hospital A), for the reasons set forth above.
There has been little research on the risk of thyroid cancer due to radiological examinations. Most studies of thyroid cancer risk related to radiation exposure have dealt with the accidents at Chernobyl and Fukushima or with survivors of the atomic bombings of Hiroshima and Nagasaki(1515 Yamashita S, Suzuki S. Risk of thyroid cancer after the Fukushima nuclear power plant accident. Respiratory Investigation. 2013;51: 128-33.) - (1717 Sinnott B, Ron E, Schneider AB. Exposing the thyroid to radiation: a review of its current extent, risks, and implications. Endocr Rev. 2010;31:756-73.). Studies on the effects that exposure to low doses of radiation has on the thyroid have dealt with changes in its functioning, such as the onset of autoimmune diseases and cysts, especially in female patients(1818 Memon A, Godward S, Williams D, et al. Dental x-rays and the risk of thyroid cancer: a case-control study. Acta Oncol. 2010;49:447-53.).
CONCLUSION
The results of the present study allow us to conclude that, at the two hospitals under study, the irradiation parameters, especially kV and mAs, are higher than those recommended in best practice guidelines. The high values of these parameters are associated with the unnecessary use of antiscatter grids, which are not recommended for examinations in patients under 10 years of age. Cylindrical collimators (for restricting the irradiation field size), the use of which is recommended for radiological examination of the sinuses, were used only by the staff at hospital A. Despite this protection, the K a,e values obtained for the examinations performed at that hospital were well above the value suggested in the best practice guidelines, up to eight times higher in some cases. At both hospitals, optimization strategies are called for, in order to minimize patient exposure to radiation and thus reduce the risk of deleterious effects.
-
Cantalupo BLVC, Xavier ACS, Silva CML, Andrade MEA, Barros VSM, Khoury HJ. Dosimetric evaluation of X-ray examinations of paranasal sinuses in pediatric patien. Radiol Bras. 2016 Mar/Abr;49(2):79-85.
-
*
Study conducted at the Universidade Federal de Pernambuco (UFPE), Recife, PE, Brazil.
Acknowledgments
The authors thank the physicians, radiology technicians, nurses, directors, and other professionals at the hospitals evaluated. This study received financial support in the form of graduate research grants from the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (Capes) (Brazilian Office for the Advancement of Higher Education) and from the Fundação de Amparo à Ciência e Tecnologia do Estado de Pernambuco (Facepe) (Foundation for the Support of Scientific and Technological Development in the state of Pernambuco).
REFERENCES
-
1[No authors listed]. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Ann ICRP. 2007;37(2-4):1-332.
-
2Tagaya M, Nakata S, Yasuma F, et al. Relationship between adenoid size and severity of obstructive sleep apnea in preschool children. Int J Pediatr Otorhinolaryngol. 2012;76:1827-30.
-
3Feres MF, Hermann JS, Sallum AC, et al. Radiographic adenoid evaluation - suggestion of referral parameters. J Pediatr (Rio J). 2014;90:279-85.
-
4T-Ping C, Weckx LLM. ENT care of children and adolescents in the Brazilian public healthy system in three different municipalities. Braz J Otorhinolaryngol. 2008;74:571-8.
-
5Vogler RC, Ii FJ, Pilgram TK. Age-specific size of the normal adenoid pad on magnetic resonance imaging. Clin Otolaryngol Allied Sci. 2000;25:392-5.
-
6Jacomelli M, Souza R, Pedreira Júnior WL. Abordagem diagnóstica da tosse crônica em pacientes não-tabagistas. J Bras Pneumol. 2003;29:413-20.
-
7Bontrager KL. Tratado de técnica radiológica e base anatômica. 4ª ed. Rio de Janeiro, RJ: Guanabara Koogan; 1999.
-
8Davies M, McCallum H, Whiter G, et al. Patient dose audit in diagnostic radiography using custom designed software. Radiography. 1997;3:17-25.
-
9Petoussi-Henss N, Zankl M, Drexler G, et al. Calculation of back-scatter factors for diagnostic radiology using Monte Carlo methods. Phys Med Biol. 1998;43:2237-50.
-
10Associação Brasileira de Normas Técnicas. ABNT NBR ISO/IEC 17025:2005 - Requisitos gerais para a competência de laboratórios de ensaio e calibração. ABNT; 2005.
-
11Brasil. Ministério da Saúde. Diretrizes de proteção radiológica em radiodiagnóstico médico e odontológico. Portaria nº 453-98. Brasília, DF: D.O.U. 02/06/1998.
-
12Brasil. Ministério da Saúde. Agência Nacional de Vigilância Sanitária. Radiodiagnóstico médico: desempenho de equipamentos e segurança. Brasília, DF: Editora Anvisa; 2005.
-
13Cook JV, Pettett A, Shah K, et al. Melhor prática em radiologia pediátrica: um manual para todos os serviços de radiologia. Rio de Janeiro, RJ: Editora Fiocruz; 2006.
-
14International Commission on Radiological Protection. ICRP ref 4825-3093-1464. Statement on tissue reactions. Approved by the Commission on April 21, 2011.
-
15Yamashita S, Suzuki S. Risk of thyroid cancer after the Fukushima nuclear power plant accident. Respiratory Investigation. 2013;51: 128-33.
-
16Leung AM. The dose of ionizing radiation during childhood is associated with the prevalence of thyroid nodules even nearly 60 years later. Clinical Thyroidology. 2015;27:37-9.
-
17Sinnott B, Ron E, Schneider AB. Exposing the thyroid to radiation: a review of its current extent, risks, and implications. Endocr Rev. 2010;31:756-73.
-
18Memon A, Godward S, Williams D, et al. Dental x-rays and the risk of thyroid cancer: a case-control study. Acta Oncol. 2010;49:447-53.
Publication Dates
-
Publication in this collection
Mar-Apr 2016
History
-
Received
07 May 2015 -
Accepted
30 June 2015