Abstracts
BACKGROUND AND OBJECTIVES: Migraine is a highly prevalent primary headache affecting patients' quality of life. It may start in childhood or adolescence and follow patients throughout their lives. Triggering migraine crises factors, when identified, may help patients cope with external stimuli and may lead to a more effective treatment. This study aimed at observing whether climate changes in the region may be a potential triggering factor for migraine crises. METHOD: Prospective study including 60 migraine patients living in the city of Santos, SP, Brazil. Participants were selected according to migraine diagnostic criteria of the International Headache Society. Headache diary data were correlated to information supplied by Climatempo Santos. RESULTS: Forty-nine headache diaries comprising 104 days of prospective evaluation were developed and analyzed. Migraine crises were recorded in 96 days (92.3%). In 51 days, 10% or more of participants (> 5) presented migraine crises while in seven days 20% or more of participants (> 10) had migraine crises. Relative humidity was approximately 50% lower the day before the days of higher incidence of migraine crises (p < 0.001), when lower relative air pressure was also observed (p = 0.01). CONCLUSION: There has been correlation between low air pressure and low relative humidity and the prevalence of migraine crises the day after.
Climate; Headache; Migraine
JUSTIFICATIVA E OBJETIVOS: Enxaqueca é uma cefaleia primária altamente prevalente, afetando a qualidade de vida dos pacientes. Pode começar na infância ou adolescência e acompanhar o paciente por toda a sua vida. Os fatores desencadeantes das crises de enxaqueca, quando identificados, podem auxiliar o paciente a lidar com os estímulos externos e levar ao tratamento mais eficaz. O objetivo deste estudo foi observar se as alterações climáticas da região podem ser um potencial fator desencadeante de crises de enxaqueca. MÉTODO: Estudo prospectivo incluindo 60 pacientes que apresentam enxaqueca e moram na cidade de Santos, SP, Brasil. Os participantes foram selecionados de acordo com os critérios diagnósticos de enxaqueca da International Headache Society. Os dados dos diários de cefaleia foram correlacionados com as informações fornecidas pelo Climatempo Santos. RESULTADOS: Quarenta e nove diários de cefaleia abrangendo 104 dias de avaliação prospectiva foram devolvidos e analisados. Durante os 104 dias de estudo, foram registradas crises de enxaqueca em 96 dias (92,3%). Em 51 dias 10% ou mais dos participantes (> 5) apresentaram crises de enxaqueca, enquanto em sete dias 20% ou mais dos participantes (> 10) tiveram crise de enxaqueca. A umidade do ar foi praticamente 50% menor na véspera dos dias de maior incidência de crises de enxaqueca (p < 0,001), quando também se observou menor pressão relativa do ar (p = 0,01). CONCLUSÃO: Foi observada correlação entre a baixa pressão atmosférica e a baixa umidade do ar com a prevalência de crises de enxaqueca no dia seguinte.
Cefaleia; Clima; Enxaqueca
ORIGINAL ARTICLE
Influence of climate as triggering factor of migraine crises: prospective study*
Mayra Souza CampanaI; Barbara Scarpim MolinaI; Diogo Molina Troiano NetoI; Vitor WaismanI; Yára Dadalti FragosoII
IGraduating in Medicine, Metropolitan University of Santos. Santos, SP, Brazil
IIHead of the Neurology Department, School of Medicine, Metropolitan University of Santos. Santos, SP, Brazil
Correspondence to
SUMMARY
BACKGROUND AND OBJECTIVES: Migraine is a highly prevalent primary headache affecting patients' quality of life. It may start in childhood or adolescence and follow patients throughout their lives. Triggering migraine crises factors, when identified, may help patients cope with external stimuli and may lead to a more effective treatment. This study aimed at observing whether climate changes in the region may be a potential triggering factor for migraine crises.
METHOD: Prospective study including 60 migraine patients living in the city of Santos, SP, Brazil. Participants were selected according to migraine diagnostic criteria of the International Headache Society. Headache diary data were correlated to information supplied by Climatempo Santos.
RESULTS: Forty-nine headache diaries comprising 104 days of prospective evaluation were developed and analyzed. Migraine crises were recorded in 96 days (92.3%). In 51 days, 10% or more of participants (> 5) presented migraine crises while in seven days 20% or more of participants (> 10) had migraine crises. Relative humidity was approximately 50% lower the day before the days of higher incidence of migraine crises (p < 0.001), when lower relative air pressure was also observed (p = 0.01).
CONCLUSION: There has been correlation between low air pressure and low relative humidity and the prevalence of migraine crises the day after.
Keywords: Climate, Headache, Migraine.
INTRODUCTION
According to the International Headache Society1, migraine is a highly prevalent primary headache affecting more females than males, which may start during childhood or adolescence and follows patients throughout their lives1. Its study is important due to individual suffering and economic losses with direct costs with medical attention and drugs, and indirect costs with decreased productivity and absenteeism, although not being fatal2.
With estimated prevalence of 12% of the population and more than twice more frequent in females, migraine has a significant impact in economics and social well being of many people and nations around the world, including Brazil3. Migraine pathophysiology has not been totally explained4.
Major involved structures seem to be the central nervous system (CNS), the trigeminovascular system and corresponding vessels, other autonomic fibers innervating such vessels and different local vasoactive agents5. Genetic changes of a specific brain calcium channel lead to hyperexcitability with abnormal brain metabolism, making the CNS more susceptible to external light and olfactory stimuli and internal stimuli such as fasting and stress6.
Climate changes are among potential external factors which could trigger migraine crises7. The role of climate changes as a factor related to migraine crises is questionable7 and may depend much more on an individual sensitivity than on a factor common to patients8. However, in some studies, at least half the patients refer climate conditions as well-defined triggering factors8-10, while in other studies it seems clear that this is only true for a very specific subpopulation of migraine patients8.
To date, there are no Brazilian prospective studies specifically evaluating the role of climate as potential triggering factor of migraine crises. This study aimed at observing whether climate changes in Santos Lowlands may be triggering factors for migraine crises.
METHOD
After the approval of the Research Ethics Committee, Metropolitan University of Santos, SP, under n. 15/2011, CAAE: 0012.0.161.000-11, this prospective study was carried out with individuals aged from 18 to 60 years, with diagnosis of migraine who were not using and did not look for prophylactic treatment at inclusion time. Participants were selected for meeting 100% of migraine diagnostic requirements of the Brazilian Headache Society, based on the classification of the International Headache Society1. Individuals with other associated headaches or under prophylactic treatment were excluded.
After confirming that individuals really met all migraine diagnostic criteria, they received a headache diary to be filled for three consecutive months. Diary filling was individually explained and detailed. Climate details of temperature, pressure and relative humidity were obtained from the "Climatempo" service by the portals www.climatempo.com.br and www.cptec.inpe.br/cidades. Follow up period included 104 consecutive days from May 20 to August 31, 2011.
Student's t test and Pearson's correlation test for quantitative data were used for statistical analysis. Other descriptions were qualitative.
RESULTS
Initially, 100 individuals were selected for headache evaluation. From them, 60 had all migraine diagnostic criteria and had no other type of headache and were included in the study. Three months after, participants returned with their diaries with all details of the crises and 49 (82%) were thoroughly and accurately filled. Eleven participants did not complete the study for not having filled all data during the three months of follow up.
From the group of 49 participants, most were females (89.8%). Participants' age varied from 17 to 57 years (mean of 20 years and median of 25 years).
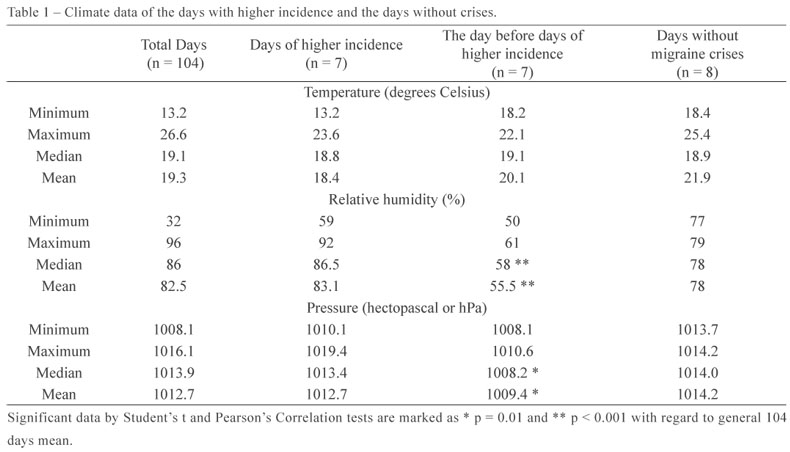
During these 104 days of study, there has been migraine complaint in 96 days (92.3%), varying from zero to 13 participants with migraine per day. In 51 days of this period, 10% or more of participants had migraine crises. In seven days of this period, 20% or more of participants had migraine crises (Table 1).
Temperature during studied days has varied between 13.2 and 26.6º C, with mean of 19.1º C. In the days of higher incidence of crises, more than 20% of participants had crises and mean temperature was 18.4º C. This mean was 20.1º C the day before the crises and 21.9º C in the days without reported crises.
Relative humidity during studied days has varied between 32% and 96%, with mean of 82.5%. In the days of higher incidence of crises, mean humidity was 83.1%, similar to the general mean of the 104 days. However, the day before the highest frequency of crises, mean relative humidity was 55.5%, typically 48% lower than the mean of all days and 40% lower than mean humidity in the days with no crises (p < 0.001 for both direct and correlation comparisons). There has been no significant difference between mean of all days (82.5%) and the days without recorded crises (78%) in terms of migraine crises observed by participants.
Mean relative pressure in studied days was 1016.1 hectopascal (hPa). We have to remind that the city of Santos is at sea level where the atmospheric pressure is really around 1000 hPa. The day before the higher incidence of migraine, mean pressure was even lower, of approximately 109.4 hPa (p = 0.01 for direct and correlation comparisons).
In summary, there has been lower atmospheric pressure and less relative humidity in the days preceding those with higher frequency of migraine crises in this population.
DISCUSSION
The difficulties to study climate changes related to a certain disease are not few. Climate varies every day and varies during the same day. Pressure, temperature and humidity as triggering factors of crises may have their effects masked by winds9, pollution10 or season11.
The correlation between migraine crises, even of higher intensity, with lower temperatures and higher humidity has been shown7, however a study10 has shown exactly the opposite, that is, higher temperatures and lower relative pressure were related to migraine crises. This study has shown that low relative humidity and low atmospheric pressure were related to a higher incidence of migraine crises, thus bringing totally different data from other mentioned studies. Since high atmospheric pressures are related to higher pollution rates, it seems that the air pollution factor, which has not been evaluated in this study, was not correlated, at least indirectly, to migraine crises evaluated by relative air pressure.
Considering a Brazilian study11 where there has been report of higher incidence of migraine crises during summer, at least 10% of participants had migraine crises.
Potential memory or medical record biases observed in several studies here mentioned for being retrospective and cohort studies, were minimized in our study which was prospective. The return of more than 80% of duly filled diaries for more than 100 days shows the interest of participants in observing potential triggering factors of their migraine crises.
Scientific evidence for climate changes as triggering factors for migraine crises is not conclusive according to world literature review.
CONCLUSION
This study has shown that low relative humidity and low atmospheric pressure were related to higher incidence of migraine crises the day after such climate changes.
REFERENCES
- 1. The international classification of headache disorders. 2nd ed. Cephalalgia 2004;24(Suppl 1):9-160.
- 2. Brandes JL. Migraine and functional impairment. CNS Drugs 2009;23(12):1039-45.
- 3. Queiroz LP, Peres MF, Piovesan EJ, et al. A nationwide population-based study of migraine in Brazil. Cephalalgia 2009;29(6):642-9.
- 4. Kelman L. The biological basis of headache. Expert Rev Neurother 2011;11(3):363-78.
- 5. Goadsby PJ. Pathophysiology of migraine. Neurol Clin 2009;27(2):335-60.
- 6. Cregg R, Momin A, Rugiero F, et al. Pain channelopathies. J Physiol. 2010;588(Pt 11):1897-904.
- 7. Hoffmann J, Lo H, Neeb L, et al. Weather sensitivity in migraineurs. J Neurol 2011;258(4):596-602.
- 8. Kelman L. The triggers or precipitants of the acute migraine attack. Cephalalgia 2007;27(5):394-402.
- 9. Prince PB, Rapoport AM, Sheftell FD, et al. The effect of weather on headache. Headache 2004;44(6):596-602.
- 10. Mukamal KJ, Wellenius GA, Suh HH, et al. Weather and air pollution as triggers of severe headaches. Neurology 2009;72(10):922-7.
- 11. Ierusalimschy R, Moreira Filho PF. Precipitating factors of migraine attacks in patients with migraine without aura. Arq Neuropsiquiatr 2002;60(3-A):609-13.
Publication Dates
-
Publication in this collection
29 Mar 2012 -
Date of issue
Mar 2012
History
-
Received
03 Nov 2011 -
Accepted
11 Feb 2012