Introduction
Juvenile systemic sclerosis (JSSc) is an autoimmune disease, characterized by disordered collagen accumulation, leading to disseminated vascular lesions in skin and internal organs fibrosis, including the kidneys.11 Martini G, Foeldvari I, Russo R, Cuttica R, Eberhard A, Ravelli A, et al. Systemic sclerosis in childhood: clinical and immunologic features of 153 patients in an international database. Arthritis Rheum. 2006;54:3971-8.
2 Zulian F, Cuffaro G, Sperotto F. Scleroderma in children: an update. Curr Opin Rheumatol. 2013;25:643-50.-33 Foeldvari I, Tyndall A, Zulian F, Müller-Ladner U, Czirjak L, Denton C, et al. Juvenile and young adult-onset systemic sclerosis share the same organ involvement in adulthood: data from the Eustar database. Rheumatology (Oxford). 2012;51:1832-7.
Worthy of note, renal involvement is a rare manifestation and occurs in 1-12% of JSSc patients, mainly with arterial hypertension and/or proteinuria.11 Martini G, Foeldvari I, Russo R, Cuttica R, Eberhard A, Ravelli A, et al. Systemic sclerosis in childhood: clinical and immunologic features of 153 patients in an international database. Arthritis Rheum. 2006;54:3971-8.,33 Foeldvari I, Tyndall A, Zulian F, Müller-Ladner U, Czirjak L, Denton C, et al. Juvenile and young adult-onset systemic sclerosis share the same organ involvement in adulthood: data from the Eustar database. Rheumatology (Oxford). 2012;51:1832-7.
4 Scalapino K, Arkachaisri T, Lucas M, Fertig N, Helfrich DJ, Londino AV, et al. Childhood onset systemic sclerosis: classification, clinical and serologic features, and survival in comparison with adult onset disease. J Rheumatol. 2006;33:1004-13.-55 Aoyama K, Nagai Y, Endo Y, Ishikawa O. Juvenile systemic sclerosis: report of three cases and review of Japanese published work. J Dermatol. 2007;34:658-61. Scleroderma renal crisis was also rarely reported55 Aoyama K, Nagai Y, Endo Y, Ishikawa O. Juvenile systemic sclerosis: report of three cases and review of Japanese published work. J Dermatol. 2007;34:658-61.,66 Zulian F, Woo P, Athreya BH, Laxer RM, Medsger TA, Lehman TJ, et al. The Pediatric Rheumatology European Society/American College of Rheumatology/European League against Rheumatism Provisional Classification Criteria for Juvenile Systemic Sclerosis. Arthritis Rheum. 2007;57:203-12. and to our knowledge, nephrotic syndrome (NS) was described in only one JSSc patient with membranous nephropathy.77 Sarkar D, Sircar G, Waikhom R, Raychowdhury A, Pandey R, Ghosh A. Severe systemic sclerosis developing in a patient of membranous nephropathy. Rheumatology (Oxford). 2011;50:1522-3.
We report herein a patient who presented NS as the first manifestation of JSSc with focal segmental glomerulosclerosis (FSGS).
Case report
A female patient presented vomiting, malaise and generalized edema at the age of 12 years. She had systemic arterial hypertension, hypoalbuminemia (<2.5 mg/dL) and proteinuria (urine protein/creatinine ratio ≥2.0 mg/g). She was diagnosed with NS and treated with prednisone (60 mg/m2/day) with progressive reduction. During follow-up she had several relapses of NS, one of them associated to the upper respiratory tract infections and another one with spontaneous bacterial peritonitis, and was referred to our University Hospital at the age of 14. On the first admission at our service, she presented orbital and lower limbs edema, systemic arterial hypertension, sclerodactyly and proximal skin sclerosis. No muscle weakness and vasculitis were observed. Laboratory findings revealed serum albumin 0.9 g/dL (normal levels 3.8-5.6), total cholesterol 637 mg/dL (normal <199), low density lipoprotein (LDL) 439 mg/dL (normal <110), serum urea 18 mg/dL (normal 15-45), serum creatinine 0.53 mg/dL (normal 0.6-0.9), 25-hydroxyvitamin D 5 ng/mL (normal 30-100 ng/mL) and proteinuria 7.8 g/day. Hands X-ray revealed no bone abnormalities. Antinuclear antibodies (ANA), rheumatoid factor, and anti-Scl-70 (anti-topoisomerase I), anti-Sm, Anti-SS-A/Ro, Anti-SS-B/La and anti-smooth muscle (anti-SMA) antibodies were negative. C3 and C4 fractions of the complement system were normal. Serology for hepatitis A, B and C, human immunodeficiency virus (HIV), cytomegalovirus, Epstein-Barr virus and syphilis were negative. Echocardiogram was normal. Moderate capillary dilation and mild focal devascularization were observed in nailfold capillaroscopy, compatible with early stage of scleroderma (scleroderma pattern) (Fig. 1). Percutaneous renal biopsy guided by ultrasound revealed focal segmental glomerulosclerosis and direct immunofluorescence were negative (Fig. 2A and B). Therefore, she fullfilled the provisional classification criteria for JSSc.66 Zulian F, Woo P, Athreya BH, Laxer RM, Medsger TA, Lehman TJ, et al. The Pediatric Rheumatology European Society/American College of Rheumatology/European League against Rheumatism Provisional Classification Criteria for Juvenile Systemic Sclerosis. Arthritis Rheum. 2007;57:203-12. The patient was treated with oral 25-hydroxyvitamin D (800 IU/day), methotrexate (0.5 mg/kg/week) and amlodipin (0.15 mg/kg). Prednisone (60 mg/m2/day) was administered for 4 consecutive weeks, followed by alternate-day (40 mg/m2) for 2 consecutive months, with tapering for 4 months and then stopping this medication. Currently, she is being treated with methotrexate 15 mg/week, without edema and proteinuria.
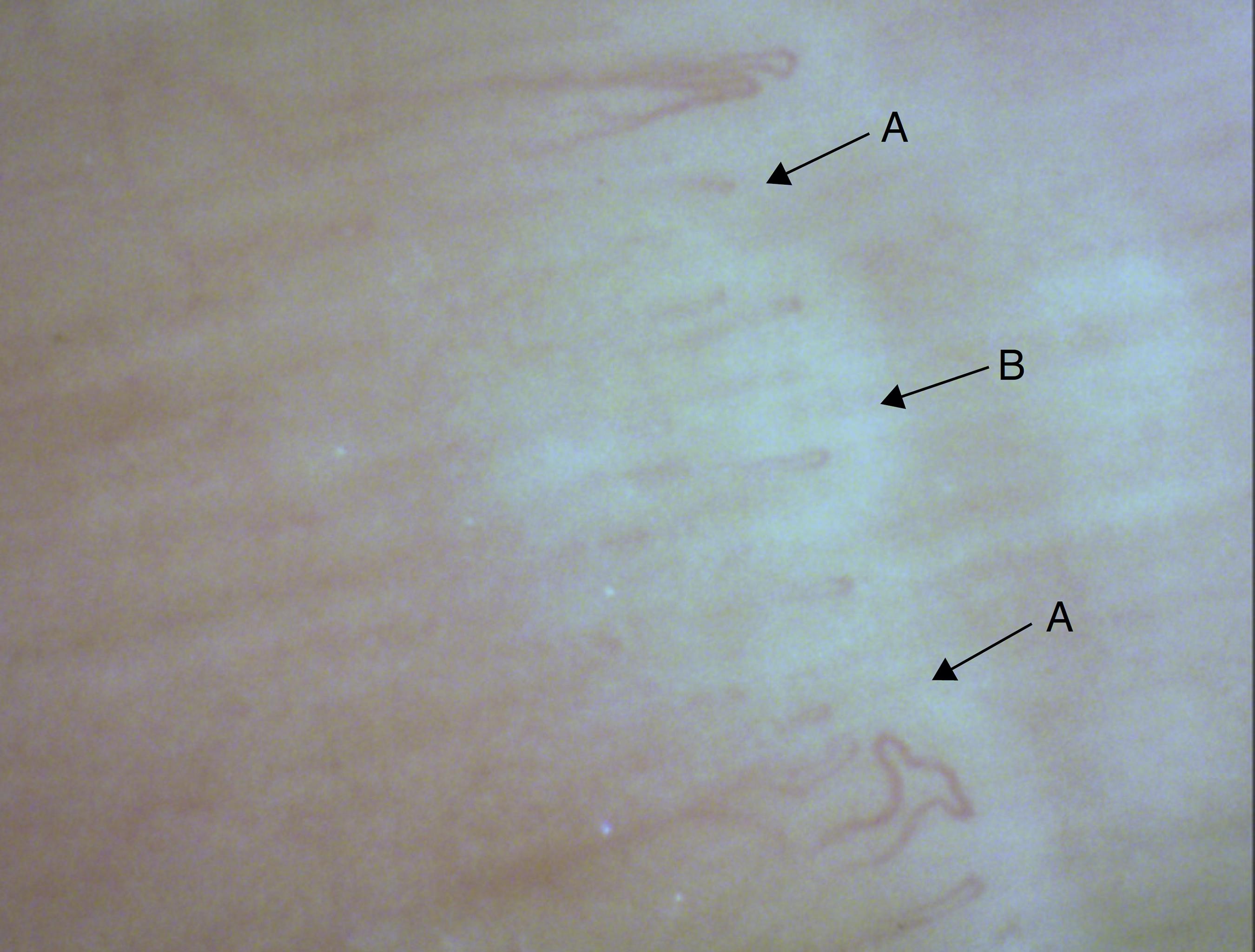
Nailfold capillaroscopy showing moderate capillary dilation (arrow A) and mild focal devascularization (arrow B) in patient with juvenile systemic sclerosis.
Optical microscopy in renal biopsy of patient with juvenile systemic sclerosis. (A) Histological findings in the Masson trichrome staining showing occasional wrinkling and thickening of glomerular basement membrane, causing double contour appearance in rare loops, segmental mesangial proliferation, mesangial matrix expansion, with tubular atrophy and interstitial. (B) Histological findings in the Silver staining showing occasional double contour appearance of glomerular basement membrane (arrow) fibrosis in less than 10% of glomeruli and normal vessels.
Discussion
To our knowledge, this was the first case reported with steroid-sensitive NS and FSGS as the first manifestation of JSSc.
The most important systemic manifestation of JSSc are cutaneous lesions, specially induration proximal to metacarpophalangeal joints, sclerodactly and edema,11 Martini G, Foeldvari I, Russo R, Cuttica R, Eberhard A, Ravelli A, et al. Systemic sclerosis in childhood: clinical and immunologic features of 153 patients in an international database. Arthritis Rheum. 2006;54:3971-8.,33 Foeldvari I, Tyndall A, Zulian F, Müller-Ladner U, Czirjak L, Denton C, et al. Juvenile and young adult-onset systemic sclerosis share the same organ involvement in adulthood: data from the Eustar database. Rheumatology (Oxford). 2012;51:1832-7.,44 Scalapino K, Arkachaisri T, Lucas M, Fertig N, Helfrich DJ, Londino AV, et al. Childhood onset systemic sclerosis: classification, clinical and serologic features, and survival in comparison with adult onset disease. J Rheumatol. 2006;33:1004-13. as observed in the present case. The capillaroscopy can be used to evaluate changes of microcirculation in the capillaries of the nail bed.88 Sato LT, Kayser C, Andrade LE. Nailfold capillaroscopy abnormalities correlate with cutaneous and visceral involvement in systemic sclerosis patients. Acta Reumatol Port. 2009;34:219-27. These findings strongly suggest systemic sclerosis diagnosis,88 Sato LT, Kayser C, Andrade LE. Nailfold capillaroscopy abnormalities correlate with cutaneous and visceral involvement in systemic sclerosis patients. Acta Reumatol Port. 2009;34:219-27. as evidenced herein, and not found in cutaneous scleroderma.99 Zulian F, Athreya BH, Laxer R, Nelson AM, Feitosa de Oliveira SK, Punaro MG, et al. Juvenile localized scleroderma: clinical and epidemiological features in 750 children. An international study. Rheumatology (Oxford). 2006;45:614-20.
Kidney involvement was rarely described in pediatric scleroderma population. The most frequent renal manifestations were arterial hypertension and proteinuria. Renal crisis in JSSc patients ranges from 0.7% to 4%.11 Martini G, Foeldvari I, Russo R, Cuttica R, Eberhard A, Ravelli A, et al. Systemic sclerosis in childhood: clinical and immunologic features of 153 patients in an international database. Arthritis Rheum. 2006;54:3971-8.,33 Foeldvari I, Tyndall A, Zulian F, Müller-Ladner U, Czirjak L, Denton C, et al. Juvenile and young adult-onset systemic sclerosis share the same organ involvement in adulthood: data from the Eustar database. Rheumatology (Oxford). 2012;51:1832-7.
4 Scalapino K, Arkachaisri T, Lucas M, Fertig N, Helfrich DJ, Londino AV, et al. Childhood onset systemic sclerosis: classification, clinical and serologic features, and survival in comparison with adult onset disease. J Rheumatol. 2006;33:1004-13.-55 Aoyama K, Nagai Y, Endo Y, Ishikawa O. Juvenile systemic sclerosis: report of three cases and review of Japanese published work. J Dermatol. 2007;34:658-61. This is a life-threatening complication with abrupt onset of malignant arterial hypertension, proteinuria and/or hematuria, thrombotic microangiopathy and potentially can result to end stage kidney disease.66 Zulian F, Woo P, Athreya BH, Laxer RM, Medsger TA, Lehman TJ, et al. The Pediatric Rheumatology European Society/American College of Rheumatology/European League against Rheumatism Provisional Classification Criteria for Juvenile Systemic Sclerosis. Arthritis Rheum. 2007;57:203-12.,1010 Kronbichler A, Mayer G. Renal involvement in autoimmune connective tissue diseases. BMC Med. 2013;11:95.,1111 Sabir O, Younas H, Tanvir I, Tarif N. Scleroderma renal crises: case report and review of literature. J Pak Med Assoc. 2013;63:916-8.
Adult scleroderma NS has a great spectrum varying from minimal changes disease and secondary amyloidosis to rapidly progressive renal failure and proliferative changes lesions with crescents, and membranous nephropathy. NS was only reported in one 12-year-old female patient who presented with scleroderma five years after the onset of this renal involvement with membranous nephropathy.77 Sarkar D, Sircar G, Waikhom R, Raychowdhury A, Pandey R, Ghosh A. Severe systemic sclerosis developing in a patient of membranous nephropathy. Rheumatology (Oxford). 2011;50:1522-3.
Importantly, our patient had steroid sensitive NS with a severe histological pattern of FSGS. This glomerulopathy is an important cause of proteinuria and chronic renal disease in children and adolescents, accounting in 5-15% of all cases of idiopathic NS.1212 D'Agati VD, Kaskel FJ, Falk RJ. Focal segmental glomerulosclerosis. N Engl J Med. 2011;365:2398-411.,1313 Lombel RM, Gipson DS, Hodson EM. Kidney disease: improving global outcomes treatment of steroid-sensitive nephrotic syndrome: new guidelines from KDIGO. Pediatr Nephrol. 2013;28:415-26.
The treatment of JSCc is performed according to organs and systems involvement. Methotrexate has been shown to improve skin scores in early diffuse SSc.1414 Rabinovich CE. Challenges in the diagnosis and treatment of juvenile systemic sclerosis. Nat Rev Rheumatol. 2011;7:676-80. Additionally, renal treatment of FSGS includes glucocorticoid and antihypertensive drugs, as used in our patient.1212 D'Agati VD, Kaskel FJ, Falk RJ. Focal segmental glomerulosclerosis. N Engl J Med. 2011;365:2398-411. Interestingly, the absence of proteinuria with complete remission after treatment suggests adequate renal long-term outcome.1313 Lombel RM, Gipson DS, Hodson EM. Kidney disease: improving global outcomes treatment of steroid-sensitive nephrotic syndrome: new guidelines from KDIGO. Pediatr Nephrol. 2013;28:415-26.
In conclusion, we reported a rare case of NS with FSGS as the first manifestation of scleroderma. Therefore, renal biopsy is mandatory in JSSc patients with sustained proteinuria or NS.
Acknowledgments
This study was supported by Fundação de Amparo à Pesquisa do Estado de São Paulo - FAPESP (grant #08/58238-4 to CAS), Conselho Nacional de Desenvolvimento Científico e Tecnológico - CNPq (302724/2011-7 to CAS), Federico Foundation to CAS and Núcleo de Apoio à Pesquisa "Saúde da Criança e do Adolescente" da USP (NAP-CriAd to CAS).
References
-
1Martini G, Foeldvari I, Russo R, Cuttica R, Eberhard A, Ravelli A, et al. Systemic sclerosis in childhood: clinical and immunologic features of 153 patients in an international database. Arthritis Rheum. 2006;54:3971-8.
-
2Zulian F, Cuffaro G, Sperotto F. Scleroderma in children: an update. Curr Opin Rheumatol. 2013;25:643-50.
-
3Foeldvari I, Tyndall A, Zulian F, Müller-Ladner U, Czirjak L, Denton C, et al. Juvenile and young adult-onset systemic sclerosis share the same organ involvement in adulthood: data from the Eustar database. Rheumatology (Oxford). 2012;51:1832-7.
-
4Scalapino K, Arkachaisri T, Lucas M, Fertig N, Helfrich DJ, Londino AV, et al. Childhood onset systemic sclerosis: classification, clinical and serologic features, and survival in comparison with adult onset disease. J Rheumatol. 2006;33:1004-13.
-
5Aoyama K, Nagai Y, Endo Y, Ishikawa O. Juvenile systemic sclerosis: report of three cases and review of Japanese published work. J Dermatol. 2007;34:658-61.
-
6Zulian F, Woo P, Athreya BH, Laxer RM, Medsger TA, Lehman TJ, et al. The Pediatric Rheumatology European Society/American College of Rheumatology/European League against Rheumatism Provisional Classification Criteria for Juvenile Systemic Sclerosis. Arthritis Rheum. 2007;57:203-12.
-
7Sarkar D, Sircar G, Waikhom R, Raychowdhury A, Pandey R, Ghosh A. Severe systemic sclerosis developing in a patient of membranous nephropathy. Rheumatology (Oxford). 2011;50:1522-3.
-
8Sato LT, Kayser C, Andrade LE. Nailfold capillaroscopy abnormalities correlate with cutaneous and visceral involvement in systemic sclerosis patients. Acta Reumatol Port. 2009;34:219-27.
-
9Zulian F, Athreya BH, Laxer R, Nelson AM, Feitosa de Oliveira SK, Punaro MG, et al. Juvenile localized scleroderma: clinical and epidemiological features in 750 children. An international study. Rheumatology (Oxford). 2006;45:614-20.
-
10Kronbichler A, Mayer G. Renal involvement in autoimmune connective tissue diseases. BMC Med. 2013;11:95.
-
11Sabir O, Younas H, Tanvir I, Tarif N. Scleroderma renal crises: case report and review of literature. J Pak Med Assoc. 2013;63:916-8.
-
12D'Agati VD, Kaskel FJ, Falk RJ. Focal segmental glomerulosclerosis. N Engl J Med. 2011;365:2398-411.
-
13Lombel RM, Gipson DS, Hodson EM. Kidney disease: improving global outcomes treatment of steroid-sensitive nephrotic syndrome: new guidelines from KDIGO. Pediatr Nephrol. 2013;28:415-26.
-
14Rabinovich CE. Challenges in the diagnosis and treatment of juvenile systemic sclerosis. Nat Rev Rheumatol. 2011;7:676-80.
Publication Dates
-
Publication in this collection
Nov-Dec 2017
History
-
Received
27 Feb 2014 -
Accepted
17 Aug 2014