Abstracts
This descriptive study was performed to identify the nursing diagnoses in the records of the inpatients of an adult intensive care unit, and map the most frequent diagnosis according to the Fundamental Human Needs. The sample consisted of 44 patient records. A total of 1,087 nursing diagnoses were identified. After excluding the repetitions, 28 different diagnoses were identified. Twenty-five diagnoses were related to psychobiological needs, and three to psychosocial needs. Further studies should identify, among the formulated nursing diagnoses and the affected human needs, which problems were solved and for what needs the care is predominantly developed. The present study results are important for the organization of teaching content for students and nurses, preparing them to consider human beings as a whole when providing care, considering their biological, emotional, and spiritual aspects.
Nursing care; Nursing Diagnosis; Classification; Intensive Care Units; Humanization of assistance
Estudo descritivo para identificar nos registros de prontuários de pacientes internados em uma Unidade de Terapia Intensiva de Adultos os diagnósticos de enfermagem e mapear os diagnósticos mais frequentes às Necessidades Humanas Básicas. Obteve-se uma amostra de 44 prontuários. Identificaram-se 1.087 diagnósticos de enfermagem. Após exclusão de repetições, encontraram-se 28 diferentes títulos de diagnósticos. Vinte e cinco diagnósticos estavam relacionados às necessidades psicobiológicas, e três, às necessidades psicossociais. Sugere-se a realização de estudos que identifiquem, entre os diagnósticos de enfermagem formulados e as necessidades humanas afetadas, quais foram solucionados e para quais necessidades são predominantemente elaborados os cuidados. Os resultados deste estudo são importantes para a organização de conteúdos de ensino para alunos e enfermeiros, preparando-os para que, ao prestar o cuidado, considerem o ser humano, tanto nos aspectos biológicos, como emocionais e espirituais.
Cuidados de enfermagem; Diagnóstico de Enfermagem; Classificação; Unidades de Terapia Intensiva; Humanização da assistência
Estudio descriptivo apuntando identificar en historias clínicas de pacientes internados en una Unidad de Terapia Intensiva de Adultos los diagnósticos de enfermería y mapear los diagnósticos más frecuentes relativos a las Necesidades Humanas Básicas. Se obtuvo una muestra de 44 historias clínicas. Se identificaron 1087 diagnósticos de enfermería. Luego de exclusión de repeticiones, se encontraron 28 diferentes títulos de diagnósticos. Veinticinco diagnósticos se relacionaban con necesidades psicobiológicas y tres a necesidades psicosociales. Se sugiere realizar estudios que identifiquen, entre los diagnósticos de enfermería formulados y las necesidades humanas afectadas, cuáles de ellos fueron solucionados y para cuáles necesidades son elaborados mayoritariamente los cuidados. Los resultados de este estudio son importantes para la organización de contenidos de enseñanza para alumnos y enfermeros, preparándolos para que al prestar el cuidado consideren al ser humano, tanto en aspectos biológicos como emocionales y espirituales.
Atención de enfermería; Diagnóstico de Enfermería; Clasificación; Unidades de Terapia Intensiva; Humanización de la atención
ORIGINAL ARTICLE
Nursing diagnoses identified in inpatients of an adult Intensive Care Unit
Tânia Couto Machado ChiancaI; Ana Paula Souza LimaII; Patrícia de Oliveira SalgadoIII
INurse. MsN, PhD. Full professor at the Federal University of Minas Gerais Nursing School. Belo Horizonte, Minas Gerais, Brazil. taniachianca@gmail.com
IINurse. Specialist in Emergency, Trauma and Intensive Care. Nurse in the Medimig Intensive Care Center and Belo Horizonte Military Police Hospital. Belo Horizonte, Minas Gerais, Brazil. anapsouzal@yahoo.com.br
IIINurse. MsN, PhD student in Nursing at the Federal University of Minas Gerais Nursing School. Nurse in the Management of Teaching and Research Unit of the Odilon Behrens Hospital. Belo Horizonte, Minas Gerais, Brazil. patriciaoliveirasalgado@gmail.com
Correspondence
ABSTRACT
This descriptive study was performed to identify the nursing diagnoses in the records of the inpatients of an adult intensive care unit, and map the most frequent diagnosis according to the Fundamental Human Needs. The sample consisted of 44 patient records. A total of 1,087 nursing diagnoses were identified. After excluding the repetitions, 28 different diagnoses were identified. Twenty-five diagnoses were related to psychobiological needs, and three to psychosocial needs. Further studies should identify, among the formulated nursing diagnoses and the affected human needs, which problems were solved and for what needs the care is predominantly developed. The present study results are important for the organization of teaching content for students and nurses, preparing them to consider human beings as a whole when providing care, considering their biological, emotional, and spiritual aspects.
Descriptors: Nursing care; Nursing Diagnosis; Classification; Intensive Care Units; Humanization of assistance
RESUMEN
Estudio descriptivo apuntando identificar en historias clínicas de pacientes internados en una Unidad de Terapia Intensiva de Adultos los diagnósticos de enfermería y mapear los diagnósticos más frecuentes relativos a las Necesidades Humanas Básicas. Se obtuvo una muestra de 44 historias clínicas. Se identificaron 1087 diagnósticos de enfermería. Luego de exclusión de repeticiones, se encontraron 28 diferentes títulos de diagnósticos. Veinticinco diagnósticos se relacionaban con necesidades psicobiológicas y tres a necesidades psicosociales. Se sugiere realizar estudios que identifiquen, entre los diagnósticos de enfermería formulados y las necesidades humanas afectadas, cuáles de ellos fueron solucionados y para cuáles necesidades son elaborados mayoritariamente los cuidados. Los resultados de este estudio son importantes para la organización de contenidos de enseñanza para alumnos y enfermeros, preparándolos para que al prestar el cuidado consideren al ser humano, tanto en aspectos biológicos como emocionales y espirituales.
Descriptores: Atención de enfermería; Diagnóstico de Enfermería; Clasificación; Unidades de Terapia Intensiva; Humanización de la atención
INTRODUCTION
The term 'Nursing Diagnosis' originated in the beginning of modern nursing, when Florence Nightingale, during the Crimean war, diagnosed and treated health problems among the soldiers, and used the surveying of these problems to plan their care(1).
With the advance of nursing and the organization of its own knowledge in the nineteen-fifties, nurses saved the experience of the epoch, with the objective of planning nursing's professional and educational practice, carrying out the care in a systematic way, that is, applying the nursing process (NP), which is composed of phases, in which the nursing diagnosis is included(1).
In Brazil, studies on the NP began to be developed with the pioneering work of Nurse Doctor Wanda de Aguiar Horta, who began discussions about the theory of Nursing in the professional field(2). The theoretical model which Horta proposed is termed the Theory of Basic Human Needs (BHN), and is described in organized, inter-related phases which provide data for nurses to plan their actions and provide care which is focused on the patients' needs(3).
The needs presented by the patients are identified by the nurses based on the collection of data. Through a process of clinical reasoning, needs are identified based on the interpretation and grouping of collected data, with nursing diagnoses being formulated and proposals for solving them being established. This process of reasoning is mental, and must be guided by the theoretical framework used where affected needs emerge.
Although nursing care is considered essential for the treatment of the majority of patients, this fact is neither very visible nor widely recognized. In care practice, one may observe the need to use the nurses to implement the Nursing Process in an effective way and with systematic actions. This reality has a greater impact, mainly, when one considers the Intensive Care Units (ICU). The reduced number of spaces and the high demand for these services, in addition to the number of procedures carried out, leads many to think again about the need for organization of actions undertaken and their follow-up. Besides this, in these units it is necessary to redirect the care, such that it might be focused on the human being and not merely on the illness or trauma which the patients are subjected to(5).
In an adult ICU in Belo Horizonte, Brazil, where the stages of the Nursing Process have been being implemented since 1996, the Theory of Basic Human Needs(3) is used as a theoretical framework and the nursing diagnoses are prepared based on NANDA-I's taxonomy II (4). However, even with the unit's nursing practice being guided by a theory, some problems relating to the covering of nursing care beyond the patient's biological aspects have been identified by the nurses in their practice. Supported by studies which establish the difficulty some nurses have in identifying aspects related to needs in the emotional and/or spiritual sphere as having priority in relation to the patients' physiological problems(6-8) concern grew about learning about the Basic Human Needs which are met in this ICU, based on the nursing diagnoses formulated for its patients.
This study's rationale is that the identification of a set of nursing diagnoses can guide the nursing care given to patients in ICU, supporting the elaboration of individualized care plans aimed at meeting the Basic Human Needs established mentally. Thus, the mapping of Basic Human Needs to the nursing diagnoses identified can contribute to the establishing of a diagnostic profile in the light of the theoretical framework adopted for the care of patients hospitalized in ICU. Knowledge of this profile is highly significant for the development of a nursing database to support a piece of software under construction and will favor the extraction of data to do with the efficacy of the nursing care provided in this unit.
In this way, the present study aims to identify, in the medical notes of the patients hospitalized in an adult ICU, the nursing diagnoses - and map the most frequent ones to Horta's Basic Human Needs.
METHOD
This is a descriptive study, developed in an adult ICU in the city of Belo Horizonte in the state of Minas Gerais. The unit has ten beds and provides care to private patients and those with private health insurance.
For the purposes of the study, the population was considered to be all the patients hospitalized in ICU in the period between 1st September 2008 and 30th September 2009 a total of 494 patients. The choice of this period was made because all the phases of the Nursing Process had been implemented, using specific forms, in the unit in this period.
The method of re-sampling by permutation(9) was used for calculating the sample. First of all, lots were drawn in order to make up a random sample composed of the nursing diagnoses from 60 sets of patients' notes. Of these, 16 sets of notes did not present formulated nursing diagnoses: these were excluded, producing a sample of 44 patients. Following this, for each patient, the number of nursing diagnoses formulated was identified and the average number of diagnoses exclusive to each patient was calculated. It was ascertained that for the first ten patients, there was an average of 19 different diagnoses, although, from the fifteenth patient on, a new diagnosis would appear once every two patients and around the fortieth patient there began to appear an average of less than 0.2 new nursing diagnoses per patient. Thus, the random sample was comprised of the patient notes of 44 patients, and this forms an estimate of the percentage of nursing diagnoses formulated by the nurses in the unit in this period.
The data was collected directly from the patient notes and transcribed individually into a spreadsheet from the program Excel for Windows, for the identification of the necessary information and the exclusion of repetitions. The nursing diagnoses obtained had their spelling corrected and underwent analysis for synonyms, correction of verb tenses, standardization of gender and number and exclusion of pseudo-terminological expressions, defined as elements which occur casually in discourse but which do not designate any particular concepts and have to be considered terminological trash(10).
The documented diagnoses were analyzed in terms of absolute and relative frequencies. In addition to this, a process of cross-mapping of the different nursing diagnostic titles collected was carried out with the classification of the BHN(3,11).
Cross-mapping is a methodological procedure which can be used in the analysis of data contained in the NP, in the different fields of care, through comparison between information found in the patients' notes and the reference classifications for nursing practice(12).
Once mapped, the nursing diagnoses were submitted to a process of validation, firstly by researchers from the Federal University of Minas Gerais' Center for Studies and Research into the Systematization of Nursing Care; following this, they were sent for evaluation by intensive care nurses and researchers in the area of the Systematization of Nursing Care (SNC), who agreed to participate in the study as experts, signing the Terms of Free and Informed Consent (TFIC).
The Delphi technique was used as a strategy for validating the process of mapping carried out this being a method for obtaining the consensus of a group of experts on a given subject(13). Although there is no guideline establishing the appropriate level of consensus to be obtained, (14), a minimum level of agreement of 70%, in the final stage of the Delphi technique, is recommended(15). Given this recommendation, the rate of 70% was adopted as a minimum level of consensus to be obtained by the experts in this study.
Two instruments were used in the process of validating the nursing diagnoses mapped: the first instrument had the necessary advice and the definitions of the BHN(11) and the second listed the titles of the nursing diagnoses collected and mapped to the BHN.
Eleven nurses were invited, via email, to undertake the validation of the nursing diagnoses mapped. On receiving the emails all eleven accepted to participate, and, also via email, received the material for validation (TFIC, an instrument with the guidance necessary for the validation and with the definitions of BHN, the instrument with the mapped nursing diagnoses and a sealed and addressed envelope for returning the TFIC). However, six of the nurses responded concerning the instrument within the arranged time and thus formed the study's sample of experts.
The study obtained favorable verdicts both from the senior management of the unit where the research was to take place and from the Federal University of Minas Gerais' Research Ethics Committee (Decision nº315/09), with the recommendations of Resolution 196/96 being followed.
RESULTS
Of the 44 patients whose notes were analyzed, the majority was female (30 people - 68%). The age range varied between 28 and 93, with 68.3% of the patients being 60 years old or over; the average age was 64, and the median age was 66.5. The standard deviation was 17.5 years. The predominant medical diagnoses were in line with the ICD-10(16), that is, illnesses of the respiratory system (30%).
Identification of the Nursing Diagnosis Labels
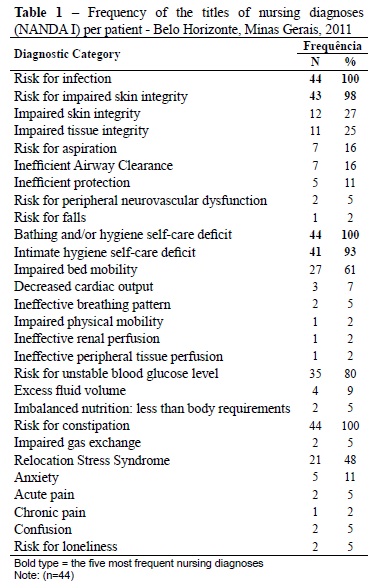
In total, 1087 nursing diagnoses were formulated for the 44 patients. After carrying out the process of content standardization, 28 different nursing diagnosis labels were obtained. (Table 1).
The nursing diagnosis labels were described in line with the 2008 Brazilian publication of the NANDA-I nursing diagnosis classification(17), as this was the edition used by the nurses to formulate the diagnoses of the patients hospitalized in the area of the study.
It may be observed that ten (36%) of the nursing diagnoses formulated were risk diagnoses. Among the 28 diagnoses identified, 7 had a frequency greater than 50%. Those with the highest frequencies were: Risk for Infection, deficit in self-care for bathing or hygiene, and Risk for constipation all of which were formulated for 100% of the patients. Other diagnoses also had high frequencies, namely: Risk for impaired skin integrity (98%), deficit in self-care for intimate hygiene (93%), Risk for unstable blood glucose level (80%) and Impaired bed mobility (61%).
Of the 13 domains of NANDA-I's Taxonomy II(4), 5 were not represented in any diagnosis, these being: Health Promotion, Role Relationships, Sexuality, Life Principles, Growth/development. The domains of Nutrition, Elimination and Exchange, Activity/Rest, Perception/cognition, Self-perception, Coping/Stress Tolerance, Safety/Protection and Comfort were represented by the occurrence of at least one of their respective diagnoses. The most-represented domains were Safety/Protection (9 different diagnostic labels) and Activity/Rest (7).
Mapping of the nursing diagnosis labels to the classification of Basic Human Needs
The nursing diagnosis titles formulated for the patients whose notes were analyzed were mapped to the BHN proposed by Horta(3) (Chart 1).
It may be seen in Chart 1 that, among the 28 different nursing diagnosis labels, 25 were mapped to psycho-biological needs; 3 to psychosocial needs, and none to psycho-spiritual needs. It may also be observed that the BHN of vascular regulation was compared to the greatest number of different nursing diagnosis labels identified (5-20%).
Concerning their mapping to psychosocial needs, the nursing diagnoses formulated were compared only to the need for emotional security, this group comprising three different nursing diagnosis labels, namely: risk of relocation stress syndrome, anxiety, and Risk for loneliness.
Validation of the nursing diagnosis labels mapped
All the nurses who made up the sample met the inclusion criteria, presenting a score equal or superior to 05 according to established criteria(18). All of the healthcare professionals work and live in Belo Horizonte, Minas Gerais and are female.
It may be verified that the nurse experts involved in this study are qualified for the role, having in addition to practical experience (the minimum length of experience in practice was four years) - experience also in academic and research activities.
For validating the nursing diagnosis labels mapped, one round of the Delphi Technique was used, as the minimum level of agreement established was attained among the evaluators in the first round. It was ascertained that the degree of concordance among the group of nurse experts in the process of validation was 100%. (Kappa= 1.0).
DISCUSSION
Elderly patients currently correspond to 42 52% of admissions to ICU(19). In the sample studied, the majority (68.3%) of the patients were concentrated in the age range of people aged 60 or over, which supports the perception that the average age of patients in ICU has risen in the last few years, and that it will increase still further with the ageing of the population in general.
For the 44 patients whose nursing notes were analyzed, 1087 nursing diagnoses had been formulated, with an average of 8.5 nursing diagnoses being elaborated per patient. This number is close to that described in the literature, in which the average number of diagnoses found per patient was, respectively, 6.9(8) e 8(20).
In this study, only ten of the nursing diagnoses formulated were risk diagnoses, two of which were identified for all of the patients. The 'real' diagnoses describe responses already present in the patients, while the risk diagnoses describe responses that may develop. This last is supported in risk factors which contribute to the increase in vulnerability to pathogens(4). The fact that the majority of diagnoses are classified as 'real' is evidence that nursing care in ICU should be centered on the recuperation of health. However, the identification of risk diagnoses indicates that the nurses are also concerned about preventive aspects of patient care(8). In an ICU one finds patients at risk of death, it falling to the nurse to recognize the initial signs of departure from normality so as to implement quality nursing care.
It may be observed that the nursing diagnoses of risk for constipation, deficit in self-care in bathing/hygiene, and risk for infection, all formulated for 100% of the patients, belong to the following domains established by NANDA-I's taxonomy, elimination and exchange, activity/rest and safety/protection, respectively(4). These diagnoses refer to the BHN of elimination, bodily care and safety (physical and environmental) and they are all psychobiological needs. Some of them may be related to lack of physical activity, as patients hospitalized in ICU remain in bed, and the Risk for constipation may be present.
In these patients the deficit in self-care for bathing/hygiene is evident and had been established for all the patients whose care notes were analyzed. The nursing actions related to bed-baths, intimate hygiene and getting dressed are essential and refer to the human needs of patients who are at complete rest, or whose mobility and locomotion are affected.
In its turn, the nursing diagnosis of Risk for Infection, as mentioned in the present study, has been identified in different hospital units(8,21). This occurrence may be explained by the fact that a hospitalized patient presents increased environmental exposure to pathogens, principally in ICU where a great number of invasive procedures are normally undertaken.
The nursing diagnoses of risk of impaired skin integrity, deficit in self-care for intimate hygiene, Risk for unstable blood glucose level and impaired bed mobility were formulated for over 50% of the patients. Thus, the psychobiological needs of physical integrity, bodily care, vascular regulation and physical activity were affected in these patients.
It may be observed, therefore, that of the diagnoses mapped to the BHN, 25 (89%) are related to psychobiological needs and only 3 (11%) to the psychosocial needs. No nursing diagnoses were mapped to psycho-spiritual needs. Authors have reported that spirituality/religiosity may be considered an extremely relevant need, as it can contribute in inspiring courage, revitalization and confidence in patients on the subject of the process of recuperation from illness(22).
It is understandable that, due to the seriousness of the state of physical health of patients hospitalized in ICU, in providing care, the nursing team prioritizes the documentation of problems and the care given to the psycho-biological needs affected. However, the human needs are inter-related and form part of the indivisible whole of the human being, such that when one need is manifested, all the others suffer some degree of alteration(3). Thus, the priorities for nursing care need to be adjusted systematically.
Although the number of nursing diagnoses mapped to the psycho-social need was limited to three, this is an important piece of data, considering that in the great majority of services carried out by nurses, care remains centered on the doctor-centered model. In a separate study undertaken in an adult ICU, not one nursing diagnosis referent to human psycho-social and/or psycho-spiritual needs was identified(8). The authors question this fact because of knowing that many patients hospitalized in ICU present difficulties related to communication, social isolation, anxiety and spiritual suffering, among others. It seems surprising that these are not documented in the patients' notes, given that they refer to needs which have been affected and which need nursing care.
Analyzing the profiles of the nurses who validated the mapped nursing diagnoses, it was possible to observe that 83% had at least one year's experience of clinical practice in Intensive Care, using a care model which employs the nursing process in practice and which uses nursing diagnoses, interventions and results to document the clinical practice. All are specialists in intensive care, it being worth noting the high number of experts (5-83%) who have been published in the area of intensive care, in nursing diagnosis, interventions or outcomes.
One hundred percent of concordance (Kappa = 1.0) was obtained among the nurse experts who evaluated the nursing diagnoses mapped to the BHNs, in a single round of the Delphi Technique. This may be explained by the fact that the first stage of the cross-mapping was submitted to a process of analysis and confirmation by a group of researchers from the area of the nursing process, which supports the results found in the mapping which was carried out.
CONCLUSION
This study allowed the most frequent nursing diagnoses made in an adult ICU to be identified and mapped to BHN. For the 44 patients whose notes were analyzed, 28 different nursing diagnosis labels were found. Of these, seven were formulated for more than 50% of the patients, with three being formulated for all of the patients. The majority of the nursing diagnoses identified in this study were also found in other research, confirming that they are common to the clinical practice of nurses in ICU.
Only three diagnoses referred to psychosocial needs and none were related to psycho-spiritual needs. This reality shows how important it is that continuity be given to research related to the identification of nursing diagnoses and the BHN that are most frequently affected in the patients hospitalized in ICU. It is suggested that studies be undertaken to identify among the nursing diagnoses formulated and the BHN affected which were resolved, which needs predominate in the care, and which have not been worked on.
In their turn, it is considered that this study's results are important for organizing teaching content for student nurses and the nurses preparing them, so that in providing the care, they consider the entire structure of the human being, covering not only biological aspects, but also cultural, historical and social values, added to the emotional and spiritual aspects which permeate infirm individuals who find themselves hospitalized.
REFERENCES
- 1. Nóbrega MML, Silva KL. Fundamentos do cuidar em enfermagem. 2ª ed. Belo Horizonte: ABEn; 2008/2009.
- 2. Amante LN, Rossetto AP, Schneider DG. Sistematização da Assistência de Enfermagem em unidade de terapia intensiva sustentada pela teoria de Wanda Horta. Rev Esc Enferm USP. 2009;43(1):54-64.
- 3. Horta WA. Processo de enfermagem. São Paulo: EPU; 1979.
-
4North American Nursing Diagnosis Association (NANDA). Diagnósticos de enfermagem da NANDA: definições e classificação 2009-2011. Porto Alegre: Artmed; 2009.
- 5. Nascimento ERP, Trentini M. O cuidado de enfermagem na Unidade de Terapia Intensiva (UTI): teoria humanística de Paterson e Zderad. Rev Latino Am Enferm. 2004;12(2):250-7.
- 6. Carmagnani MI, Cunha IC, Behlau MS. Diagnósticos de enfermagem em pacientes submetidos à laringectomia. Rev Paul Enferm. 2003;22(1):51-61.
- 7. Galdeano LE, Rossi LA, Pezzuto TM. Diagnósticos de enfermagem de pacientes no período pré-operatório de cirurgia cardíaca. Rev Esc Enferm USP. 2004;38(3):307-16.
- 8. Lucena AF, Barros ALBL. Nursing diagnoses in a Brazilian Intensive Care Unit. Int J Nurs Terminol Classif. 2006;17(3):139-46.
- 9. Good PI. Permutation tests: a pratical guide to resampling methods for testing hyphoteses. 2nd ed. New York: Springer-Verlag; 1994. (Springer series in statistics).
- 10. Pavel S, Nolet D. Manual de terminologia. Canadá: Public Words and Govermment Services; 2001.
- 11. Benedet AS, Bub MBC. Manual de diagnóstico de enfermagem: uma abordagem baseada na teoria das necessidades humanas básicas e na classificação diagnóstica da NANDA. 2ª ed. Florianópolis: Bernúncia; 2001.
- 12. Moorhead S, Delaney C. Mapping nursing intervention data into the Nursing Interventions classification (NIC): process and rules. Nurs Diagn. 1997;8(4):137-44.
- 13. Goodman CM. The Delphi Technique: a critique. J Adv Nurs. 1987;12(3):729-34.
- 14. Keeney S, Hasson F, Mckenna H. Consulting the oracle: ten lessons from the Delphi Technique in nursing research. J Adv Nurs. 2006;2(53):205-12.
- 15. Grant JS, Kinney MR. Using the Delphi Technique to examine content validity of nursing diagnosis. Nurs Diag. 1992;3(1):12-22.
-
16Organização Mundial da Saúde (OMS). Classificação Estatística Internacional de Doenças e Problemas Relacionados à Saúde: CID 10. São Paulo: EDUSP; 1998.
-
17North American Nursing Diagnosis Association (NANDA). Diagnósticos de enfermagem da NANDA: definições e classificação 2007-2008. Porto Alegre: Artmed; 2008.
- 18. Fehring RJ. Methods to validate nursing diagnoses. Heart Lung. 1987;16(6): 625-9.
- 19. Alves GC, Silva JGB, Lima RSA, Sobral JB, Mota RMS, Abreu KLS, et al . Fatores de risco para óbito em pacientes idosos gravemente enfermos. Rev Bras Ter Intensiva. 2010;22(2):138-43.
- 20. Pasini D, Alvim I, Kanda L, Mendes RSP, Cruz DALM. Diagnósticos de enfermagem de pacientes em Unidades de Terapia Intensiva. Rev Esc Enferm USP. 1996; 30(3):501-18.
- 21. Rocha LA, Maia TF, Silva LF. Diagnósticos de enfermagem em pacientes submetidos à cirurgia cardíaca. Rev Bras. Enferm. 2006;59(3):321-6.
- 22. Fonseca AS, Tapia GES, Silva IM, Noleto MRP, Campos JP. Espiritualidade: o significado na prática do enfermeiro. Nursing (São Paulo). 2008;11(122):312-7.
Publication Dates
-
Publication in this collection
05 Dec 2012 -
Date of issue
Oct 2012
History
-
Received
22 July 2011 -
Accepted
11 Mar 2012