Abstracts
BACKGROUND AND OBJECTIVES: Foot pain in elderly people may interfere with gait balance and cycle and may contribute for functional incapacity in the geriatric population. This study aimed at evaluating the frequency of functional incapacity associated to foot pain in elderly people. METHOD: Participated in this study 100 elderly people aged 60 years, with foot pain intensity of 30 mm by the pain visual analog scale (VAS). Types of feet and their injuries, types of shoes, falls, their circumstances and consequences were evaluated. Manchester Foot Pain Disability Index (MFPDI) and VAS at rest and movement, dynamic gait index and instrumental activity of daily life scale (IADL) were applied. Sperman and multiple regression tests were used for statistical analysis with significance level of 5% (p < 0.05). RESULTS: There has been prevalence of functional incapacity associated to foot pain above 50%. Univariate analysis has shown significant correlations of functional incapacity associated to foot pain and foot pain intensity at movement (p < 0.002), with the level of functional independence for IADL (p < 0.001), and with gait functionality, balance and risk for falls (p < 0.003), with significant association with the latter. The same correlations were significant in the multivariate analysis (p < 0.005). CONCLUSION: Functional incapacity associated to foot pain was highly prevalent in the elderly and was significantly correlated to foot pain intensity at movement, to the level of functional independence for IADL and to gait / balance functionality and risk for falls.
Elderly; Foot diseases; Pain
JUSTIFICATIVA E OBJETIVOS: O pé doloroso no idoso pode interferir no equilíbrio e no ciclo da marcha podendo ser um fator contribuinte para a incapacidade funcional na população geriátrica. O objetivo deste estudo foi avaliar a frequência de incapacidade funcional associada ao pé doloroso no idoso. MÉTODO: Cem participantes, com idade > 60 anos, dor no pé de intensidade > 30 mm pela escala analógica visual (EAV) de dor. Foram analisados os tipos de pés e suas lesões, tipos de calçados, ocorrência de queda, sua circunstância e consequência. Aplicado o Índice Manchester de Incapacidade Associada ao Pé Doloroso no Idoso (MFPDI) e a EAV ao repouso e movimento, Índice de Marcha Dinâmica (DGI), e Escala de Atividade Instrumental de Vida Diária (AIVD). Análise estatística com os testes de Spermann e regressão múltipla, com nível de significância em 5% (p < 0,05). RESULTADOS: Foi observada prevalência de incapacidade funcional associada ao pé doloroso maior que 50%. Na análise univariada houve correlações significantes da incapacidade funcional associada ao pé doloroso com intensidade de dor no pé ao movimento (p < 0,002), o nível de independência funcional para as AIVD (p < 0,001), e a funcionalidade de marcha, equilíbrio e risco de queda (p < 0,003), em relação a esta última variável, a associação foi importante. Na análise multivariada, as mesmas correlações mantiveram-se significantes (p < 0,05). CONCLUSÃO: A incapacidade funcional associada ao pé doloroso foi muito prevalente no idoso, e correlacionou-se significativamente com a intensidade da dor no pé em movimento, o nível de independência funcional para as AIVD, e a funcionalidade da marcha/equilíbrio e risco de queda.
Doenças do pé; Dor; Idoso
ORIGINAL ARTICLE
Foot pain in the elderly associated to functional incapacity*
Sabrina Canhada Ferrari PratoI; Fânia Cristina SantosII; Virgínia Fernandes Moça TrevisaniIII
IPhysical Therapist, Master and Doctor in Internal Medicine and Therapeutics, Federal University of São Paulo (UNIFESP). São Paulo, Brazil
IIGeriatrician, Master and Doctor in Medicine, Federal University of São Paulo (UNIFESP). São Paulo, SP, Brazil
IIIRheumatologist, Master and Doctor in Rheumatology, Federal University of São Paulo (UNIFESP). São Paulo, SP, Brazil
Correspondence to
SUMMARY
BACKGROUND AND OBJECTIVES: Foot pain in elderly people may interfere with gait balance and cycle and may contribute for functional incapacity in the geriatric population. This study aimed at evaluating the frequency of functional incapacity associated to foot pain in elderly people.
METHOD: Participated in this study 100 elderly people aged 60 years, with foot pain intensity of 30 mm by the pain visual analog scale (VAS). Types of feet and their injuries, types of shoes, falls, their circumstances and consequences were evaluated. Manchester Foot Pain and Disability Index (MFPDI) and VAS at rest and movement, dynamic gait index and instrumental activity of daily life scale (IADL) were applied. Spearman and multiple regression tests were used for statistical analysis with significance level of 5% (p < 0.05).
RESULTS: There has been prevalence of functional incapacity associated to foot pain above 50%. Univariate analysis has shown significant correlations of functional incapacity associated to foot pain and foot pain intensity at movement (p < 0.002), with the level of functional independence for IADL (p < 0.001), and with gait functionality, balance and risk for falls (p < 0.003), with significant association with the latter. The same correlations were significant in the multivariate analysis (p < 0.005).
CONCLUSION: Functional incapacity associated to foot pain was highly prevalent in the elderly and was significantly correlated to foot pain intensity at movement, to the level of functional independence for IADL and to gait / balance functionality and risk for falls.
Keywords: Elderly, Foot diseases, Pain.
INTRODUCTION
With aging, maintenance of autonomy is closely related to quality of life (QL). So, a way to quantify QL is by the level of autonomy with which people independently perform their daily activities within a socio-economic and cultural context.
A study states that aging while maintaining all functions is not a problem both for the individual and the community; when functions start to deteriorate is when problems start to appear because people loose their autonomy1. Among several problems affecting functional capacity, one of them is elderly foot pain. Evidences from detailed studies of several feet disorders suggest that 80% of the population have some feet problem2. Such problems bring some consequences to the elderly, such as: decreased strength and coordination, and worsen posture instability and the risk for falls, resulting in functional incapacity3.
Feet are convergence points of body weight during ambulation and have well detailed structures for such function. Such responsibility attributed to the feet make them more susceptible to injuries and deformities. These changes often generate posture instability and, as a consequence, falls3.
The major risk for falls is related to feet and shoes disorders4. A study carried out by these authors3 has shown that toe abnormalities, callosities and inadequate shoes may impair walking and increase the risk for falls.
Feet problems may directly interfere with balance and gait cycle, thus being a contributing factor for functional incapacity and falls in the geriatric population.
This study aimed at evaluating the frequency of functional incapacity related to foot pain in the elderly and the influence of related factors using the Manchester Foot Pain and Disability Index (MFPDI) to preserve autonomy and independence.
METHOD
After the project approval by the Research Ethics Committee (Opinion 0274/07), Federal University of São Paulo (UNIFESP), this study was carried out from March 2007 to December 2008.
This is a transversal, descriptive and analytical study carried out with a sample of 100 elderly people evaluated in the outpatient setting of the Discipline of Geriatrics and Gerontology, UNIFESP. Inclusion criteria were: age > 60 years, both genders, with foot pain intensity > 30 mm measured by the visual analog scale (VAS); pain at rest or movement and duration > 3 months. Exclusion criteria were irradiated or referred pain to the foot; amputation of lower limb and those who could not walk and had no understanding and motivation to participate in the study. They all signed the free and informed consent term.
An investigation protocol was used addressing variables such as: socio-demographic data, presence of falls, their circumstances and consequences, most commonly used type of shoe. We have also physically examined the feet to classify them in different types of feet and injuries.
In addition to this protocol, some tools were applied, such as:
MFPDI is divided into four subscales with 19 questions: 9 incapacity questions, 5 pain questions, 3 concern questions and 2 difficulty questions. For each question, patients have to point the frequency of feet symptoms in the last 30 days. If there is no incapacity the alternative "never, in any moment" should be marked. If present, one alternative "yes, in some days" or " yes, most/every day" should be chosen. Using the simple scoring strategy, all points are added to determine the incapacity level. MFPDI is scored as follows: "never in any moment" (score = 0), "yes, in some days" (score = 1) and " yes, most/every day" (score = 2). Score goes from 0 to 385.
VAS is a 100 mm line with anchors on both directions. One is "no pain" and the other is "maximum pain". Patients were oriented to choose the value best reflecting their feet pain in the last month at rest (rVAS) and movement (mVAS) and a ruler was used to measure pain from 0 to 100 mm. Line was horizontal with keywords throughout the scale6.
Dynamic gait index (DGI) consists of 8 tasks involving gait in different sensory contexts, which include leveled surface, changes in gait speed, horizontal and vertical head movements, cross or bypass obstacles, rotate around their own body axis, ascend and descend stairs. All patients were evaluated by an ordinal scale with 4 categories according to their performance in each task: severe impairment (0), moderate impairment (1), mild impairment (2) and normal gait (3). Maximum score is 24 points and a score below 19 points indicates risk for falls7.
Instrumental daily life activities scale (IDLA) consists of 9 questions regarding the use of telephone, trips, going shopping, preparing meals, domestic tasks, use of drugs and money handling. Scoring is as follows: dependence (1), capacity with help (2) and independence (3). Maximum score is 27 points representing the level of functional independence: independent (19 to 27 points); partially dependent, where they need some help (10 to 18 points) and totally dependent (1 to 9 points)8.
After evaluation, all participants were referred to specific and individual feet treatments.
A descriptive evaluation with absolute (N) and relative (%) frequencies was used for socio-demographic variables frequency, types of feet injuries, type of shoe, fall with circumstance and consequence, MFPDI, DGI and IDLA.
Median of central trend and interquartile interval (Q1 and Q3) for variability measurements were used for rest VAS and movement VAS.
MFPDI and investigation protocol were associated with Mann-Whitney and Kruskal-Wallis tests.
Spearman test (RS) was used for correlation analysis between foot pain-associated functional incapacity and other involved variables, and multiple regression model was used for variables significantly correlated in the previous model, considering statistically significant p < 0.05.
RESULTS
Sample was made up of 100 elderly with predominance of age group from 60 to 70 years (43%), females (85%) and Caucasians (60%).
Most frequent findings were 83% of talipes valgus and 52% of talipes planus. There has been 64% prevalence of skin injuries and from total sample, 63% had nail lesions and 53% presented toes deformities. Most frequently used shoes were sneakers and very soft shoes ("moleca") (29% each), sandals (22%), slippers (15%) and "mule" slippers (5%).
It has been observed that approximately 60 elderly have fallen at least once in previous year and from them, 27% have fallen twice or three times. According to circumstance, falls occurred at home (53%) or on the street (47%) and as to consequence, it has been observed that 22% of cases resulted in fractures, however 55% have resulted in no injury or in severe or moderate injuries, respectively between 18% and 27%.
Foot pain-associated functional incapacity frequency in the elderly according to MFPDI was < 50% (answer yes, in most / every day), except for questions IM1, IM5, IM9 and IM15 (Table 1).
As to foot pain intensity, medians were 80 mm by mVAS and 60 mm by rVAS. According to gait functionality and balance, and to risk for falls using DGI it was > 30%. There has been moderate functional impairment in the studied sample. Functional independence for IDLA has shown that > 60% of the sample were independent.
Association analysis has shown that foot pain-associated functional incapacity in the elderly was not significantly correlated with groups gender (U = 500.0; p = 0.18), dwelling (U = 484.5; p = 0.14), skin injuries (U = 1024.5; p = 0.36), nail lesions (U = 1140.5; p = 0.18); vascular lesions (U = 495.0; p = 0.170), toe deformities (U = 1173.0; p = 0.62), talipes planus (U = 1032.0; p = 0.16), talipes cavus (U = 987.0; p = 0.07), talipes varus (U = 145.0; p = 1.0), talipes valgus (U = 1146.5; p = 0.66), regular physical activities (U = 1098.0; p = 0.37) and fracture (U = 881.0; p = 0.65) through Mann Wallis test (U). With regard to talipes equinus there were no two groups because only one patient had talipes equinus.
Kruskall-Wallis test (H) was used to analyze the association of MFPDI to the investigation protocol for the following variables: race (H = 0.75; p = 0.86), marital status (H = 1.54; p = 0.82), number of falls (H = 0.34; p = 0.84), injuries caused by falls (H = 1.08; p = 0.58), place of the fall (H = 2.64; p = 0.46), room (H = 10.7; p = 0.15), time of the day (H = 3.26; p = 0.51), type of shoe (H = 2.82; p = 0.59) without statistically significant difference. Although general analysis of education groups (H = 10.3, p = 0.03) has shown p < 0.05, a posteriori analysis has not confirmed the reported difference because p value among groups was p > 0.05.
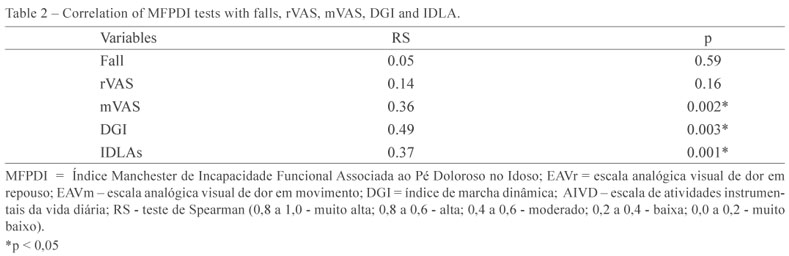
There were also no correlations with variables fall and rVAS. There have been low, however statistically significant correlations with mVAS (p < 0.002) and with the level of functional independence for IDLA (p < 0.001). There has been also statistically significant correlation with GDI (p < 0.003), however of moderate level (Table 2).
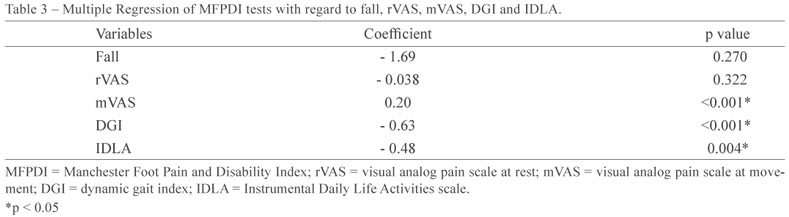
In a multiple regression model where variables significantly associated to foot pain-related functional incapacity were analyzed, that is variables fall rVAS, mVAS, DGI and IDLA, they were independently and significantly associated to MFPDI from the statistical point of view (Table 3).
DISCUSSION
In our study with the elderly followed up in the outpatient setting and with foot pain, most (85%) were females and this gender difference is clearly shown in the literature. There is a general consensus that females develop and report more feet problems than males. This may be attributed, first, to high heel and pointy shoes, which increase the chance of developing feet problems with aging, such as hallux valgus, toe deformities and callosities. Other aspect is tolerance to pain; females report more pain than males and as a consequence they look more often for health services9.
Major types of feet and their injuries in the elderly were talipes valgus and planus and skin / nail lesions and toe deformities. These data are similar to findings of a different study10 with 417 elderly aged above 60 years, which has observed 84% prevalence of dermatological feet affections and 86% of toe deformities. A different study11, also evaluating feet of 459 elderly with foot pain and aged 65 years or above, has reported a high prevalence of talipes valgus and toe deformities, in addition to the fact that foot pain was significantly correlated to those types of feet and deformities.
The high frequency of feet injuries in our study has an important role with regard to the elderly population, because as observed in different findings12, affections such as corns, ulcerations, toe deformities and talipes planus are clinically very frequent in the elderly, which may result in gait pattern changes, thus affecting their postural stability.
Our study has shown that only 29% of individuals used sneakers with more frequency, which is considered the most adequate and safer for the elderly. Most individuals (71%) used inadequate shoes especially very soft shoes ("moleca"), sandals, slippers and "mule" slippers. Elderly people in general choose shoes made of soft material with flexible structure, which seem to be more comfortable and to better accommodate painful feet deformities and such fact could contribute for the inadequate choice of shoes, since other factors, such as safety are more important.
Falls are a serious and common problem among the elderly and in our study 60% have reported falls in previous year; from them, 27% have fallen two or more times, characterizing the so-called "chronic faller". We have also observed that 22% of falls resulted in fractures. Studies13,14 have also reported that approximately 30% to 60% of community-dwelling elderly aged 65 years or above fall once a year, and 15% to 30% of them fall at least twice a year, which is similar to our findings.
Foot pain-related functional incapacity in the elderly was very frequent, which may become a very serious problem. In line with such findings, a study12 evaluating 172 elderly aged between 62 and 69 years has concluded that disabling foot pain was also very frequent and has also shown that females were more affected.
A population survey aiming at estimating foot pain frequency in Cheshire has observed that almost 100% of people reported disabling foot pain. Foot pain-related incapacity in that study was multifactorial and MFPDI was an effective tool to evaluate disabling foot pain in the elderly population in addition to being easy and fast to be applied12.
Foot pain intensity by VAS was not related to foot pain-related functional incapacity when pain was at rest; however there has been significant correlation when considering pain at movement. Foot pain intensity evaluation is very important, but no study was found in the literature with this interest. Since pain intensity impacts QL of the elderly, this aspect has been addressed.
DGI had significant correlation with MFPDI, that is, pain foot-related functional incapacity in the elderly could predispose to gait instability, unbalance and risk for falls, which are important consequences for the elderly. There are few studies in the literature applying DGI in the elderly with foot pain and these have not found correlations of DGI with feet problems in the elderly. Some studies have reported that the risk for falls was correlated to feet disorders. Toe abnormalities and deformities, and callosities are potential gait impairers, which may also increase the risk for falls and lead to fractures and daily life activities restrictions.
Our study has shown the same when using DGI, that is, disabling foot pain in the elderly was associated to the risk for falls, however the same correlation was not shown when variables were falls, their circumstances or consequences. But a study15 has shown that gait instability measured by DGI is a good indicator of the risk for falls in the elderly.
The level of functional independence for IDLA was correlated to MFPDI; this was a mild, however significant correlation from the statistical point of view. This is a very important finding for the elderly. Disagreeing from our data, a study11 has shown that disabling foot pain was not correlated to IDLA performance in 459 elderly aged 65 years or above and living in Italy.
Our study had some limitations which could influence results, such as the possible memory bias, since the elderly were asked about events of the previous year. Foot pain may represent additional impairments for the health of the elderly being a serious aging problem.
CONCLUSION
The prevalence of functional incapacity was high among evaluated elderly and was significantly and independently correlated to foot pain intensity at movement, to the level of functional independence to perform instrumental daily life activities and to gait / balance functionality and risk for falls.
ACKNOWLEDGMENTS
For their valuable contributions for this study, we acknowledge the Discipline of Internal Medicine and Therapeutic, the Centro Cochrane do Brasil and the Institute of Geriatrics and Gerontology (IGG) / Federal University of São Paulo (UNIFESP). São Paulo, SP.
REFERENCES
- 1. Kalache A, Veras RP, Ramos LR. The aging of the world population. A new challenge. Rev Saude Publica 1987;21(3):200-10.
- 2. Garrow AP, Papageorgiou AC, Silman AJ, et al. Development and validation of a questionnaire to assess disabling foot pain. Pain 2000;85(1-2):107-13.
- 3. Menz HB, Lord SR. The contribution of problems to mobility impairment and falls in older people. J Am Geriatr Soc 2001; 49(12):1651-6.
- 4. Kiely DR, Kiel DP, Burrows AB, et al. identifying nursing home residents at risk for falling. J Am Geriatr Soc 1998;46(5):551-5.
- 5. Menz HB, Tiedemann A, Kwan MM, et al. Foot pain in community-dwelling older people: an evaluation of the Manchester Foot Pain and Disability Index. Rheumatology 2006;45(7):863-7.
- 6. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain 1986;27(1):117-26.
- 7. Price DD. Psychological and neural mechanisms of pain. New York: Raven Press; 1988. p. 245-52.
- 8. Menz HB, Morris ME, Lord SR. Foot and ankle risk factors for falls in older people: a prospective study. J Gerontol A Biol Sci Med Sci 2006;61(8):866-70.
- 9. Gorecki GA. Shoe related foot problems and public health. J Am Podiatry Assoc 1978;68(4):245-7.
- 10. Helfand AE. Foot problems associated with older patients: a focused podogeriatric assessment study in ambulatory care. J Am Podiatr Med Assoc 2004;94(3):293-304.
- 11. Benvenuti F, Ferrucci L, Guralnik JM, et al. Foot pain and disability in older persons: an epidemiologic survey. J Am Geriatr Soc 1995; 43(5):479-84.
- 12. Menz HB, Morris ME, Lord SR. Foot and ankle characteristics associated with impaired balance and functional ability in older people. J Gerontol A Biol Sci Med Sci 2005;60(12):1546-52.
- 13. King MB, Tinetti ME. Falls in community-dwelling older persons. J Am Geriatr Soc 1995;43(10):1146-54.
- 14. Tromp AM, Smit JH, Deeg DJ, et al. Predictors for falls and fractures in the Longitudinal Aging Study Amsterdam. J Bone Miner Res 1998;13(12):1932-9.
- 15. Whitney SL, Hudak MT, Marchetti GF. The dynamic gait index relates to self-reported fall history in individuals with vestibular dysfunction. J Vestib Res 2000;10(2):99-105.
Publication Dates
-
Publication in this collection
29 Mar 2012 -
Date of issue
Mar 2012
History
-
Received
10 Oct 2011 -
Accepted
27 Jan 2012