Abstracts
This cross-sectional study aimed to determine the self-care ability of individuals with type 2 diabetes mellitus and to relate this capacity with some sociodemographic and clinical variables. Participants were 251 patients who attended the Emergency Service at the Mérida Regional Hospital in Yucatán, Mexico, in 2006. Data were obtained through directed home interviews, using a form, a questionnaire and the Self-Care Capacity Scale. Descriptive and correlation statistics were used for data analysis. The results showed 83 (33.5%) subjects with good and 168 (66.5%) subjects with regular ability. A directly proportional correlation was found between self-care ability and years of study (r=0.124; p<0.05), as well as a negative correlation for religion (rs=-0.435; p<0.05) and evolution time of the disease (r=-0.667; p<0.05). These variables should be taken into account to promote self-care for diabetes patients, and further research needs to be developed with a focus on other variables involved in the behavior adopted to benefit their health.
Self care; Diabetes mellitas, type 2; Nursing; Emergency medical services
Estudo transversal com os objetivos de determinar a capacidade de autocuidado de pessoas com diabetes mellitus tipo 2 e relacionar tal capacidade com variáveis sociodemográficas e clínicas. Participaram 251 pessoas que ingressaram no Serviço de Urgência do Hospital Regional Mérida, em Yucatán, México, em 2006. Os dados foram obtidos mediante entrevista domiciliar dirigida, utilizando-se formulário, questionário e a Escala de Capacidade Autocuidado. Para a análise, utilizou-se a estatística descritiva e correlacional. Os resultados mostraram que 83 (33,5%) dos sujeitos apresentaram boa capacidade de autocuidado e 168 (66,5%), capacidade regular. Obteve-se correlação diretamente proporcional entre capacidade de autocuidado e anos de estudo (r=0,124; p<0,05), mas negativa para religião (rs=-0,435; p<0,05) e tempo de evolução da doença (r=-0,667; p<0,05). Para a promoção do autocuidado em pessoas com diabetes faz-se necessário considerar essas variáveis, bem como desenvolver novos estudos que enfoquem outras variáveis envolvidas no comportamento adotado em benefício da saúde.
Autocuidado; Diabetes mellitus tipo 2; Enfermagem; Serviços médicos de emergência
Estudio transversal que tuvo como objetivos determinar la capacidad de autocuidado de personas con diabetes mellitus tipo 2 y relacionar tal capacidad con variables sociodemográficas y clínicas. Participaron 251 personas que ingresaron en el Servicio de Urgencia del Hospital Regional de Mérida, Yucatán, México, en 2006. Los datos fueron obtenidos a través de entrevistas domiciliarias dirigidas, utilizándose formulario, cuestionario y Escala de Capacidad de Auto-cuidado. Para el análisis se utilizó la estadística descriptiva y correlacional. Los resultados mostraron que 83 (33,5%) de los sujetos exhibieron buena capacidad de autocuidado, y 168 (66,5%) capacidad regular. Se obtuvo correlación directamente proporcional entre capacidad de autocuidado y años de estudio (r=0,124; p<0,05) y negativa para religión (r5=-0,435; p<0,05) y tiempo de evolución de la enfermedad (r=-0,667; p<0,05). Para la promoción del autocuidado a la persona con diabetes se deben considerar tales variables, así como desarrollarse nuevos estudios que focalicen otras variables involucradas en el comportamiento adoptado en beneficio de su salud.
Autocuidado; Diabetes mellitus tipo 2; Enfermería; Servicios médicos de urgencia
ORIGINAL ARTICLE
Factors related to self-care in diabetes mellitus patients attended at na emergency service in Mexico*
Factores relacionados al autocuidado de personas con diabetes mellitus atendidas en servicio de urgencia en México
Irasema Romero BaquedanoI; Manoel Antônio dos SantosII; Carla Regina de Souza TeixeiraIII; Tatiane Aparecida MartinsIV; Maria Lúcia ZanettiV
IRN. PhD in Fundamental Nursing, University of São Paulo at Ribeirão Preto, College of Nursing. Collaborating Center for Nursing Research Development. Ribeirão Preto, SP, Brazil. irasemaromero@hotmail.comIIPsychologist. Professor at the University of São Paulo at Ribeirão Preto, Faculty of Philosophy, Sciences and Letters. Ribeirão Preto, SP, Brazil. masantos@ffclrp.usp.brIIIRN. Professor at the University of São Paulo at Ribeirão Preto. Ribeirão Preto, SP, Brazil. carlarst@eerp.usp.br
IVUndergraduate student, University of São Paulo at Ribeirão Preto. Ribeirão Preto, Teaching Diploma in Nursing. Ribeirão Preto, SP, Brazil. tatianemartins@hotmail.comVRN. Associate professor, University of São Paulo at Ribeirão Preto. Ribeirão Preto, SP, Brazil. zanetti@eerp.usp.br
Correspondence addressed to
ABSTRACT
This cross-sectional study aimed to determine the self-care ability of individuals with type 2 diabetes mellitus and to relate this capacity with some sociodemographic and clinical variables. Participants were 251 patients who attended the Emergency Service at the Mérida Regional Hospital in Yucatán, Mexico, in 2006. Data were obtained through directed home interviews, using a form, a questionnaire and the Self-Care Capacity Scale. Descriptive and correlation statistics were used for data analysis. The results showed 83 (33.5%) subjects with good and 168 (66.5%) subjects with regular ability. A directly proportional correlation was found between self-care ability and years of study (r=0.124; p<0.05), as well as a negative correlation for religion (rs=-0.435; p<0.05) and evolution time of the disease (r=-0.667; p<0.05). These variables should be taken into account to promote self-care for diabetes patients, and further research needs to be developed with a focus on other variables involved in the behavior adopted to benefit their health.
Key words: Self care. Diabetes mellitas, type 2. Nursing. Emergency medical services.
RESUMEN
Estudio transversal que tuvo como objetivos determinar la capacidad de autocuidado de personas con diabetes mellitus tipo 2 y relacionar tal capacidad con variables socio-demográficas y clínicas. Participaron 251 personas que ingresaron en el Servicio de Urgencia del Hospital Regional de Mérida, Yucatán, México, en 2006. Los datos fueron obtenidos a través de entrevistas domiciliarias dirigidas, utilizándose formulario, cuestionario y Escala de Capacidad de Auto-cuidado. Para el análisis se utilizó la estadística descriptiva y correlacional. Los resultados mostraron que 83 (33,5%) de los sujetos exhibieron buena capacidad de autocuidado, y 168 (66,5%) capacidad regular. Se obtuvo correlación directamente proporcional entre capacidad de autocuidado y años de estudio (r=0,124; p<0,05) y negativa para religión (r5=-0,435; p<0,05) y tiempo de evolución de la enfermedad (r=-0,667; p<0,05). Para la promoción del autocuidado a la persona con diabetes se deben considerar tales variables, así como desarrollarse nuevos estudios que focalicen otras variables involucradas en el comportamiento adoptado en beneficio de su salud.
Descriptores: Autocuidado. Diabetes mellitus tipo 2. Enfermería. Servicios médicos de urgencia.
INTRODUCTION
There are different definitions of self-care in specific cultural and social contexts(1). In the Americas, self-care refers to actions people adopt in favor of their own health without formal medical supervision. It is defined as practices carried out by people and family members through which positive health behaviors are promoted to prevent diseases and treat symptoms(1).
Historically, nursing is a discipline that seeks to educate people in self-care(1). Self-care is defined as a regulating function, which individuals deliberately use to maintain vital requirements, for development and integral functioning(2). The ability to perform self-care is developed over life through a spontaneous learning process, given the maturation of intellectual curiosity, with others' guidance and supervision and experience with self-care measures(3).
Self-care is also considered part of people's life style, which is understood as a standard of conduct that reflects on the way individuals interact in the social milieu(3). The concept of lifestyle is broad and involves standards that emerge from the selection of options available to people according to their social and economic circumstances, and the facility with which they choose alternatives. Hence, the choice of a healthy lifestyle implies concrete self-care actions such as self-medication, self-treatment, social support and care taken in situations of disease in the individual's environment(3).
The World Health Organization recommends promoting self-care education to prevent and treat chronic diseases(1). Self-care education for people with chronic health problems should promote the development of self-care skills so that individuals share and assume responsibility for their own health and learn to live better with the disease, modify or keep healthy habits, and promote self-reliance so they feel better regardless of the severity of the disease.
Self-care is an efficacious strategy to reduce the cost of health care, reduce the number of hospitalizations and emergency consultations, promote the rational use of medication and improve the relationship between health professionals and patients(1). In this context, self-care in health is defined as measures each person individually takes to protect his/her physical, mental and social well-being. Self-care is based on the belief that human beings are capable of caring for their health and includes a series of actions to maintain physical and mental health, prevent diseases, satisfy physical and psychological needs, seek medical help or to self-medicate(1).
When one considers that individuals with diabetes mellitus present a chronic condition that requires permanent care to maintain quality of life and metabolic control, one perceives the need to develop self-care skills to manage the disease. One study showed that introducing lifestyle changes is an effective strategy in preventing type 2 diabetes mellitus(4).
The role of multiprofessional health teams is to help individuals with diabetes to develop self-care skills to manage the disease to keep appropriate metabolic control, prevent or delay diabetes-related chronic complications(5). The presence of a professional is particularly important when a person has difficulty taking responsibility for her/his self-care.
From this perspective, professionals need to know the variables related to self-care to provide effective care. Studies have addressed these issues, investigating variables related to access to information and knowledge, satisfaction with health services, family support, among other relevant psychosocial factors(5-9).
Therefore, this study focuses on variables related to the self-care ability of people cared for in an emergency service of a general hospital to support the restructuring process of care provided to the population with diabetes in Mexico in the context of the Integrated Health Care Model (MIDAS)(10). Identifying the variables related to self-care allows the identification of potential barriers for treatment adherence of people with type 2 diabetes mellitus and also the proposal of educational strategies to strengthen self-care in the studied population.
OBJECTIVES
This study aims to determine the self-care ability of people with type 2 diabetes mellitus and relate this ability to gender, age, schooling, religion, type of disease evolution, and participation in support groups.
METHOD
This cross-sectional study was carried out in the emergency service of the Regional Hospital Mérida, Institute of Social Welfare and Services for State Workers (ISSSTE), Mérida, Yucatán, Mexico, from January 1st to December 31st 2006.
A convenience sample was used. Inclusion criteria were: people with diagnosis of type 2 diabetes mellitus, both genders, age between 30 and 80 years of age, residents of Mérida, Mexico, who were cared for by the emergency service of the previously mentioned hospital during the 12-month period defined by the study and voluntarily consented to participate in the study. Exclusion criteria were: people with type 2 diabetes mellitus who, after three consecutive visits, were not found at their households, moved to another address or died in the study period.
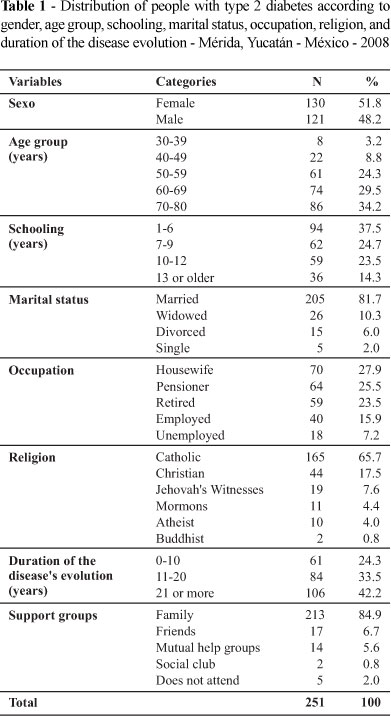
Of the 382 people with type 2 diabetes admitted into the service, 131 did not meet the inclusion criteria. The sample was composed of 251 people with type 2 diabetes mellitus who met the eligibility criteria. Table 1 shows the characterization of the individuals' socio-demographic variables.
Data Collection Instrument
The following were used to collect data: one registration form, one questionnaire with socio-demographic and clinical variables, and one scale to measure self-care ability. The registration form was used to obtain a list of patients' hospitalization date, name, medical file number, address and hospitalization motive.
The questionnaire included six closed questions addressing socio-demographic and clinical variables: gender, age, schooling, marital status, occupation, religion, duration of the disease evolution and participation in support groups. The Self-Care Ability Scale is an instrument developed and validated in Mexico(11). It is a Likert scale with 25 items that evaluate universal self-care requirements, of development and diversion of health, with a satisfactory level of reliability (Crombach's alpha = 0.86). To evaluate self-care ability, a three-point score was attributed to the items always, two to frequently, one to sometimes, and zero to never. At the end, scores obtained in all the items were computed, which was compared with the proposed indicators: very good (57-75), good (38-56), regular (19-37), poor (0-18). The maximum possible score is 75 points.
Procedure
First, the patients' medical files were found and data concerning date of hospitalization, , patients' name and file number, address and motive of hospitalization were recorded in the form. With the respective addresses, patients and family members were visited at home for the purpose of clarification concerning the study's objectives. If they consented to participate in the study, a free and informed consent form was signed.
Then, socio-demographic and clinical data were obtained through the individual application of the questionnaire. Data collection was completed with the Self-Care Ability Scale. The application of the instruments took an average of 30 minutes and was held at the participants' home in a private room.
To organize and analyze data, the statistical program SPSS version 12.0 was used. For the correlative descriptive statistics Pearson's r was used to establish the relationship between proportion or interval variables and Spearman's correlation for the ordinal variables with the level of significance at p<0.05.
The study was approved by the Committee on Bioethics, College of Nursing and Obstetrics at Celaya, Mexico, on November 5th 2007.
RESULTS
When self-care abilities of people with type 2 diabetes were analyzed, the minimum score 25 and the maximum 43 were found, average of 35.72±3.69.
According to the proposal of the Self-Care Ability Scale, the answers were grouped and categorized as: very good, good, regular and poor. The data obtained in relation to self-care ability showed that 83 (33.5%) people with type 2 diabetes presented good self-care ability and 168 (66.5%) regular ability.
In relation to self-care ability related to gender (Table 2), we observed that 47 (18.7%) women presented good self-care ability and 83 (33.1%) regular. In relation to men, 37 (14.7%) presented good self-care ability and 84 (33.5%) regular.
Concerning self-care ability in relation to age group (Table 3) the following groups presented good self-care ability: 26 (10.3%) individuals between 70 and 80 years of age, 25 (10.0%) between 50 and 59 years of age, 22 (8.8%) between 60 and 69 years of age, 10 (4.0%) between 40 and 49 years of age, and one (0.4%) between 30 and 39 years of age.
In relation to regular self-care ability: 60 (23.9%) individuals between 70 and 80 years old, 52 (20.7%) between 60 and 69 years of age, 36 (14.3%) between 50 and 59 years of age, 12 (4.8%) between 40 and 49, and seven (2.8%) individuals between 30 and 39 years of age displayed regular self-care ability (Table 3).
In relation to self-care ability related to schooling (Table 4), of the 94 (37.5%) individuals who completed one to six years of schooling (primary school in Mexico): 29 (11.5%) had good self-care ability and 65 (26.0%) had regular self-care ability. Of the 62 (24.7%) individuals who completed from seven to nine years of schooling (secondary school): 17 (6.8%) had good ability to self-care and 45 (17.9%) regular ability. Of the 59 (23.5%) people who completed from 10 to 12 years of schooling: 22 (8.8%) showed good self-care ability and 37 (14.7%) regular ability. Of the 36 (14.3%) people who had a bachelor's degree (13 or more years of schooling), 16 (6.4%) had good self-care ability and 20 (7.9%) had regular self-care ability.
Considering self-care ability related to religion, of the 84 (33.5%) people who presented good self-care ability: 80 (31.9%) were Catholic, three (1.2%) were Christians, and one (0.4%) was Mormon. Of the 167 (66.5%) individuals with regular self-care ability: 85 (33.8%) were Catholic, 41(16.3%) Christians, 19 (7.6%) Jehovah witnesses, 10 (4.0%) were Mormons, two (0.8%) were Buddhists, and 10 (4.0%) were atheists.
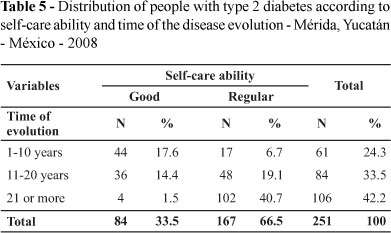
In regard to self-care ability related to duration of disease evolution (Table 5), of the 84 (33.5%) individuals who presented good self-care ability: 44 (17.6%) had the disease from one to 10 years, 36 (14.4%) from 11 to 20 years, and four (1.5%) 21 years or more. Of the 167 (66.5%) individuals who presented regular self-care ability: 17 (6.7%) had the disease from one to 10 years, 48 (19.1%) from 11 to 20 years, and 102 (40.7%) for 21 year of more.
When analyzing the correlation between self-care ability and years of schooling (r=0.124; p<0.05), a directly proportional correlation was found between these two variables, that is, the higher the schooling level, the higher the individuals' self-care ability.
Considering the correlation between self-care and religion, a negative correlation was found (rs=-0.435; p<0.05), that is, the lower the belief expressed in religion, the higher the self-care ability.
Finally, an inversely proportional correlation was found between the evolution of the disease and self-care ability, the shorter the duration of the evolution of the disease, the higher the individuals' self-care ability (r=-0.667; p<0.05).
DISCUSSION
Currently, there are recommendations to develop self-care abilities among people with diabetes to control the disease(12). For that, individuals with diabetes mellitus need to actively participate in the monitoring of the disease: food choice, numbers of meals, quality and quantity of food, regular physical exercise, self-monitoring of capillary glucose, feet examination, use of correct medication doses and schedule, periodical medical consultations, knowledge of signs and symptoms of hyperglycemia, among others.
The average score obtained when analyzing the self-care ability of people with type 2 diabetes mellitus was 35.72±3.69 points. A total of 33% of the individuals presented good self-care ability and 67% regular self-care ability in the Self-Care Ability Scale. None presented very good or poor self-care ability.
When considering the score obtained by the individuals in this study in relation to self-care ability, one needs to take into account the individuals' average age, older than 65 years. People who are at this stage of development have self-care requirements related to the phase of the life cycle itself and also co-morbidities and chronic complications that accrue from poor metabolic control, which might explain the results of the study(13).
The data lead to the reflection that the studied people with type 2 diabetes mellitus might have low motivation for self-care and/or limitations given impairment related to co-morbidities and chronic conditions. From this perspective, the literature indicates that when a person with diabetes presents some impairment and/or limitation, the presence of a professional is essential to motivate and help the individual to develop self-care abilities(9).
Diabetes mellitus is considered a highly complex disease and most people with type 2 diabetes are diagnosed in the adult phase, which imposes a challenge to health educators to ensure effective interventions that really favor the incorporation of self-care in the disease management given the peculiarities of the learning process of adult individuals .
On the other hand, considering that only 5.6% of the studied individuals participated in Mutual Help Groups, we can infer that they did not have the opportunity to develop abilities to self-care. These data refer to the analysis that public policies adopted in Mexico in health care delivered to people with diabetes mellitus still need adjustments to obtain effective results.
The diagnosis of a chronic disease such as type 2 diabetes mellitus implies adopting self-care behavior for the entire life, including changes in lifestyle compatible with their own concept of quality of life. Given these circumstances, abandoning part or the entire prescribed treatment is not uncommon(14). Because this is a disease that requires permanent care, adherence to treatment might be low, resulting in poor metabolic control. A study revealed that only a fraction of people with type 2 diabetes regularly realizes follow-up in health institutions and only 25% to 40% achieved the desired metabolic control(10).
Knowledge concerning self-care abilities is another variable that can explain the score obtained by the studied individuals. One study addressing the importance of having knowledge about self-care in diabetes mellitus showed that a low level of information about the disease and its etiology hinder the learning process, harms prevention and early diagnosis and increases the probability of other complications(6).
In relation to self-care ability according to age, one has to consider that age is an important factor in the perception of environmental barriers for treatment adherence. The older the individual, the higher his/her perception of environmental barriers(15). On the other hand, the youngest people are those who least perceive environmental barriers(15).
The absolute increase of the Mexican population is in itself a challenge for the health system. The change in the age pyramid shows that the Mexican population is aging. The health problems of the adult population, between 45 and 64 years of age and the older population show that the demand is growing with repercussions on the economic and organizational spheres(10). The country is going through a demographic and epidemiological transition. Health professionals need to rethink effective strategies to care for older individuals, considering the specificities in this phase of the life cycle(10).
Age is a factor that interferes in health needs during life cycle development. An adult individual has values, beliefs and habits already formed when s/he receives the diagnosis of type 2 diabetes mellitus. The onset of diabetes at this stage of life might be accompanied by resistance to change, which might explain, in part, data obtained in this study(2). Hence, age is a variable that is important to be taken into account when evaluating self-care ability and when providing education in diabetes for managing the disease. Consequently, it is a relevant variable that can influence treatment-adherence.
Another aspect to consider is the proportion of Mexican individuals who develop type 2 diabetes before 40 years of age(16). Considering that these individuals are exposed to the effects of hyperglycemia for a prolonged period of time and are thereby at a higher risk to develop chronic diseases, the impact of such diseases on the Mexican Health System might become unsustainable. It is necessary that Mexican policies guiding care directed to individuals with diabetes be urgently consolidated.
In relation to self-care ability according to years of schooling, individuals with higher levels of schooling showed good self-care ability; the higher the years of schooling the better the individuals' self-care abilities. Hence, people who received more years of formal education tend to present more knowledge and ability for self-care and also better ability to relate with the health team(5). Given the disease's complexity, schooling years is a variable that should be considered in planning educational programs for diabetes designed to develop self-care abilities. From this perspective, health professionals should consider this variable and seek diversified and innovative teaching strategies capable of mobilizing people with diabetes to self-care.
The analysis of self-care in relation to religious beliefs should account for the fact that people might place the responsibility for self-care on a superior being. When a person attributes the responsibility of his/her care to a religious belief, s/he may not value the acquisition of knowledge, skills and motivation to self-care. Hence, the development of self-care abilities becomes limited, since it is considered an issue exogenous to the individual. In this case, health professionals should seek strategies designed to enable individuals to assume the responsibility for their own self-care(17).
Because type 2 diabetes mellitus is a chronic disease, it demands patients maintain self-care behavior for their entire lives(18). This condition is one of the factors that determine treatment-adherence. When the self-care ability is undermined, one of the consequences might be unsatisfactory metabolic control. One study showed that only a small portion of people with diabetes regularly seeks health services and only 25% to 40% of them have satisfactory metabolic control(19).
CONCLUSION
The results obtained in this study allowed determining that most of people with type 2 diabetes mellitus presented regular self-care ability (66.5%), and this is related to socio-demographic and clinical variables.
Self-care ability related to gender indicated that the studied women had better self-care abilities compared to men. Better self-care abilities were also found among individuals between 70 and 80 years of age. Individuals with six years of schooling presented better self-care abilities as did those who reported being Catholic. In relation to duration of disease, the results indicated that the longer a person has diabetes, the worse is her/his self-care ability.
These findings indicate that the self-care ability of people with type 2 diabetes mellitus is linked to multiple factors that deserve attention of health professions when proposing education programs.
The scarcity of national studies to compare results limits the understanding of the implications of the obtained results for the Mexican context. Further studies addressing other variables that might be related to self-care abilities are needed to enable future comparisons and fill in this gap.
REFERENCES
-
1Organización Panamericana de Salud. Fortalecimiento del autocuidado como estrategia de la Atención Primaria en Salud: la contribución de las instituciones de salud en América Latina [texto en la Internet]. Santiago, Chile; 2006. [citado 2008 out. 17]. Disponible en: http://www.biblioteca.cotecnova.edu.co/docentes/Magali/Cartillas/autocuidado.pdf
- 2. Orem DE. Nursing: concepts of practice. 6th ed. St Louis: Mosby; 2001.
- 3. Kickbusch I. Self-care in health promotion. Soc Scienc Med. 1989;29(2):125-30.
- 4. Tuomilehto J, Lindström J, Eriksson JG, Valle TT, Hämäläinen H, Ilanne-Parikka P, et al. Finnish Diabetes Prevention Study Group. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. 2001;344(18):1343-50.
- 5. Otero LM, Zanetti ML, Souza CRT. Sociodemographic and clinical characteristics of a diabetic population at a primary level health care center. Rev Lat Am Enferm. 2007; 15(n.esp):768-73.
- 6. Pace AE, Ochoa-Vigo K, Caliri MHL, Fernandes APM. O conhecimento sobre diabetes mellitus no processo de autocuidado. Rev Lat Am Enferm. 2006;14(5):728-34.
- 7. Otero LM, Zanetti ML, Ogrizio MD. Knowledge of diabetic patients about their disease before and after implementing a diabetes education program. Rev Lat Am Enferm. 2008;16(2):231-7.
- 8. Zanetti ML, Otero LM, Biaggi MV, Santos MA, Péres DS, Guimarães FPM. Satisfaction of diabetes patients under follow-up in a diabetes education program. Rev Lat Am Enferm. 2007;15(4):583-9.
- 9. Péres DS, Santos MA, Zanetti ML, Ferronato AA. Dificuldades dos pacientes diabéticos para o controle da doença: sentimentos e comportamentos. Rev Lat Am Enferm. 2007;15(6):1105-12.
-
10México. Secretaría de Salud. Programa Nacional de Salud 2001-2006. La democratización de la salud en México. Hacia un sistema universal de salud [texto en la Internet]. México (DF); 2001. [citado 2008 out. 17]. Disponible en: http://www.scielosp.org/scieloOrg/php/reflinks.php?refpid=S0036-3634200700070 000700011&pid=S0036-36342007000700007&lng=en
- 11. Díaz GR, Jordán JML, Vera RAM, Ruiz PL, Olalde GE. Escala de Capacidad de Autocuidado. Guanajuato (MEX): Facultad de Enfermería y Obstetricia de Celaya, Universidad de Guanajuato; 2004.
- 12. Sociedade Brasileira de Diabetes (SBD). Diretrizes SBD 2007: tratamento e acompanhamento do diabetes mellitus. São Paulo; 2007.
- 13. Zanetti ML, Biaggi MV, Santos MA, Peres DS, Teixeira CRS. O cuidado à pessoa diabética e as repercussões na família. Rev Bras Enferm. 2008;61(2):186-92.
- 14. Leite SN, Vasconcellos MPC. Adesão à terapêutica medicamentosa: elementos para a discussão de conceitos e pressupostos adotados na literatura. Ciênc Saúde Coletiva. 2003;8(3):775-82.
- 15. Martinez AO, Moreno MMG. Barreras ambientales para el apego al tratamiento en pacientes con diabetes tipo 2. Desarro Cient Enferm. 2006;14(6):196-201.
- 16. México. Secretaría de Salud. Programa de Acción: diabetes mellitus. México (DF): Secretaría de Salud; 2001.
- 17. Tavares DMS, Rodrigues RAP. Educação conscientizadora do idoso diabético: uma proposta de intervenção do enfermeiro. Rev Esc Enferm USP. 2002;36(1):88-96.
- 18. Souza CR, Zanetti ML. Administração de insulina: uma abordagem fundamental na educação em diabetes. Rev Esc Enferm USP. 2000;34(3):264-70.
- 19. Clement S. Diabetes self-management education. Diabetes Care. 1995;18(8):1204-14.
Publication Dates
-
Publication in this collection
15 Dec 2010 -
Date of issue
Dec 2010
History
-
Received
05 Aug 2009 -
Accepted
10 Mar 2010