
ABSTRACT
Objective
To understand the experience of men in relation to the process of living with hemophilia.
Method
Qualitative study using the theoretical and methodological referential Symbolic Interactionism and the constructivist strand of Grounded Theory. Participated 12 men with hemophilia followed at a Blood Center in the south of Rio Grande do Sul, Brazil. Intensive interviews, genograms and field notes were used for data collection, with concomitant analysis, following the initial, focused, and theoretical coding stages.
Results
The theoretical model was built, which has as central category Adapting to (co)exist with hemophilia and the categories Knowing yourself and the illness: knowing how to deal, Adjusting life: taking care of yourself and Getting used to the illness: being almost normal.
Conclusion
It was revealed the experience of men who adapt to (co)exist with hemophilia and their actions and behaviors, aiming to preserve them away from bleeding, pain, and the risk of death.
Keywords
Hemophilia A; Hemophilia B; Life change events; Qualitative research; Nursing
RESUMEN
Objetivo
Comprender la experiencia de los hombres en relación con el proceso de vivir con hemofilia.
Método
Estudio cualitativo usando los referenciales teórico y metodológico Interaccionismo Simbólico y la línea constructivista de la Teoría Fundamentada. Participaran 12 hombres con hemofilia acompañados en un Banco de Sangre en el sur del Rio Grande do Sul, Brasil. Se utilizó para recolecta de datos entrevista intensiva, genograma y nota de campo, con análisis concomitante, siguiendo las etapas de codificación inicial, focalizada y teórica.
Resultados
Se construyó el modelo teórico, que tiene como categoría central Adaptando para (con)vivir con hemofilia y las categorías Conociendo a sí mismo y la enfermedad: sabiendo lidiar, Ayustando la vida: cuidando de sí y Acostumbrándose con la enfermedad: siendo casi normal.
Conclusión:
Se reveló la experiencia de hombres que se adaptan a (con)vivir con hemofilia y sus acciones y comportamientos, con el objetivo de preservarlos lejos del sangrado, el dolor y el riesgo de muerte.
Palabras clave
Hemofilia A; Hemofilia B; Acontecimientos que cambian la vida; Investigación cualitativa; Enfermería
RESUMO
Objetivo
Compreender a experiência de homens em relação ao processo de viver com a hemofilia.
Método
Estudo qualitativo usando os referenciais teórico e metodológico Interacionismo Simbólico e a vertente construtivista da Teoria Fundamentada nos Dados. Participaram 12 homens com hemofilia acompanhados em um Hemocentro situado no sul do Rio Grande do Sul, Brasil. Utilizou-se para a coleta de dados entrevista intensiva, genograma e nota de campo, com análise concomitante, seguindo as etapas de codificação inicial, focalizada e teórica.
Resultados
Construiu-se o modelo teórico, que tem como categoria central Adaptando para (con)viver com a hemofilia e as categorias Conhecendo a si e a doença: sabendo lidar, Ajustando a vida: cuidando de si e Acostumando-se com a doença: sendo quase normal.
Conclusão
Revelou-se a experiência de homens que realizam adaptações para (con)viver com a hemofilia e suas ações e comportamentos, visando preservá-los longe de sangramentos, da dor e do risco de morte.
Palavras-chave
Hemofilia A; Hemofilia B; Acontecimentos que mudam a vida; Pesquisa qualitativa; Enfermagem
INTRODUCTION
Hemophilia is a genetic, hemorrhagic illness, of recessive inheritance linked to gender, resulting from mutations in the genes that encode coagulation factors VIII (hemophilia A) or IX (hemophilia B), located in the long arm of the X chromosome11. Castellone DD, Adcock DM. Factor VIII activity and inhibitor assays in the diagnosis and treatment of hemophilia A. Semin Thromb Hemost. 2017;43(3):320-30. doi: https://doi.org/10.1055/s-0036-1581127
https://doi.org/10.1055/s-0036-1581127...
-22. Sokołowska B, Kozińska J, Kozioł M, Wąsik-Szczepanek E, Szczepanek D, Hus M. Diagnosis and treatment of acquired hemophilia: a single-center experience. Pol Arch Intern Med. 2017;127(11):796-9. doi: https://doi.org/10.20452/pamw.4139
https://doi.org/10.20452/pamw.4139...
. The prevalence of hemophilia A and B is around 1:5,000 to 10,000 (about 80% of cases) and 1:30,000 to 40,000 (about 20% of cases) male births. In majority is transmitted by the child’s carrier mother, but almost 30% of the cases come from a new mutation. This phenomenon occurs in the mother or in the fetus, and it may be a single isolated case or only between siblings, with no previous manifestation in other family members22. Sokołowska B, Kozińska J, Kozioł M, Wąsik-Szczepanek E, Szczepanek D, Hus M. Diagnosis and treatment of acquired hemophilia: a single-center experience. Pol Arch Intern Med. 2017;127(11):796-9. doi: https://doi.org/10.20452/pamw.4139
https://doi.org/10.20452/pamw.4139...
. In the Report on the Annual Global Survey 2018, carried out by the World Federation of Hemophilia, 210,454 people with hemophilia were identified worldwide, and from these, 12,653 in Brazil. 125 countries participated in the research, reaching 6,990,954,264 of the world population33. Soucie JM. Global hemophilia care: data for action. Ann Intern Med. 2019;171(8):585-6. doi: https://doi.org/10.7326/M19-2535
https://doi.org/10.7326/M19-2535...
.
The hemorrhagic manifestations occur especially in the form of muscle hematomas (10-20%) and hemarthrosis (70-80%), which most frequently affect the knee, ankle, elbow, shoulder and hip joints. When they reach the same joint repeatedly, in the long term, they can progress to hemophilic arthropathy, causing motor sequelae, contractures and physical disability. It is an incurable illness and the treatment consists by the intravenous infusion of the deficient factor concentrate or with its abnormal coagulant activity11. Castellone DD, Adcock DM. Factor VIII activity and inhibitor assays in the diagnosis and treatment of hemophilia A. Semin Thromb Hemost. 2017;43(3):320-30. doi: https://doi.org/10.1055/s-0036-1581127
https://doi.org/10.1055/s-0036-1581127...
-22. Sokołowska B, Kozińska J, Kozioł M, Wąsik-Szczepanek E, Szczepanek D, Hus M. Diagnosis and treatment of acquired hemophilia: a single-center experience. Pol Arch Intern Med. 2017;127(11):796-9. doi: https://doi.org/10.20452/pamw.4139
https://doi.org/10.20452/pamw.4139...
.
As it is a chronic condition, people live for a long time, showing periods of improvement or worsening, in addition, it causes suffering and can generate disabilities44. Martin A, Mulhern B, Shaikh A, Asghar S, O'Hara J, Pedra G, et al. Disease state adaptation experienced by patients with hemophilia: literature review and expert consensus. Blood. 2019;134(Suppl 1):5801. doi: https://doi.org/10.1182/blood-2019-124396
https://doi.org/10.1182/blood-2019-12439...
-55. Gupta N, Benbouzid A, Belhani M, El Andaloussi M, Maani K, Wali Y, et al. HAEMOcare: the first international epidemiological study measuring burden of hemophilia in developing countries. TH Open. 2019;3(2):e190-9. doi: https://doi.org/10.1055/s-0039-1688414
https://doi.org/10.1055/s-0039-1688414...
. The man with hemophilia, although being careful, is exposed to the risk of bleeding, and consequently, pain and physical sequelae, which causes stress66. Thomazelli CF, Lemos JM, Marques CLBB. Percepção dos portadores de hemofilia sobre a atuação do enfermeiro. Saúde Biociênc. 2019 [cited 2020 Mar 25];1(1):18-33. Available from: http://unifatea.com.br/seer3/index.php/saudebiociencias/article/view/1096/1011
http://unifatea.com.br/seer3/index.php/s...
. Situations that can influence your lifestyle and quality of life, requiring adaptations at all times.
Therefore, he needs permanent care at the biopsychosocial and spiritual level, both for himself and for other people with whom he has relationships. Thus, it is believed that the support and involvement between man, family and multidisciplinary team are fundamental for the success of prophylactic and therapeutic measures and the full reaching of well-being. In addition, listening to these men and understanding their way of acting in the world, with the illness and the treatment, can assist to a comprehensive and quality care conduct, resulting in effective care practices.
In this context, this study is relevant due to the need to understand the experience of men with hemophilia, since in the literature, in general, the approach is centered on clinical aspects22. Sokołowska B, Kozińska J, Kozioł M, Wąsik-Szczepanek E, Szczepanek D, Hus M. Diagnosis and treatment of acquired hemophilia: a single-center experience. Pol Arch Intern Med. 2017;127(11):796-9. doi: https://doi.org/10.20452/pamw.4139
https://doi.org/10.20452/pamw.4139...
,55. Gupta N, Benbouzid A, Belhani M, El Andaloussi M, Maani K, Wali Y, et al. HAEMOcare: the first international epidemiological study measuring burden of hemophilia in developing countries. TH Open. 2019;3(2):e190-9. doi: https://doi.org/10.1055/s-0039-1688414
https://doi.org/10.1055/s-0039-1688414...
and, thus, the exiguous focus is verified in the subjective aspects that are part of daily life and positively or negatively influence life, both with regard to the male gender, as well as this and hemophilia. Still, for contributing with reflections and information about the experience of man in living with hemophilia, giving him a voice and visibility as the protagonist of his care in society, as well as contributing to the practice of Nursing. Especially in hemophilia, in which the adaptation process is intrinsic to man’s life, influencing his actions. Thus, the objective is to understand the experience of men in relation to the process of living with hemophilia.
METHOD
Qualitative study that used the theoretical perspective of Symbolic Interactionism77. Blumer H. Symbolic interactionism: perspective and method. Englewood Cliffs: Prentice-Hall; 1969.-88. Charon JM. Symbolic interactionism: an introduction, an interpretation, an integration. 10th ed. Boston: Prentice Hall; 2010. for making possible to apprehend the meanings attributed by the human being to the social objects with which he interacts and his actions in the different circumstances of life, allowing to understand the experience of men with hemophilia. The methodological reference used was the constructivist strand of Grounded Theory (GT)99. Charmaz K. A construção da teoria fundamentada: guia prático para análise qualitativa. Porto Alegre: Artmed; 2009. -1010. Yin RK. Pesquisa qualitativa do início ao fim. Porto Alegre: Penso; 2016., based on Symbolic Interactionism and with a view to seize the person's experience to develop a theory, which is structured with the collection and systematic analysis of qualitative data.
The study was carried out with 12 men with hemophilia followed at the Regional Blood Center of Pelotas (Hemocentro Regional de Pelotas - HEMOPEL), Rio Grande do Sul, Brazil, with data collection and analysis from June 2014 to November 2015. The number of participants was not predetermined, since the GT considers the theoretical sampling, which was formed by the representativeness and density of the data that occurred during the collection and analysis, carried out simultaneously. Therefore, data collection was interrupted with the achievement of theoretical saturation, that is, when there was verified repetition of data and the absence of new information and, in parallel, there was an understanding of the identified concepts99. Charmaz K. A construção da teoria fundamentada: guia prático para análise qualitativa. Porto Alegre: Artmed; 2009. .
Participants met the inclusion criteria: being male, having hemophilia A or B, being 18 years old or more and being a monitored user at HEMOPEL; and exclusion criteria: presenting cognitive limitations, such as speech, attention and/or reasoning, and not speaking the Portuguese language. First, they were divided into sample groups, composed as follows: first group, they had siblings with the illness; second group, they did not have siblings with the illness, but other family members, such as grandfather, uncle, cousin, nephew and grandson; and third group, only they had the illness in the family. Next, a list was organized, respecting the composition of each sample group, in alphabetical order, with name and phone number and family members affected by the illness, information collected from the users’ medical records.
The first nine men were interviewed according to the division of the sample groups, five belonging to the first, two to the second and two to the third. The last three men interviewed fit into the second sample group, however, with the need to gather relevant data in order to elaborate and refine the categories, more data was collected. It was sought men with characteristics that corroborated the reach of densification of existing categories with theoretical saturation, that is, one man with difficulties in dealing with the illness and the treatment and two with complications due to hemophilia due to problems with diagnosis and treatment, and who had experienced the illness for approximately 40 years.
The initial approach to the participants took place in person or by telephone, by searching for the researcher or after contact by the men themselves with the researcher. Subsequently, seven chose to do the interview at HEMOPEL, because they had to go to the service to undergo physical therapy, to seek coagulation factor and to consult, and the others preferred it at home. The researcher conducted interviews in the municipalities of Pelotas, Rio Grande and Canguçu.
Data collection was carried out using the following research instruments: intensive interview99. Charmaz K. A construção da teoria fundamentada: guia prático para análise qualitativa. Porto Alegre: Artmed; 2009. , which with the participants’ consent was recorded and transcribed in full; genogram construction1111. Wright LM, Leahey M. Enfermeiras e famílias: um guia para avaliação e intervenção na família. 5. ed. São Paulo: Roca; 2012. ; and field notes99. Charmaz K. A construção da teoria fundamentada: guia prático para análise qualitativa. Porto Alegre: Artmed; 2009. .
To carry out the interview and the genogram construction, a meeting was held with the first nine men and two with the last three, which lasted from 1 hour to 4 hours and 55 minutes. To understand the experience of men living with hemophilia, questions were asked like: Tell me what it is like to live with hemophilia; Speak what hemophilia is to you; Comment on what it means to have hemophilia for you; Tell me how your life with this illness has been for you; Tell me what you think about your future.
Regarding the data analysis, this was concomitant with the collection, using the constant comparative method, following the stages for the construction of the GT. In the initial coding, there was a rigorous fixation on the data, looking for the actions contained in each part of the reports, being analyzed line by line for the extraction of the first codes. In the focused coding, the identified codes were grouped to form the categories, which were built and rebuilt, and compared among themselves. And in the theoretical coding, it was sought to identify the central category that integrates the others, determined its connection with the other categories and between them. It is noteworthy that during the entire data collection and analysis process, occurred with written memos, which helped to keep the researcher involved in the investigation process. In addition, it enabled writing free of thoughts, observations and impressions, as well as providing reflections and the formation of categories and the theorization99. Charmaz K. A construção da teoria fundamentada: guia prático para análise qualitativa. Porto Alegre: Artmed; 2009. .
Furthermore, it is worth noting that the theoretical model was validated with the participants, briefly telling the story of their experience and they recognizing themselves in it99. Charmaz K. A construção da teoria fundamentada: guia prático para análise qualitativa. Porto Alegre: Artmed; 2009. -1010. Yin RK. Pesquisa qualitativa do início ao fim. Porto Alegre: Penso; 2016.. This moment provided opportunities for exchanges and the return of part of the research data to the participants, including the delivery of the genogram.
To develop the study, it was respected Resolution 466/12 of the National Health Council of the Ministry of Health, which addresses the guidelines and standards for research involving human beings1212. Ministério da Saúde (BR), Conselho Nacional de Saúde. Resolução nº 466, de 12 de dezembro de 2012. Diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Diário Oficial da União. 2013 [cited 2020 Mar 25] jun 13;150(112 Seção 1):59-62. Available from: http://conselho.saude.gov.br/resolucoes/2012/Reso466.pdf
http://conselho.saude.gov.br/resolucoes/...
. It received approval from the Research Ethics Committee of the State Foundation for Health Research and Production, under statement No. 671,719, and CAAE nº 30774014,1,0000,5320. By signing the Free and Informed Consent Form, the participants agreed to participate in the research, being presented the objectives, the guarantee of anonymity, free access to data and results and the freedom to give up at any time. In order to preserve their identity, they were identified by the letter "H", of hemophiliac man, followed by an Arabic numeral following the sequence of the interviews, plus age.
RESULTS AND DISCUSSION
First, a chart is presented a with a brief characterization of men with hemophilia participating in the study (Chart 1):
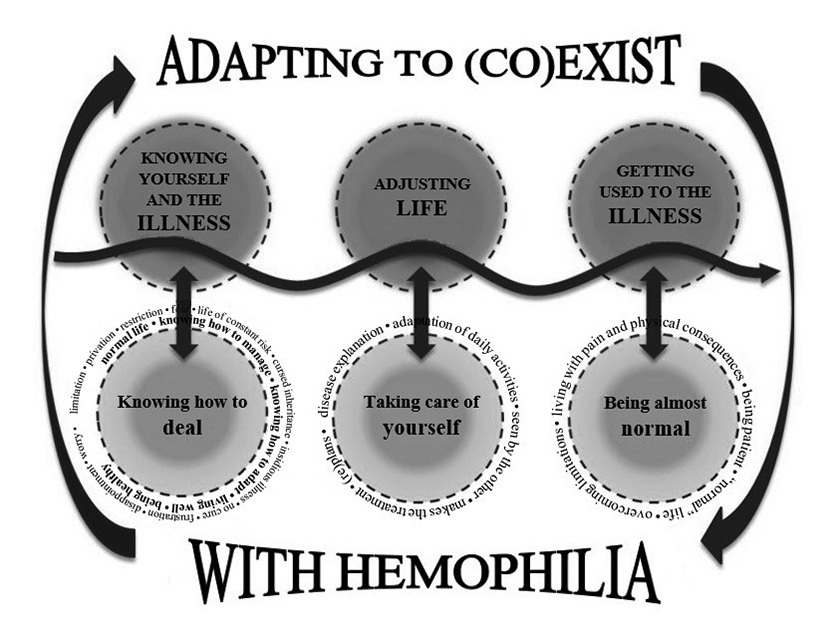
From the data analysis, the theoretical model was built: Adapting to (co)exist with hemophilia (Figure 1), composed by the categories Knowing yourself and the illness: knowing how to deal, Adjusting life: taking care of yourself and Getting used to the illness: being almost normal.
The option to use the expression (co)exist instead of the words to live and/or to coexist together is a stylistic and semantic resource. The objective is to emphasize the process of living with hemophilia, which demands continuous adaptations. Thus, it is not only a matter of living with the illness, but of actions of the man in this process.
The central category that represents the theoretical model of the experience of men with hemophilia was identified as Adapting to (co)exist with hemophilia. In this sense, the meaning of the experience is related to constantly adapting to (co)exist with hemophilia.
The adaptation in chronic illness is understood as the adjustment that people make to the different contexts in which they get involved and act, considering the specifics of their illness. For example, the pain and absences resulting from hospitalizations express the need for continuous adaptations1313. Pais SC, Menezes I. How do we live with chronic disease? a rights-based approach promoting the wellbeing of children with chronic disease. Cienc Saude Coletiva. 2019;24(10):3663-72. doi: https://doi.org/10.1590/1413-812320182410.17932019
https://doi.org/10.1590/1413-81232018241...
.
This is a dynamic process that occurs throughout the life cycle of men with hemophilia, usually starting in childhood. Even when they did not have or understood the diagnosis, they already lived with the illness’ signs and symptoms, as well as with the sequelae that came with the difficulty in the treatment, requiring continuously adaptations.
Through the self the person talks to himself, is aware of himself, perceives and evaluates the other and himself, recognizes the influence of the other in him and vice versa, thinks, analyzes what he does, makes decisions, defines how to act in a determined situation, plans, tests plans, evaluates and reevaluates77. Blumer H. Symbolic interactionism: perspective and method. Englewood Cliffs: Prentice-Hall; 1969.-88. Charon JM. Symbolic interactionism: an introduction, an interpretation, an integration. 10th ed. Boston: Prentice Hall; 2010.,1414. Sanderstrom KL, Martin DD, Fine GA. Símbolos, selves e realidade social: uma abordagem interacionista simbólica à psicologia social e à sociologia. Petrópolis: Vozes; 2016.. Thus, men with hemophilia constantly perceive and evaluate ways of better living in their daily lives. And it is not conditioned or manipulated by the environment, since it is able to interpret, plan, evaluate and control the situation.
There are three realities, physical (concrete), social (apparent) and internal (personal). In physical and social reality, initially a person responds physically to a certain stimulus or interaction, but then, based on the interpretation of the fact, he will decide a line of action, of how to react socially. In the internal reality, there is a personal interpretation that interprets the events and gets its own conclusions that can be divergent from one person to another, who experienced the same situation88. Charon JM. Symbolic interactionism: an introduction, an interpretation, an integration. 10th ed. Boston: Prentice Hall; 2010.. The men in this study acted according to their interpretation, making adaptations for life.
This theoretical model integrates three categories that emerged and represent the experience of men, aiming to demonstrate the adaptations in the (co)existence with hemophilia: Knowing yourself and the illness: knowing how to deal, Adjusting life: taking care of yourself and Getting used to the illness: being almost normal.
Knowing yourself and the illness: knowing how to deal begins the process of experience, when men define it using symbols with negative and positive meanings. This definition demonstrates the temporality between a past in childhood and a present as an adult. They redefine perceptions and concepts, thus, in childhood, the negative aspects stand out, but over time they readapt and interpret the illness in a more positive way. Even so, they demonstrate to always live in a duality of feelings and perceptions.
Thus, this category demonstrates the ability of men to deal with hemophilia even with difficulties, being characterized by symbols with negative and positive meanings. The symbols with negative meanings are: limitation, privation, restriction, fear, life of constant risk, cursed inheritance, insidious illness, no cure, frustration, disappointment and worry.
I think it is the limitation that I have of not being able. Hemophilia, for me, is not having an exaggeration in the things I do. [...] Other than that, I don't have hemophilia (H8, 45 years).
For me, I think it is a privation of a lot of things, fear of a lot of things. More fear and privation, I think. [...] It is privation of not being able to do everything we can and afraid that we will not know what will happen. With me, it happened to be well and in seconds I had a hemorrhage and the doctors deceived me. This I think is fear (H10, 39 years).
He (physician) forbade me to play ball, any game that had an impact. So that was a very frustrating thing, very disappointing even. [...] Like the conscious hemophiliac today that is easier to take care, but at the time the teenager I discovered it was not easy. Which is something that the person does not accept (H11, 39 years).
In positive symbology, the category comprises symbols with positive meanings: practically normal life, knowing how to manage and adapt, to live well and be healthy.
It is living adapting for that day, for that hour, for that moment, and without much planning over a long distance (H1, 24 years).
No problem, we live with it, we have already learned to live with it (H5, 52 years).
For me, having hemophilia is this: you have to know how to deal with the things you can or cannot do. You have to know, also, that in the future I may have hemophiliac children or hemophiliac grandchildren. So you have to know, you have to understand how it works so that you can also take care of your future children (H7, 19 years).
The adaptation process is interrelated to learning to live with limitations and knowing how to manage them, which delimit men’s actions. And this learning happens throughout your life.
Thus, in the negative view of men, hemophilia is the limitations and adversities with which they live daily. It is living with a treacherous illness that has no time to manifest, a reason for privation and fear and, above all, incurable. They never know what will or will not happen, because at any time it can bleed spontaneously without necessarily suffering any trauma.
In the meantime, they are apprehensive about the possibility of a serious bleeding that can lead to death. In view of this, they do not know tomorrow, due to the unpredictability of the illness. In this context, fear can become one of the main adaptation mechanisms, because it helps to overcome obstacles and to try to avoid problems.
Still, they treat hemophilia as something more abstract, just an invisible and untouchable word. This is because they consider it as the difficulties of everyday life and what is felt concretely, as pain in the joints. Having hemophilia does not cause restrictions, but having a hemarthrosis does, because this is real and bring limitations.
Another data that emerges is the concern about the transmissibility of hemophilia, a cursed inheritance, to the children. The man is afraid of transmitting hemophilia to the next generations for what he has already suffered, but at the same time, he is aware that the treatment has evolved, knows and understands the illness, knows what care to teach and the necessary support for the good living with it , being able to help the family, if it occurs in their descendants. From self, mind and human action, he knows that hemophilia can affect other people, in this case the family as a society, which can trigger anxiety about the unpredictable future1515. Saltnes SS, Geirdal AO, Saeves R, Jensen JL, Nordgarden H. Experiences of daily life and oral rehabilitation in oligodontia - a qualitative study. Acta Odontol Scand. 2019;77(3):197-204. doi: https://doi.org/10.1080/00016357.2018.1535137
https://doi.org/10.1080/00016357.2018.15...
.
Regarding the positive interpretation of hemophilia, healthy people are considered, which they attribute to the fact of taking care of themselves. Despite this, they believe that when they get older they will have some sequel. It is noticed that their vision is built through interaction with others and with the illness, their perception, observation, conversation with themselves and interpretation. There is also the internal reality, experienced and elaborated by the person. Also, they emphasize the importance of knowing yourself and the illness with the perspective of enhancing your care for healthy living.
Thus, health professionals are important actors in this process, in the sense of realizing that each person’s experience is unique, which knows how to define their feelings and the meanings of the illness. Therefore, it is up to the other to respect their knowledge and accept their needs.
Each person has an individuality, which is different from another. Consequently, their experiences of interactions, positions, cultures and socialization are unique, which can change over time88. Charon JM. Symbolic interactionism: an introduction, an interpretation, an integration. 10th ed. Boston: Prentice Hall; 2010.,1414. Sanderstrom KL, Martin DD, Fine GA. Símbolos, selves e realidade social: uma abordagem interacionista simbólica à psicologia social e à sociologia. Petrópolis: Vozes; 2016.. Thus, it is essential to listen to users, as there is a need to understand what they think to undertake care. This attitude is believed to positively interfere in the relationship between the professional and the user.
The positive effect of therapeutics is also related to an individualized and welcoming service by health professionals, who need to be attentive to the needs of each user and provide support, which occurs through a relationship of trust, dialogue and guidance1616. Budó MLD. Cuidado sociocultural en el sentido práctico: en busca del cuidado con sentido [editorial]. Cult Cuid. 2016;XX(45):9-11. doi: https://doi.org/10.14198/cuid.2016.45.01
https://doi.org/10.14198/cuid.2016.45.01...
-1717. Feijó AM, Santos BP, Schwartz E, Fernandes AJF, Lutz T, Linck CL. Família: principal vínculo apoiador do homem com câncer. Enferm Rev. 2018 [cited 2020 Feb 27];21(2):2-15. Available from: http://periodicos.pucminas.br/index.php/enfermagemrevista/article/view/18819
http://periodicos.pucminas.br/index.php/...
. Although health professionals are provided with greater knowledge, participants believe they should know more about the illness, treatment, and care. Research that investigated the knowledge, attitudes and behaviors of young men with hemophilia pointed out that despite the information provided by the health team, these men considered, above all, their own experience, as they realized that they knew themselves better1818. Torres‐Ortuño A, Cuesta‐Barriuso R, Nieto‐Munuera J, Galindo‐Piñana P, López‐Pina JA. Coping strategies in young and adult haemophilia patients: a tool for the adaptation to the disease. Haemophilia. 2019;25(3):392-7. doi: https://doi.org/10.1111/hae.13743
https://doi.org/10.1111/hae.13743...
.
It is noteworthy that man experiences, interprets, perceives and defines hemophilia in its uniqueness, using symbols, such as treacherous illness. And from this perspective, he takes care of himself and adjusts his life.
Adjusting life: taking care of yourself is the category that characterizes man’s actions making adaptations to (co)exist with hemophilia, which occurs when he knows himself and the illness. This category also demonstrates a temporality, justified by the comparison between the past and the present, childhood, and adulthood.
As a child, had difficult to understand the importance of care, while, over time and in adulthood, he perceives activities that serve as protection to not trigger bleeding, pain and physical sequelae. He defines that it is not only the past that influences, but that the cause of the actions is also the result of what is happening in the present.
This category is characterized by actions involving adaptations undertaken in care to live better. The man with hemophilia explains his illness, adapts his daily activities, is seen by the other, undergoes treatment and (re)plans.
Back in high school, kids wanted to play ball. So we got in the middle and we couldn't, then it hurt, I stayed eight days, fourteen days at home, in bed, I couldn't even move. And then sometimes it was eight days, ten days without sleeping, sitting on the bed, I couldn't even lie down. So that was a very bad time (H5, 52 years).
It was harder when I was younger. The kid likes to play ball, likes to play football, likes to skate and all that. Whether or not I was a little bit prived because of my health. But today it’s easier, today I accept it better and live well with her(hemophilia), because there are some things that we cannot do, but there are others that do not prevent anything. The fact that I study, I also do swimming, which is something I like, so these things don't stop me. So today I can live well with hemophilia without any problem (H7, 19 years).
There was no treatment. Treatment was absolute rest. And when it was something very serious like a bruise or a cut, it was lowering and making plasma and putting blood, which was something that made me very uncomfortable [...] I went down, stayed for a month, didn't see any results. And even when I was discharged home, I knew that at least once, twice a year, I had to go down to make the plasma because it gave spontaneous bleeding, bleeding in the urine. So, many, a little cut that never stopped. [...] I started using factor I was 28 years old. Before that, I had severe surgery on my right arm. When I was 16, I moved to Porto Alegre. And I had a month off, I did the cryoprecipitate, where hepatitis C happened. At the age of 28 years old, they called me here at the Blood Center, found my file and started to do the treatment with factor VIII. [...] There was no physician who treated hemophiliacs, so I was a teenager, and I was still treating myself with a pediatrician. And then I slept on my arm, the arm swelled and even it started to bleed. And then I had to stay in Rio Grande, Rio Grande moved to Porto Alegre, which was the only reference I had on hemophiliac (H11, 39 years).
I started doing factor in 2001. The history of factor I have from 2001 backwards is factor VIII, and my factor is IX. So, I had no factor tracking, and what happens? He didn’t come to work, the boss, the chief, I don’t know what he’s going to understand, that’s killing service, that whole story. It is already another case, then I explain the following day: this, this and this happened to me. I had a muscle pain and my ankle is swollen and my wrist and any part of my body where I put the extra strain on that task and presented me with this illness. No one believes. [...] It's okay that you have your limitations, but your limitations, what rule over them? The emotional rules them, the emotional rules everything. [...] I was the house nurse. I was going to their house (hemophiliacs). There was no reason, I recognized his pain, I already felt it. So I used to say: don't move. I already knew the vein that hurt, the one that didn't hurt to the needle. So I knew the whole situation. And they didn't, because there is no physical situation worse than mine. They didn't do it because the emotional wouldn't let it, but why me? So it's that kind of situation, did the factor on them (H12, 40 years).
And then the joints, if it swelled you put an ice pack, you make a factor. If you don't know how to apply, you come to where the Blood center is, you look for it, send someone else to do it. We already did it, we applied it for about three years.[...] We learned doing hard. [...] So, the person with hemophilia who already knows the diagnosis says to the physician: I can't do muscle injection, I can't take anything like that, ASA (acetylsalicylic acid), anticoagulant and such. You already know, already give a guide: look, I do this, I do that [...] But at that time, there was no hemophilia at that time, the guy lived stubbornly (H2, 49 years).
Whenever the hemophiliac has a break, he has to have a plan B, and then adaptations begin. [...] It is a illness that nowadays is very controlled, you do prophylaxis, you have good doctors to take care of you, you have a team already prepared for all that. And you end up creating this awareness also by taking care of yourself and to have a longer life with the lowest possible degree of joint damage and mobility impairment in the future (H4, 28 years).
I take care of myself, that I know I have limits. Depending on whether I can suffer even an injury, I can get hurt. So, I try to balance what I can and what I cannot do (H9, 22 years).
Men always need to adapt, which they learn from childhood, when they start to realize that care is part of their daily lives so that they can perform some activities instead of others. But it was not always “easy” to understand that they could not play ball like other children or suffer prejudice.
Participants of a study, active sportsmen, reported that in order to continue practicing their sports, they had to adapt their treatment to the developed activity and assume responsibility and treatment planning1919. von Mackensen S, Hilberg T, Valentino LA, Kurnik K, Khair K. Validation of the Haemophilia & Exercise Project‐Test‐Questionnaire (HEP‐Test‐Q) - an instrument for the assessment of subjective physical functioning in children with haemophilia. Haemophilia. 2018;24(6):888-95. doi: https://doi.org/10.1111/hae.13533
https://doi.org/10.1111/hae.13533...
. Upon learning the risks, men with hemophilia are ready to act, as they did in childhood, and in the face of any abnormality, they are alert and seek help, not leaving it until later. Therefore, the feeling that it is necessary to act immediately remains in the behavior of men.
The hemophiliac man knows how to recognize bleeding, as he learns the signs and symptoms since childhood. This long experience empowers him, allows to get to know the treatment, how and when to infuse the coagulation factor, know what to do to reduce pain and also what not to do to avoid it. In this way, he realizes, reflects, and influences himself (self), and acts with his mind. The knowledge of the illness and the way to act in case of bleeding or musculoskeletal injury on the part of men was also the result of another research1818. Torres‐Ortuño A, Cuesta‐Barriuso R, Nieto‐Munuera J, Galindo‐Piñana P, López‐Pina JA. Coping strategies in young and adult haemophilia patients: a tool for the adaptation to the disease. Haemophilia. 2019;25(3):392-7. doi: https://doi.org/10.1111/hae.13743
https://doi.org/10.1111/hae.13743...
.
During childhood they had many restrictions, it was marked by a time when there was no adequate treatment for hemophilia and was little known, therefore, some suffered from late and incorrect diagnoses and inadequate treatments, which resulted in several sequels, such as hemophilia arthropathies and infectious diseases. The coagulation factor was not available or when it started to be used only on demand, that is, after bleeding. They were usually transfused with the cryoprecipitate blood component and, to relieve pain, they used analgesics and anti-inflammatory drugs. They spent days and months in hospitals, emergency rooms or at home, at the mercy of health professionals who were unaware of the diagnosis, which caused constant adaptations, such as absences at school and at work.
A study shows that bleeding, physical limitations and restrictions impact social activities, school, and work. Some issues are related to absences due to these problems and because they remain in hospital for long periods of time for treatment1515. Saltnes SS, Geirdal AO, Saeves R, Jensen JL, Nordgarden H. Experiences of daily life and oral rehabilitation in oligodontia - a qualitative study. Acta Odontol Scand. 2019;77(3):197-204. doi: https://doi.org/10.1080/00016357.2018.1535137
https://doi.org/10.1080/00016357.2018.15...
. However, nowadays, with the presence of the coagulation factor and prophylactic therapy they can do what they were unable to do in childhood, having a practically normal life. Therefore, living with hemophilia at that time has become easier, as they have access to treatment, referral centers and assistance. Even for those who already have sequelae, who remain with difficulties.
In this context, in addition to the need for men with hemophilia to adapt to be able to continue studying and working, they live with people's ignorance about their illness. Society does not believe or understand hemophilia. Therefore, studying and working depends on the understanding of others, because in the face of bleeding, men are often unable to perform their activities normally.
When they have a physical disability, society labels them for what they see externally, the physical situation, calling them poor people. However, even with physical disabilities like the other, what differentiates is hemophilia, because with the physical problem or physical disability, he is able to overcome and go beyond, while the greatest obstacle is pain. And in this situation, in addition to physical pain, they feel emotional pain.
Although the interaction between hemophiliac men and other people has given the illness visibility, it is still not well understood. However, study participants believe that it is always important in these relationships to pass on information, even if people do not understand or give value to the illness.
In a study conducted with men, they reported that people in general were not aware of what is the experience of living with the illness2020. Myung G, Harada ND, Fong SL, Aquino-Beaton C, Fong CD, Fang MA. Stigma and medication adherence in patients with rheumatic disease. J Psychosom Res. 2019;125:109791. Available from: https://doi.org/10.1016/j.jpsychores.2019.109791
https://doi.org/10.1016/j.jpsychores.201...
. In the study in which participated men with hemophilia, they reported feeling stigmatized and believing in the existence, still, of many stereotypes about people with hemorrhagic disorders. They suffered discrimination because of their condition, particularly at school and at work, due to the lack of knowledge and understanding of other people about the illness and the treatment1515. Saltnes SS, Geirdal AO, Saeves R, Jensen JL, Nordgarden H. Experiences of daily life and oral rehabilitation in oligodontia - a qualitative study. Acta Odontol Scand. 2019;77(3):197-204. doi: https://doi.org/10.1080/00016357.2018.1535137
https://doi.org/10.1080/00016357.2018.15...
.
This attitude occurs by the communication of man with his self (mind), causing human action. Still, with social interaction they found other meanings that made them act so that they could (co)exist with the illness and achieve their life goals. The expectations of others are considered, influencing their plans and directions.
In symbolic interactionism, society depends on people continuously interacting with each other and with himself77. Blumer H. Symbolic interactionism: perspective and method. Englewood Cliffs: Prentice-Hall; 1969.-88. Charon JM. Symbolic interactionism: an introduction, an interpretation, an integration. 10th ed. Boston: Prentice Hall; 2010.. In the situation of men with hemophilia, the interaction between health professionals and users has made the illness better known and understood in this environment, leading to the evolution of treatment and in better care. While for society as a whole, the interaction helped to understand the illness and its meaning, although sometimes it is not well understood.
It is highlighted the power of social interaction for the (re)construction of thoughts and attitudes or even clarification of a certain situation. Men seek to mobilize themselves to resume social activities or to reinsert themselves in the labor market, as they have the need to adapt activities and life, giving a new meaning to hemophilia. In the adaptation process, men continually (re)plan or have a plan B, which demonstrates that they learned to (co)exist with the illness, living one day at a time.
They live with physical pain constantly, whether due to the occurrence of bleeding, commonly in the joints, or due to the physical sequelae caused by these repetitive bleeds. Until 2011, when the coagulation factor was only used on demand, they suffered much more from pain, but learned about the need for self-care to avoid pain. For example, when they bleed, they infuse the coagulation factor, apply ice and rest.
Thus, when living with hemophilia since childhood, they use symbols to talk to themselves (self and mind) and learn how to act (human action), in case, the care and adaptations they perform. They go through something, perceive, interpret, plan and act.
The adaptation process involves adapting their activities due to bleeding and pain. But to take care and adapt, they need to have something or think they will, which they perceive from experience, as also found in another study, in which men compared current symptoms with others already presented in the past1818. Torres‐Ortuño A, Cuesta‐Barriuso R, Nieto‐Munuera J, Galindo‐Piñana P, López‐Pina JA. Coping strategies in young and adult haemophilia patients: a tool for the adaptation to the disease. Haemophilia. 2019;25(3):392-7. doi: https://doi.org/10.1111/hae.13743
https://doi.org/10.1111/hae.13743...
.
The fact of experiencing hemophilia for a long period of time, even without a defined diagnosis, made them empower themselves in all aspects, from the biological to the emotional. In some moments they manage to go further, in others they do not, but even with the limitations and difficulties they always find ways to develop their daily activities or know the time to stop and restart.
The man with hemophilia needs to know himself (self) and the illness with the intention of not suffering from his actions, allowing him to coexist with hemophilia. Furthermore, the relationship you have with yourself can help or hinder. For example, you know your health condition, having clarity of care and the importance of having trained professionals for this and, even, with the awareness that the emotional situation affects physically, requiring self-control. It is also important to have willpower and solidarity with your peers, which in this case, is to know what the other feels, the moment they assume the role of the other.
Getting used to the illness: being almost normal is the category that expresses the consequences of the actions of men who make adaptations to (co)exist with hemophilia. The man with hemophilia needs to know himself, the illness, and the care so that his actions result in consequences, such as not having bleeding, pain and physical sequelae.
The man with hemophilia learns and gets used to coexist with pain and physical consequences, to be patient, to have a “normal” life and to overcome the limitations. Like the other categories, this one also shows a temporality for comparing past and present.
For me, the hemophilia [...] that we know, know what it is, the disorders that it brings, the sequalae that it leaves, for me it is now practically common, normal (H2, 49 years).
I am 55 years old and I think I didn’t take five years out of which I had no pain, the rest every day we feel pain (H3, 55 years).
My leg hurts, my arm hurts, but I'm used to it, I know how to take it. But it is a battle, you have to take care of yourself (H6, 51 years).
So, you have to know yourself, you have to know, otherwise who is going to suffer the consequences of your actions is yourself. [...] Within your limitation, you start creating courage. I am limited, but I want to get over it (H12, 40 years).
Men, because they know hemophilia, prefer to coexist with it instead of another disease, which is due to the experience they have, the time of interaction. Hemophilia is part of their lives as if it were a characteristic, permanent and natural. They get used to their obstacles and the adaptations they need to make constantly, having a practically normal life. As a result, hemophilia interferes with man’s choices and life.
In relation to physical pain, it is part of the daily life of the man with hemophilia who has sequelae, but also of the one who does not have it, because it appears at any time due to bleeding without warning. However, they get used to the pain and make adaptations, whether in small activities, in study or at work. They cannot stop because of hemophilia limitations, because there is always something, so they constantly (re)plan and adapt their plans, demonstrating the importance of their dynamism.
In the meantime, the biggest problem that destabilizes the hemophiliac man is pain, which is the most difficult part of hemophilia. So, your problem is not the physical disability because apparently it is the same as the others physically, but the hemophilia, the bleeding, the pain, the adaptation you need to do and the care you need to have to avoid them, this is the difference in relation to the others. In his self he knows that he needs to make adaptations, so with his mind he acts (human action) to reach his goal. In this context, pain limits daily activities, such as work, study, and physical activity, and can influence quality of life.
The learning of the illness’ time reflects on men as people, redefining their self and their ways of perceiving life and those who are part of it. There are several qualities learned by men, among them, tolerance, and patience. They believe that they have learned to coexist better with adversity, to listen and respect the other, to value people and things as they are and to give importance to what really has value.
For men, hemophilia is an illness that requires care, they need to know, know how to manage and make adaptations, that is, (co)exist with it. So, they decide to follow new paths and overcome the illness because they have symbols, self and mind to think, interpret and (re)define the different situations they experience in their life.
Given the exposed, the person is an active being who has self and mind, uses symbols to communicate and represent, solves problems, thinks, and makes choices, taking him to new paths. Furthermore, he is a social being, as the social context changes, he also changes88. Charon JM. Symbolic interactionism: an introduction, an interpretation, an integration. 10th ed. Boston: Prentice Hall; 2010.,1414. Sanderstrom KL, Martin DD, Fine GA. Símbolos, selves e realidade social: uma abordagem interacionista simbólica à psicologia social e à sociologia. Petrópolis: Vozes; 2016.. In men with hemophilia, their self is redefined in the face of changes, for fear of bleeding, pain and death. Always in a time of struggle, new transformations are imposed on them, who need to reorganize their roles, readapting the self and learning new skills to deal with hemophilia.
CONCLUSION
The theoretical model reveals the experience of men who make various adaptations to be able to (co)exist with the hemophilia and the motivation for their actions and behaviors, resulting from the definition and redefinition of the self, aiming to preserve their life away from bleeding, pain and of the risk of death, which is reinforced with the evidences of the knowledge about the illness built over the years and aware in adulthood. In this sense, they adapt to (co)exist with hemophilia, beginning the process by knowing themselves and the illness, by defining hemophilia with symbols and their meanings and knowing how to deal with fear, privation, and adaptations. They act by adjusting their lives and taking care of themselves, involving treatment, adaptations of daily activities, the view of the other, the explanation of the illness and the (re)making of their plans and, consequently, getting used to the illness, when they live with the pain and the physical consequences, and try to take a “normal” life.
In the meantime, this study gives men a voice and visibility to hemophilia with society and health professionals, as well as making it possible to know and expand the problematic of these men. Knowing their experience can help families of children and adolescents with hemophilia, empowering them regarding their actions, behaviors and treatment.
Still, the results of this research serve as a warning for the importance of the knowledge of health professionals about what it is like for the person (co)exist with hemophilia, so that they know that the meaning and the way of living is defined from the guidance provided in the course of the experience, as well as assisting in early diagnosis and offering adequate monitoring and treatment, collaborating for quality of life. It also shows a fertile and important field for Nursing care for people with coagulopathies and how much can be contributed to the knowledge of the experience with hemophilia, that until now is little explored.
It should be added that the study has limitations, as it worked with the subjectivity of each person and the results found are linked to it, so they cannot be generalized. It is important to notice that all men had the severe form of hemophilia, in which bleeding is more frequent and can occur spontaneously. Therefore, it may be that the experience of men with mild or moderate hemophilia is different. In view of the above, it is reinforced in the academic scope, of teaching and research fields, the need for greater enterprise in the problem of hemophilia and the realization of more qualitative research focusing on this thematic, in order to deepen knowledge.
Acknowledgment
To the Coordination for the Improvement of Higher Education Personnel (CAPES) for the scholarship of the Sandwich Doctorate Program Abroad (PDSE) - Proc. No. 99999,004522/2014-01.
REFERENCES
- 1. Castellone DD, Adcock DM. Factor VIII activity and inhibitor assays in the diagnosis and treatment of hemophilia A. Semin Thromb Hemost. 2017;43(3):320-30. doi: https://doi.org/10.1055/s-0036-1581127
» https://doi.org/10.1055/s-0036-1581127 - 2. Sokołowska B, Kozińska J, Kozioł M, Wąsik-Szczepanek E, Szczepanek D, Hus M. Diagnosis and treatment of acquired hemophilia: a single-center experience. Pol Arch Intern Med. 2017;127(11):796-9. doi: https://doi.org/10.20452/pamw.4139
» https://doi.org/10.20452/pamw.4139 - 3. Soucie JM. Global hemophilia care: data for action. Ann Intern Med. 2019;171(8):585-6. doi: https://doi.org/10.7326/M19-2535
» https://doi.org/10.7326/M19-2535 - 4. Martin A, Mulhern B, Shaikh A, Asghar S, O'Hara J, Pedra G, et al. Disease state adaptation experienced by patients with hemophilia: literature review and expert consensus. Blood. 2019;134(Suppl 1):5801. doi: https://doi.org/10.1182/blood-2019-124396
» https://doi.org/10.1182/blood-2019-124396 - 5. Gupta N, Benbouzid A, Belhani M, El Andaloussi M, Maani K, Wali Y, et al. HAEMOcare: the first international epidemiological study measuring burden of hemophilia in developing countries. TH Open. 2019;3(2):e190-9. doi: https://doi.org/10.1055/s-0039-1688414
» https://doi.org/10.1055/s-0039-1688414 - 6. Thomazelli CF, Lemos JM, Marques CLBB. Percepção dos portadores de hemofilia sobre a atuação do enfermeiro. Saúde Biociênc. 2019 [cited 2020 Mar 25];1(1):18-33. Available from: http://unifatea.com.br/seer3/index.php/saudebiociencias/article/view/1096/1011
» http://unifatea.com.br/seer3/index.php/saudebiociencias/article/view/1096/1011 - 7. Blumer H. Symbolic interactionism: perspective and method. Englewood Cliffs: Prentice-Hall; 1969.
- 8. Charon JM. Symbolic interactionism: an introduction, an interpretation, an integration. 10th ed. Boston: Prentice Hall; 2010.
- 9. Charmaz K. A construção da teoria fundamentada: guia prático para análise qualitativa. Porto Alegre: Artmed; 2009.
- 10. Yin RK. Pesquisa qualitativa do início ao fim. Porto Alegre: Penso; 2016.
- 11. Wright LM, Leahey M. Enfermeiras e famílias: um guia para avaliação e intervenção na família. 5. ed. São Paulo: Roca; 2012.
- 12. Ministério da Saúde (BR), Conselho Nacional de Saúde. Resolução nº 466, de 12 de dezembro de 2012. Diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Diário Oficial da União. 2013 [cited 2020 Mar 25] jun 13;150(112 Seção 1):59-62. Available from: http://conselho.saude.gov.br/resolucoes/2012/Reso466.pdf
» http://conselho.saude.gov.br/resolucoes/2012/Reso466.pdf - 13. Pais SC, Menezes I. How do we live with chronic disease? a rights-based approach promoting the wellbeing of children with chronic disease. Cienc Saude Coletiva. 2019;24(10):3663-72. doi: https://doi.org/10.1590/1413-812320182410.17932019
» https://doi.org/10.1590/1413-812320182410.17932019 - 14. Sanderstrom KL, Martin DD, Fine GA. Símbolos, selves e realidade social: uma abordagem interacionista simbólica à psicologia social e à sociologia. Petrópolis: Vozes; 2016.
- 15. Saltnes SS, Geirdal AO, Saeves R, Jensen JL, Nordgarden H. Experiences of daily life and oral rehabilitation in oligodontia - a qualitative study. Acta Odontol Scand. 2019;77(3):197-204. doi: https://doi.org/10.1080/00016357.2018.1535137
» https://doi.org/10.1080/00016357.2018.1535137 - 16. Budó MLD. Cuidado sociocultural en el sentido práctico: en busca del cuidado con sentido [editorial]. Cult Cuid. 2016;XX(45):9-11. doi: https://doi.org/10.14198/cuid.2016.45.01
» https://doi.org/10.14198/cuid.2016.45.01 - 17. Feijó AM, Santos BP, Schwartz E, Fernandes AJF, Lutz T, Linck CL. Família: principal vínculo apoiador do homem com câncer. Enferm Rev. 2018 [cited 2020 Feb 27];21(2):2-15. Available from: http://periodicos.pucminas.br/index.php/enfermagemrevista/article/view/18819
» http://periodicos.pucminas.br/index.php/enfermagemrevista/article/view/18819 - 18. Torres‐Ortuño A, Cuesta‐Barriuso R, Nieto‐Munuera J, Galindo‐Piñana P, López‐Pina JA. Coping strategies in young and adult haemophilia patients: a tool for the adaptation to the disease. Haemophilia. 2019;25(3):392-7. doi: https://doi.org/10.1111/hae.13743
» https://doi.org/10.1111/hae.13743 - 19. von Mackensen S, Hilberg T, Valentino LA, Kurnik K, Khair K. Validation of the Haemophilia & Exercise Project‐Test‐Questionnaire (HEP‐Test‐Q) - an instrument for the assessment of subjective physical functioning in children with haemophilia. Haemophilia. 2018;24(6):888-95. doi: https://doi.org/10.1111/hae.13533
» https://doi.org/10.1111/hae.13533 - 20. Myung G, Harada ND, Fong SL, Aquino-Beaton C, Fong CD, Fang MA. Stigma and medication adherence in patients with rheumatic disease. J Psychosom Res. 2019;125:109791. Available from: https://doi.org/10.1016/j.jpsychores.2019.109791
» https://doi.org/10.1016/j.jpsychores.2019.109791
Publication Dates
-
Publication in this collection
21 May 2021 -
Date of issue
2021
History
-
Received
03 June 2020 -
Accepted
04 Nov 2020

 Source: The Authors, 2015
Source: The Authors, 2015