
Abstract
The aims of this study were: a) to check if there is difference between muscle thickness measured by ultrasonography at three different sites, elbow flexors and knee extensors of patients with Parkinson's disease (PD); b) to check if there is correlation between muscle thickness and functional performance in patients with PD. Muscle thickness was assessed by ultrasonography at three anatomical sites in elbow flexors (proximal - EF1, medial, EF2, and distal - EF3) and knee extensors (proximal - EK1, medial - EK2, and distal - EK3), as well as functional performance assessment (chair stand and arm curl) of 31 patients with PD. The results suggest that EF3 muscle thickness was significantly (p> 0.05) lower than EF2 and EF1. Muscle thickness of knee extensors was statistically different in the anatomical points of rectus muscles and vastus medialis muscles (EK1>EK2>EK3). There was no correlation between muscle thickness and functional performance of lower (r= 0.17; p= 0.35) and upper limbs (r= -0.17; p= 0.34) of PD patients. The results indicate that the anatomical point has significant influence on the muscle thickness of elbow flexors and knee extensors of patients with PD. Thus, the careful determination of the evaluation of muscle thickness sites is a key variable when the goal is to quantify muscle thickness in patients with PD.
Key words
Functional performance; Parkinson’s disease; Quadriceps muscle; Ultrasonography
Resumo
Os objetivos do presente estudo foram: a) testar se existe diferença entre os valores de espessura muscular mensurados por ultrassonografia em três diferentes pontos, nos músculos flexores de cotovelo e extensores do joelho em pacientes com doença de Parkinson (DP); b) Testar se existe correlação entre a espessura muscular e desempenho funcional em pacientes com DP. A medida de espessura muscular foi avaliada por ultrassonografia em três pontos anatômicos nos flexores de cotovelo (proximal – FC1, médio, FC2, e distal – FC3) e extensores de joelho (proximal – EJ1, medial - EJ2, e distal – EJ3), além da avaliação do desempenho funcional (teste de sentar e levantar, e flexão de cotovelo) de 31 pacientes (64.6 ± 10.6 anos de idade) com DP. Os resultados sugerem que a espessura muscular do ponto FC3 foi significativamente (p>0.05) menor que os valores do ponto FC2 e FC1. A espessura muscular dos extensores do joelho foi estatisticamente diferente nos pontos anatômicos dos músculos reto da coxa e vasto intermédio (EJ1>EJ2>EJ3). Não houve correlação entre a espessura muscular e o desempenho funcional dos membros inferiores (r= 0.17; p= 0.35) e superiores (r= -0.17; p= 0.34) de pacientes com DP. Os resultados do nosso estudo indicam que o ponto anatômico de mensuração exerce influência significativa na espessura muscular dos flexores do cotovelo e extensores do joelho de pacientes com DP. Desta forma, a determinação criteriosa dos locais de avaliação da espessura muscular é uma variável fundamental, quando o objetivo é quantificar a espessura muscular em pacientes com DP.
Palavras-chave
Desempenho funcional; Doença de parkinson; Músculo quadríceps; Ultrassonografia
INTRODUCTION
Parkinson’s disease (PD) is considered the second most prevalent chronic neurodegenerative disease in the world, affecting approximately 6.1 million people in 201611 GBD 2016 Parkinson’s Disease Collaborators. Global, regional, and national burden of Parkinson’s disease, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2018;17(11):939-953.. PD is characterized by the death of doparminergic neurons in the substantia nigra and accumulation of alpha-synuclein neurotoxic aggregates in the central nervous system, triggering and worsening PD symptoms, such as: bradykinesia, tremor at rest, joint stiffness, impaired gait, among others22 Poewe W, Seppi K, Tanner CM, Halliday GM, Brundin P, Volkmann J, et al. Parkinson disease. Nat Rev Dis Primers 2017;23(3):17013..
The incidence of PD prevails in the elderly population, a stage of life that is physiologically characterized by morphofunctional changes such as: reduced functional capacity, strength and muscle mass. These changes appear to be maximized in patients with neurodegenerative diseases (e.g. Alzheimer’s and Parkinson’s disease).
Common in PD, reduced muscle mass (especially fast-contraction fibers) is associated with musculoskeletal disorders (e.g. sarcopenia), frailty33 Tan AH, Hew YC, Lim SY, Ramli NM, Kamaruzzaman SB, Tan MP, et al. Altered body composition, sarcopenia, frailty, and their clinico-biological correlates, in Parkinson's disease. Parkinsonism Relat Disord 2018;56:58-64., insulin resistance44 Dirks ML, Wall BT, van de Valk B, Holloway TM, Holloway GP, Chabowski A, et al. One week of bed rest leads to substantial muscle atrophy and induces whole-body insulin resistance in the absence of skeletal muscle lipid accumulation. Diabetes 2016;65(10): 2862-75., subclinical inflammation55 Peake J, Della Gatta P, Cameron-Smith D. Aging and its effects on inflammation in skeletal muscle at rest and following exercise-induced muscle injury. Am J Physiol Regul Integr Comp Physiol 2010;298(6):R1485-95. and decline in functional capacity66 Selva Raj I, Bird SR, Shield AJ. Ultrasound Measurements of Skeletal Muscle Architecture Are Associated with Strength and Functional Capacity in Older Adults. Ultrasound Med Biol 2017;43(3):586-594.. In this sense, the evaluation of morphological variables: types of muscle fibers, muscular cross-sectional area, as well as muscle thickness (MT) are clinically relevant77 Radaelli R, Neto ENW, Marques MFB, Pinto RS. Espessura e qualidade musculares medidas a partir de ultrassonografia: influência de diferentes locais de mensuração. Rev Bras Cineantropom Desempenho Hum 2011;13(2):87-93..
The study by Selva et al.66 Selva Raj I, Bird SR, Shield AJ. Ultrasound Measurements of Skeletal Muscle Architecture Are Associated with Strength and Functional Capacity in Older Adults. Ultrasound Med Biol 2017;43(3):586-594. demonstrated that the thickness of the femoral quadriceps in older adults, measured by ultrasound, was an independent and significant predictor of the isometric and isokinetic strength of knee extensors. In addition, the thickness of the medial gastrocnemius muscle was an independent and significant predictor of functional capacity (measured through timed up and go test, stair climb power, stair descent power and vertical jump height). Based on these findings, the authors reported that ultrasound is a safe, non-invasive and efficient method for inferring strength and functional capacity.
Thus, standardization of anatomical points seems to be a determining factor for obtaining reliable data. For example, Radaelli et al.77 Radaelli R, Neto ENW, Marques MFB, Pinto RS. Espessura e qualidade musculares medidas a partir de ultrassonografia: influência de diferentes locais de mensuração. Rev Bras Cineantropom Desempenho Hum 2011;13(2):87-93. assessed MT of 79 physically active men using ultrasound at three different points in the elbow flexor and knee extensor muscles. The results showed that the 1.5 cm difference between anatomical points has significant influence on MT.
To the best of our knowledge, no studies assessing MT of different anatomical points in the elbow flexor and knee extensor muscles in patients with PD were found in literature. Thus, the aims of this study were: a) to check whether there is difference between MT values measured by ultrasound at three different points in the flexor muscles of the elbow and knee extensors of PD patients; b) To check whether there is correlation between MT measures and functional performance (chair stand test and arm curl) in patients with Parkinson’s disease.
METHOD
Individuals who participated in this study were selected from a sample of 60 volunteers enrolled in the resistance training project for patients with PD. The following inclusion criteria were used: 1) Diagnosis of PD by a neurologist specialized in movement disorders, according to clinical criteria proposed by Gelb et al.88 Gelb DJ, Oliver E, Gilman S. Diagnostic criteria for Parkinson disease. Arch Neurol 1999;56(1):33–39.; 2) Age ≥ 45 years; 3) Stage 1–3 on the Hoehn and Yahr scale; 4) Stable use of medication; 5) Participants sedentary in the last 6 months. The following exclusion criteria were used: 1) Mini-Mental State Examination score99 Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12(3):189-198.<24; 2) Patient who has not completed all assessments.
Of the 60 PD patients initially considered for inclusion in the study, five were excluded due to discontinued medication, seven were classified in stages > 3 on the Hoehn and Yahr scale and 16 did not complete all evaluations. Thus, 31 patients (64.6 ± 10.6 years of age), of both sexes and with clinical diagnosis of idiopathic PD were included in the study.
Assessments
Functional tests were performed in two moments: familiarization with tests in the first moment and after the 48-hour interval, all patients underwent the retest following the same sequence (dynamometry, arm curl and sitting and standing) with the same evaluators. After five days, MT was measured by a single experienced evaluator.
Handgrip strength
Handgrip strength was assessed using dynamometry (Saehan Corporation, Yangdeok-Dong, Korea). In this test, the patient kept the dynamometer in the hand to be tested, with arm at right angles and the elbow at the side of the body. The dynamometer handle was adjusted if necessary. The base was fitted to the first metacarpal (heel of the palm). When ready, the subject pressed the dynamometer with isometric effort, which was maintained for approximately 5 seconds1010 Marin RV, Pedrosa MA, Moreira-Pfrimer LD, Matsudo SM, Lazaretti-Castro M. Association between lean mass and hand grip strength with bone mineral density in physically active postmenopausal women. J Clin Densitom 2010;13(1):96-101.. The patient was encouraged to perform maximum effort and no other body movement was allowed. One-minute interval between attempts was adopted (three measures on each limb) and the highest value was recorded.
Elbow flexion (30-second Biceps curls)
Patients started the test in a sitting position, with the trunk resting on the chair and feet resting on the floor. After command, the patient performed the greatest number of repetitions with the maximum possible amplitude (without compensation) for 30 seconds1111 Rikli RE, Jones CJ. Development and validation of a functional fitness test for community-residing older adults. J Aging Phys Activity 1999;7(2):129-61. The contralateral limb was supported on the thigh to avoid gripping on the chair. Two attempts were performed on the right limb (different days) and the highest value (highest number of repetitions) was recorded. Loads of 2 kg for women and 4 kg for men were adopted.
Chair stand
Patients started the test sitting on the chair (standard height of 44 cm), with trunk erect (without support on the back of the chair), feet resting on the floor and arms crossed on the trunk. After command, the patient performed as many repetitions as possible for 30 seconds. It was considered a repetition when the subject raised the trunk fully extending the knees, kept the trunk erect and sat down again, with only the need for minimal contact of hips on the chair1111 Rikli RE, Jones CJ. Development and validation of a functional fitness test for community-residing older adults. J Aging Phys Activity 1999;7(2):129-61. Two attempts were performed (different days) and the highest value was recorded.
Muscle thickness
MT (mm) was assessed using image obtained with an ultrasound device (Ultrasound Mindray M6, Shenzhen, China), with image being obtained in B-mode. During MT assessment, patients remained lying down with the assessed limb extended and relaxed. A transducer with sampling frequency of 7.5 MHz was perpendicularly and transversely positioned over the evaluated muscles. For image acquisition, water-based gel was used, which promotes acoustic contact without the need for pressure on the skin. During the test, any pressure from the transducer on the patient’s skin was avoided.
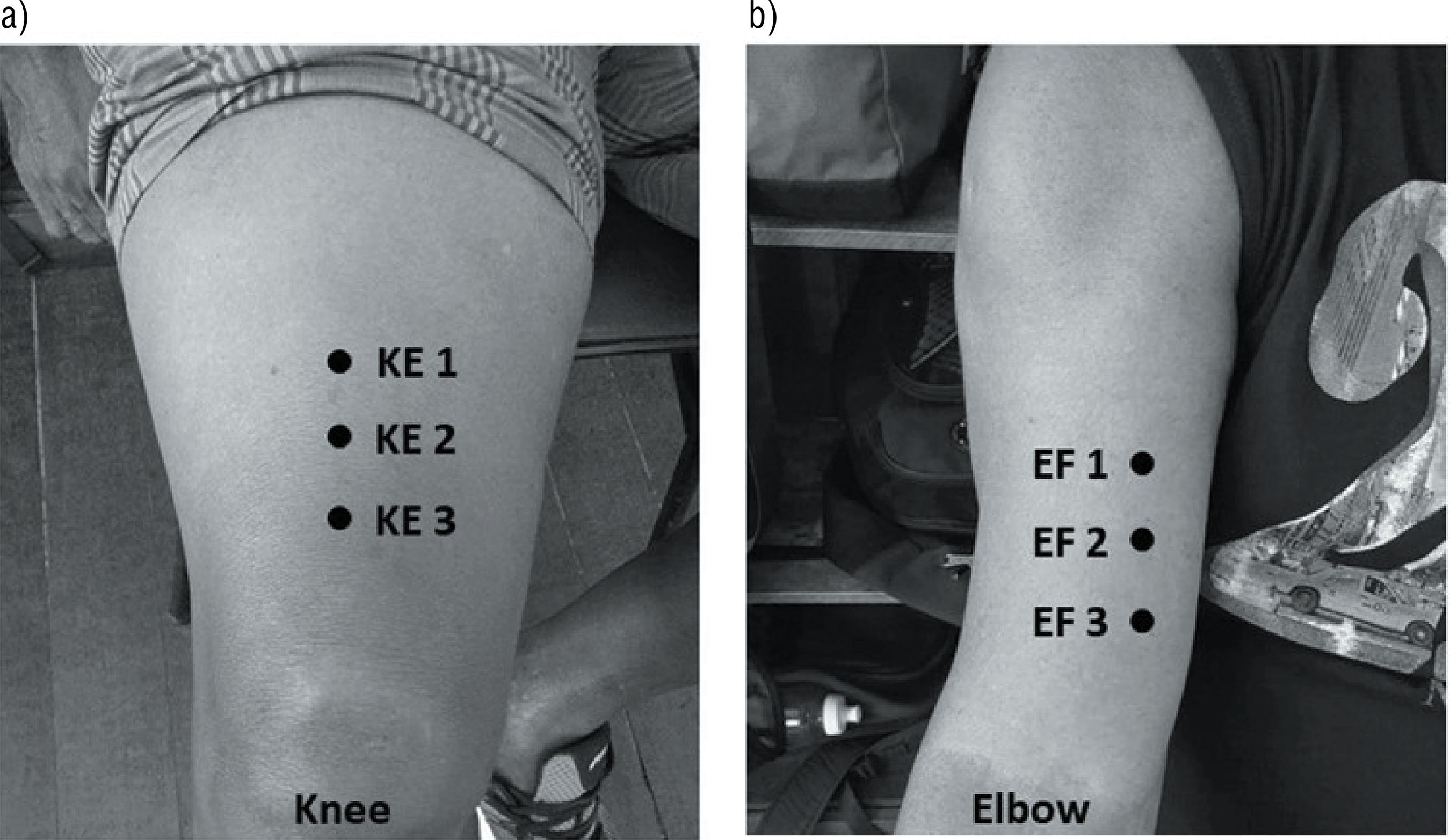
Subcutaneous adipose tissue and bone tissue were identified by ultrasound imaging, and the distance between these two points was defined as MT. The MT of biceps brachii and brachii muscles was assessed in the right segment and all measurements were performed by the same evaluator in triplicate (intraday intraclass correlation coefficient> 0.9). The main assessment point of elbow flexor muscles was performed according to proposition of Miyatani et al.1212 Miyatani M, Kanehisa M, Ito M, Kawakami Y, Fukunaga T. The accuracy of volume estimates using ultrasound muscle thickness measurements in different muscle groups. Eur J Appl Physiol 2004;91(2-3):264–272., at 50% of the distance between the elbow joint olecranon and the scapular acromial process, and was defined as EF2. In addition, two more points were used for correlations: EF3 and EF1, demarcated one centimeter and a half below and above EF2, respectively (figure 1a).
First, thigh length was measured (distance between the greater trochanter of the femur and the knee joint line), and then the region of 50% of this length was marked1313 Abe T, Dehoyos D, Pollock M, Garzarella L. Time course for strength and muscle thickness changes follow upper and lower body resistance training in men and women. Eur J Appl Physiol 2000;81(3):174-80.. Subsequently, the MT of rectus muscles and vastus medialis (knee extensor) muscles, defined as KE2, was measured. In addition, two more points were used for correlations: KE3 and KE1, demarcated one and a half centimeters from KE 2 (figure 1b). MT of knee extensors was assessed in the right segment and all measurements were performed by the same evaluator in triplicate (intraday intraclass correlation coefficient > 0.9).
Statistical analysis
Data obtained were submitted to statistical analysis to verify normality using the Shapiro-Wilk test. After data showed normal distribution, Pearson’s correlation coefficient was used to correlate values of physical tests (chair stand, elbow flexion), MT of elbow flexors and knee extensors. For the comparison between MT values obtained from the different points in each muscle, ANOVA was used for repeated measures with Bonferroni post hoc to identify the main differences. Data were analyzed using the SPSS 13.0 software and significance level of p <0.05 was adopted.
RESULTS
The sample characteristics are shown in table 1. Figure 2 shows that the MT of EF3 point was significantly lower than that of EF2 and EF1 points. Lower limb MT was statistically different at anatomical points of knee extensor muscles (figure 3).
The results presented indicate that there is no significant correlation between the chair stand test and MT of knee extensors (figure 4a), and elbow flexion test and MT of elbow flexors (figure 4b).
Relationship between the chair stand test and muscle thickness of knee extensors (a); Relationship between the elbow flexion test and muscle thickness of elbow flexors (b).
DISCUSSION
The main result of our study suggests that the anatomical measurement point has significant influence on the MT of PD patients. Interestingly, a difference of one and a half centimeters between anatomical points of elbow flexors and knee extensors has an influence on MT. That is, the lack of standardization and / or careful anatomical demarcation can underestimate or even overestimate MT.
Ultrasound has been used in several studies in order to measure MT and even edema, as an indirect structural and local marker1212 Miyatani M, Kanehisa M, Ito M, Kawakami Y, Fukunaga T. The accuracy of volume estimates using ultrasound muscle thickness measurements in different muscle groups. Eur J Appl Physiol 2004;91(2-3):264–272.
13 Abe T, Dehoyos D, Pollock M, Garzarella L. Time course for strength and muscle thickness changes follow upper and lower body resistance training in men and women. Eur J Appl Physiol 2000;81(3):174-80.-1414 Thiebaud RS, Yasuda T, Loenneke JP, Abe T. Effects of low-intensity concentric and eccentric exercise combined with blood flow restriction on indices of exercise-induced muscle damage. Interv Med Appl Sci 2013;5(2):53-59.. However, accuracy, reproducibility and uniformity of anatomical points must be considered in order to reduce bias. In addition, Matta et al.1515 Matta TT, Nascimento FX, Trajano GS, Simão R, Willardson JM, Oliveira LF. Selective hypertrophy of the quadriceps musculature after 14 weeks of isokinetic and conventional resistance training. Clin Physiol Funct Imaging 2017;37(2):137-142. in a longitudinal study, showed that the morphological adaptation resulting from resistance training occurs in a non-uniform way along the muscle, a process called selective hypertrophy. Thus, identifying MT in elbow flexors and knee extensors in more than one point provides a methodological contribution to ultrasound.
The results of our study also corroborate the findings of Radaelli et al.77 Radaelli R, Neto ENW, Marques MFB, Pinto RS. Espessura e qualidade musculares medidas a partir de ultrassonografia: influência de diferentes locais de mensuração. Rev Bras Cineantropom Desempenho Hum 2011;13(2):87-93., who assessed MT at three anatomical points of elbow flexors and three points of knee extensors in physically active men (26.9 ± 4.4 years; 67, 7 ± 8.1Kg; 169.1 ± 5.8cm). The results showed that the measurement point significantly affects MT in knee extensors and elbow flexors.
Our study evaluated a specific population, older adults with PD. In neuromuscular or neurodegenerative diseases, muscle tissue can be replaced by fibrous tissue (intramuscular fat), and consequently less MT. This process seems to be maximized in sedentary patients1616 Meghan EV, Melissa D, Michael EM, Cralen CD, Anthony PM, Katherine RS. Characterizing upper limb muscle volume and strength in older adults: A comparison with young adults. J Biomech 2012;45(2):334–341., increasing the risk for musculoskeletal disorders (e.g. sarcopenia).
Several studies have demonstrated the relationship between strength, power and functional capacity with MT in different populations66 Selva Raj I, Bird SR, Shield AJ. Ultrasound Measurements of Skeletal Muscle Architecture Are Associated with Strength and Functional Capacity in Older Adults. Ultrasound Med Biol 2017;43(3):586-594.,1717 Garcia P. Relation of functional capacity, strength and muscle mass in elderly women with osteopenia and osteoporosis. Fisioter Pesqui 2015;22(2):126–32.. In addition, ultrasound is considered an efficient and established tool to quantify changes in muscle architecture in the elderly1818 Morse CI, Thom JM, Birch KM, Narici MV. Changesintriceps surae muscle architecture with sarcopenia. Acta Physiol Scand 2005;183:291–298.,1919 Narici MV, Binzoni T, Hiltbrand E, Fasel J, Terrier F, Cerretelli P. In vivo human gastrocnemius architecture with changing joint angle at rest and during graded isometric contraction. J Physiol 1996;496(Pt 1): 287–297.. This information justifies the clinical relevance of MT and the need to standardize the anatomical measurement points by ultrasound for accurate analysis and monitoring.
Our study found no statistically significant correlation of MT and functional performance of sitting and standing and elbow flexion in patients with PD. These findings can be explained by the evidence found by Moroney et al.2020 Moroney R, Heida C, Geelen J. Increased bradykinesia in Parkinson's disease with increased movement complexity: elbow flexion-extension movements. J Comput Neurosci 2008;25(3):501-19., who, through a mathematical model of the circuit-cortex-ganglia basal-thalamus-cortex, analyzed the increase in bradykinesia on the performance of elbow flexion-extension movement, the authors demonstrated that the loss of dopaminergic neurons in the nigrostriatal pathway and the loss of functional segregation at striatal level between neurons in competing pathways contribute to bradykinesia, impairing the ability to perform complex movements and suppress unwanted movements, respectively.
Previous studies that correlated MT in the femoral quadriceps and performance in the chair stand test2121 Yohei T, Megumi O, Ryota A, Hiroaki K, Yasuo K, Tetsuo F. Sit-to-stand test to evaluate knee extensor muscle size and strength in the elderly: a novel approach. J Physiol Anthropol 2009;28(3):123-8.,2222 Akira S, Ryoichi E, Takayuki I, Sumiaki M, Shun O, Mitsuru H, et al. Anatomical cross-sectional area of the quadriceps femoris and sit-to-stand test score in middle-aged and elderly population: development of a predictive equation. J Physiol Anthropol 2017; 36:3. in elderly women have shown moderate (r = 0.70)2222 Akira S, Ryoichi E, Takayuki I, Sumiaki M, Shun O, Mitsuru H, et al. Anatomical cross-sectional area of the quadriceps femoris and sit-to-stand test score in middle-aged and elderly population: development of a predictive equation. J Physiol Anthropol 2017; 36:3. and strong positive correlation (r = 0.80)2121 Yohei T, Megumi O, Ryota A, Hiroaki K, Yasuo K, Tetsuo F. Sit-to-stand test to evaluate knee extensor muscle size and strength in the elderly: a novel approach. J Physiol Anthropol 2009;28(3):123-8. between these variables, suggesting that MT can predict the ability to generate skeletal muscle strength in the elderly. There are no other studies that have related the elbow flexion test and MT of elbow flexors, on the other hand, researches show positive association between MT of elbow flexors and the functionality of upper limbs1616 Meghan EV, Melissa D, Michael EM, Cralen CD, Anthony PM, Katherine RS. Characterizing upper limb muscle volume and strength in older adults: A comparison with young adults. J Biomech 2012;45(2):334–341.,2323 Melissa D, Meghan EV, Joel DE, Greg S, Michael EM, Anthony PM, Katherine RS. Upper extremity muscle volumes and functional strength after resistance training in older adults. J Aging Phys Act 2013;21(2):186–207.. Possibly, in our findings, the neuropathological impairment of PD has a direct influence, inducing low-amplitude movements and reducing speed in the chair stand and elbow flexion functional performance tests.
Finally, further investigations with samples larger than that of this study should be carried out in order to obtain better statistical analyses. We also recommend the inclusion of a control group to better interpret the results in future studies. Finally, our results cannot be extrapolated to other populations, since the present study was conducted with a specific population with PD.
CONCLUSIONS
The results of our study indicate that the anatomical measurement point has a significant influence on the MT of elbow flexors and knee extensors of PD patients. Thus, the careful determination of MT assessment sites is a fundamental variable, when the objective is to quantify MT in PD patients. In addition, no positive correlation was found between MT and functional performance in patients with PD.
COMPLIANCE WITH ETHICAL STANDARDS
-
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-profit sectors. This study was funded by the authors. -
Ethical approval
Ethical approval was obtained from the local Human Research Ethics Committee – Amazon University and the protocol (CAAE: 43624015.6.0000.517) was written in accordance with standards set by the Declaration of Helsinki.
How to cite this article
-
Abrahin O, Souza DM, Wilson-Mateus, Silva AF. Muscle thickness and functional performance of patients with Parkinson’sdisease. Rev Bras Cineantropom Desempenho Hum 2020, 22:e60774. DOI: http://dx.doi.org/10.1590/1980-0037.2020v22e60774
REFERENCES
-
1GBD 2016 Parkinson’s Disease Collaborators. Global, regional, and national burden of Parkinson’s disease, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2018;17(11):939-953.
-
2Poewe W, Seppi K, Tanner CM, Halliday GM, Brundin P, Volkmann J, et al. Parkinson disease. Nat Rev Dis Primers 2017;23(3):17013.
-
3Tan AH, Hew YC, Lim SY, Ramli NM, Kamaruzzaman SB, Tan MP, et al. Altered body composition, sarcopenia, frailty, and their clinico-biological correlates, in Parkinson's disease. Parkinsonism Relat Disord 2018;56:58-64.
-
4Dirks ML, Wall BT, van de Valk B, Holloway TM, Holloway GP, Chabowski A, et al. One week of bed rest leads to substantial muscle atrophy and induces whole-body insulin resistance in the absence of skeletal muscle lipid accumulation. Diabetes 2016;65(10): 2862-75.
-
5Peake J, Della Gatta P, Cameron-Smith D. Aging and its effects on inflammation in skeletal muscle at rest and following exercise-induced muscle injury. Am J Physiol Regul Integr Comp Physiol 2010;298(6):R1485-95.
-
6Selva Raj I, Bird SR, Shield AJ. Ultrasound Measurements of Skeletal Muscle Architecture Are Associated with Strength and Functional Capacity in Older Adults. Ultrasound Med Biol 2017;43(3):586-594.
-
7Radaelli R, Neto ENW, Marques MFB, Pinto RS. Espessura e qualidade musculares medidas a partir de ultrassonografia: influência de diferentes locais de mensuração. Rev Bras Cineantropom Desempenho Hum 2011;13(2):87-93.
-
8Gelb DJ, Oliver E, Gilman S. Diagnostic criteria for Parkinson disease. Arch Neurol 1999;56(1):33–39.
-
9Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12(3):189-198.
-
10Marin RV, Pedrosa MA, Moreira-Pfrimer LD, Matsudo SM, Lazaretti-Castro M. Association between lean mass and hand grip strength with bone mineral density in physically active postmenopausal women. J Clin Densitom 2010;13(1):96-101.
-
11Rikli RE, Jones CJ. Development and validation of a functional fitness test for community-residing older adults. J Aging Phys Activity 1999;7(2):129-61
-
12Miyatani M, Kanehisa M, Ito M, Kawakami Y, Fukunaga T. The accuracy of volume estimates using ultrasound muscle thickness measurements in different muscle groups. Eur J Appl Physiol 2004;91(2-3):264–272.
-
13Abe T, Dehoyos D, Pollock M, Garzarella L. Time course for strength and muscle thickness changes follow upper and lower body resistance training in men and women. Eur J Appl Physiol 2000;81(3):174-80.
-
14Thiebaud RS, Yasuda T, Loenneke JP, Abe T. Effects of low-intensity concentric and eccentric exercise combined with blood flow restriction on indices of exercise-induced muscle damage. Interv Med Appl Sci 2013;5(2):53-59.
-
15Matta TT, Nascimento FX, Trajano GS, Simão R, Willardson JM, Oliveira LF. Selective hypertrophy of the quadriceps musculature after 14 weeks of isokinetic and conventional resistance training. Clin Physiol Funct Imaging 2017;37(2):137-142.
-
16Meghan EV, Melissa D, Michael EM, Cralen CD, Anthony PM, Katherine RS. Characterizing upper limb muscle volume and strength in older adults: A comparison with young adults. J Biomech 2012;45(2):334–341.
-
17Garcia P. Relation of functional capacity, strength and muscle mass in elderly women with osteopenia and osteoporosis. Fisioter Pesqui 2015;22(2):126–32.
-
18Morse CI, Thom JM, Birch KM, Narici MV. Changesintriceps surae muscle architecture with sarcopenia. Acta Physiol Scand 2005;183:291–298.
-
19Narici MV, Binzoni T, Hiltbrand E, Fasel J, Terrier F, Cerretelli P. In vivo human gastrocnemius architecture with changing joint angle at rest and during graded isometric contraction. J Physiol 1996;496(Pt 1): 287–297.
-
20Moroney R, Heida C, Geelen J. Increased bradykinesia in Parkinson's disease with increased movement complexity: elbow flexion-extension movements. J Comput Neurosci 2008;25(3):501-19.
-
21Yohei T, Megumi O, Ryota A, Hiroaki K, Yasuo K, Tetsuo F. Sit-to-stand test to evaluate knee extensor muscle size and strength in the elderly: a novel approach. J Physiol Anthropol 2009;28(3):123-8.
-
22Akira S, Ryoichi E, Takayuki I, Sumiaki M, Shun O, Mitsuru H, et al. Anatomical cross-sectional area of the quadriceps femoris and sit-to-stand test score in middle-aged and elderly population: development of a predictive equation. J Physiol Anthropol 2017; 36:3.
-
23Melissa D, Meghan EV, Joel DE, Greg S, Michael EM, Anthony PM, Katherine RS. Upper extremity muscle volumes and functional strength after resistance training in older adults. J Aging Phys Act 2013;21(2):186–207.
Publication Dates
-
Publication in this collection
18 May 2020 -
Date of issue
2020
History
-
Received
22 Sept 2018 -
Accepted
19 Dec 2019

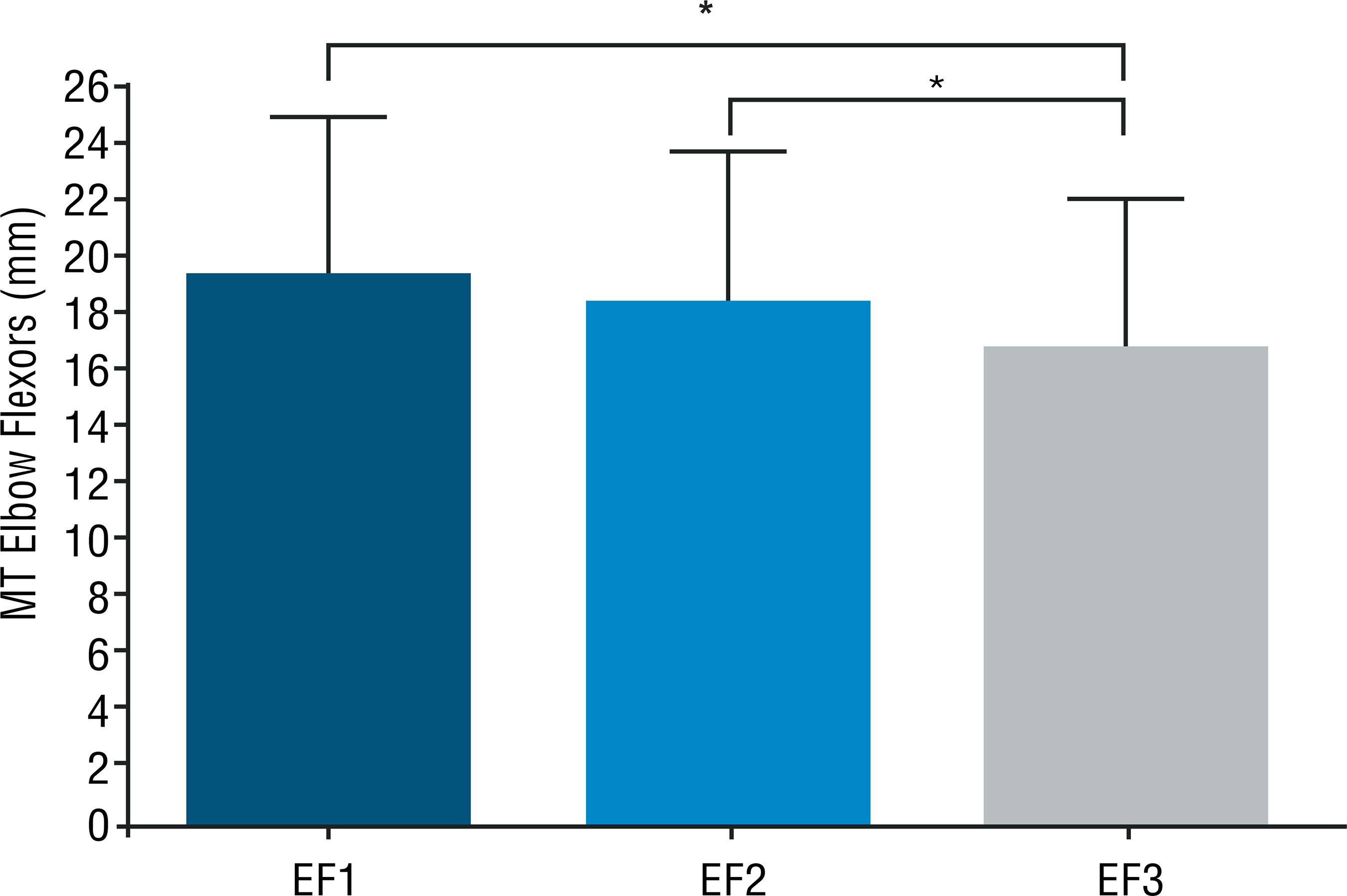 Legend = * significant difference (p <0.05).
Legend = * significant difference (p <0.05).
 Legend = * significant difference (p <0.05).
Legend = * significant difference (p <0.05).
