Abstracts
OBJECTIVE: To assess whether the change in body mass index Z-score for age >0.67 in the first year of life was associated with overweight at preschool age. METHODS: A cohort study nested in a randomized field trial conducted in São Leopoldo, Rio Grande do Sul, Southern Brazil. Data on weight and height of children at birth, from six to eight, and from 12 to 16 months were collected. From ages three to four, besides these data, waist circumference was measured. Weight gain was calculated by the difference in body mass index/age Z-score from 12 to 16 months in relation to that at birth, adopting as cutoff >0.67 Z-score for weight gain. Waist-to-height ratio was calculated, and the excess of central adiposity was considered for values >0.5. Multivariate analysis to test the association between outcomes and independent variables was applied. RESULTS: The prevalence of excessive weight gain in the first year of life was 29.5% out of the 338 studied children. After adjustment for gender, origin group, birth weight, duration of exclusive breastfeeding and mother's body mass index, the change in >0.67 Z-score from birth to 12 to 16 months was an independent risk factor for overweight (RR 2.81, 95%CI 1.53-5.16) and for elevated waist-to-height ratio (RR 2.10, 95%CI 1.19-3.72) in preschool age. CONCLUSIONS: Excessive weight gain in the first year of life was associated with overweight and high abdominal adiposity at preschool age.
weight gain; adiposity; child, preschool
OBJETIVO: Avaliar se a mudança no escore Z do índice de massa corpórea por idade >0,67 no primeiro ano de vida se associou ao excesso de peso na idade pré-escolar. MÉTODOS: Estudo de coorte aninhado a ensaio de campo randomizado realizado na cidade de São Leopoldo, no Rio Grande do Sul. Foram coletados dados de peso e estatura das crianças ao nascimento, dos seis aos oito meses e dos 12 aos 16 meses. Aos três e aos quatro anos, além destes dados aferiu-se a circunferência da cintura. Calculou-se o ganho de peso pela diferença no escore Z do índice de massa corpórea/idade dos 12 até os 16 meses em relação ao índice de massa corpórea/idade ao nascimento, adotando-se ponto de corte >0,67 para ganho de peso excessivo. A relação cintura/estatura foi realizada, considerando-se excesso de adiposidade central se valores >0,5. Utilizou-se a análise multivariada para o teste da associação entre os desfechos e as variáveis independentes. RESULTADOS: A prevalência do ganho de peso excessivo no primeiro ano de vida foi de 29,5% de um total de 338 crianças. Após ajuste para as variáveis sexo, grupo, peso ao nascer, tempo de aleitamento materno exclusivo e índice de massa corpórea da mãe, a mudança no escore Z >0,67 do nascimento até os 12 a 16 meses apresentou-se como fator de risco para o excesso de peso (RR 2,81; IC95% 1,53-5,16) e elevada relação cintura/altura na idade pré-escolar (RR 2,10; IC95% 1,19-3,72). CONCLUSÕES: O ganho de peso excessivo no primeiro ano de vida está associado ao excesso de peso e à elevada adiposidade abdominal na idade pré-escolar.
ganho de peso; adiposidade; pré-escolar
OBJETIVO: Evaluar si el cambio en el escore Z del Índice de Masa Corporal (IMC) por edad >0,67 en el primer año de vida se asoció al exceso de peso en la edad pre-escolar. MÉTODOS: Estudio de cohorte aunado a ensayo de campo aleatorio realizado en la ciudad de São Leopoldo (Rio Grande do Sul). Se recogieron datos de peso y estatura de los niños al nacer, 6 a 8 y 12 a 16 meses. A los 3 a 4 años de edad, se verificó también la circunferencia de la cintura. Se calculó la ganancia de peso por la diferencia en el escore Z de IMC/Edad a los 12 a 16 meses respecto al IMC/Edad al nacer, adoptando punto de corte >0,67 para ganancia de peso excesiva. Relación cintura/estatura fue realizada, considerando exceso de adiposidad central valores >0,5. Se utilizó el análisis multivariado para probar la asociación entre los desenlaces y las variables independientes. RESULTADOS: La prevalencia de ganancia de peso excesiva en el primer año de vida fue de 29,5% de un total de 338 niños. Después del ajuste para las variables sexo, grupo, peso al nacer, tiempo de lactancia materna exclusiva e IMC de la madre, el cambio en el escore z >0,67 del nacimiento hasta los 12 a 16 meses se presentó como factor de riesgo para excesos de peso (RR 2,81; IC95% 1,53-5,16) y elevada relación cintura/altura en la edad pre-escolar (RR 2,10; IC95% 1,19-3,72). CONCLUSIÓN: Ganancia de peso excesivo en el primer año de vida está asociada a exceso de peso y elevada adiposidad abdominal en la edad pre-escolar.
ganancia de peso; adiposidad; pre-escolar
ORIGINAL ARTICLE
Association between weight gain in the first year of life with excess weight and abdominal adiposity at preschool age
Asociación entre ganancia de peso en el primer año de vida con exceso de peso y de adiposidad abdominal en la edad pre-escolar
Mariane Leite BertottoI; Júlia ValmórbidaII; Mônica Cristina BroiloIII; Paula Dal B. CampagnoloIV; Márcia Regina VitoloV
Instituição: Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA), Porto Alegre, RS, Brasil
INutricionista pela UFCSPA, Porto Alegre, RS, Brasil
IIMestranda pelo Programa de Pós-Graduação da UFCSPA, Porto Alegre, RS, Brasil
IIIDoutoranda pelo Programa de Pós-Graduação da UFCSPA, Porto Alegre, RS, Brasil
IVDoutora em Ciências da Saúde pela UFCSPA; Professora da Universidade do Vale do Rio dos Sinos e Coordenadora da Escola Superior de Saúde Unisinos Mãe de Deus, São Leopoldo, RS, Brasil
VDoutora em Ciências Biológicas pela Universidade Federal de São Paulo (Unifesp); Professora Adjunta do Departamento de Nutrição da UFCSPA, Porto Alegre, RS, Brasil
Endereço para correspondência
ABSTRACT
OBJECTIVE: To assess whether the change in body mass index Z-score for age >0.67 in the first year of life was associated with overweight at preschool age.
METHODS: A cohort study nested in a randomized field trial conducted in São Leopoldo, Rio Grande do Sul, Southern Brazil. Data on weight and height of children at birth, from six to eight, and from 12 to 16 months were collected. From ages three to four, besides these data, waist circumference was measured. Weight gain was calculated by the difference in body mass index/age Z-score from 12 to 16 months in relation to that at birth, adopting as cutoff >0.67 Z-score for weight gain. Waist-to-height ratio was calculated, and the excess of central adiposity was considered for values >0.5. Multivariate analysis to test the association between outcomes and independent variables was applied.
RESULTS: The prevalence of excessive weight gain in the first year of life was 29.5% out of the 338 studied children. After adjustment for gender, origin group, birth weight, duration of exclusive breastfeeding and mother's body mass index, the change in >0.67 Z-score from birth to 12 to 16 months was an independent risk factor for overweight (RR 2.81, 95%CI 1.535.16) and for elevated waist-to-height ratio (RR 2.10, 95%CI 1.193.72) in preschool age.
CONCLUSIONS: Excessive weight gain in the first year of life was associated with overweight and high abdominal adiposity at preschool age.
Key-words: weight gain; adiposity; child, preschool.
RESUMEN
OBJETIVO: Evaluar si el cambio en el escore Z del Índice de Masa Corporal (IMC) por edad >0,67 en el primer año de vida se asoció al exceso de peso en la edad pre-escolar.
MÉTODOS: Estudio de cohorte aunado a ensayo de campo aleatorio realizado en la ciudad de São Leopoldo (Rio Grande do Sul). Se recogieron datos de peso y estatura de los niños al nacer, 6 a 8 y 12 a 16 meses. A los 3 a 4 años de edad, se verificó también la circunferencia de la cintura. Se calculó la ganancia de peso por la diferencia en el escore Z de IMC/Edad a los 12 a 16 meses respecto al IMC/Edad al nacer, adoptando punto de corte >0,67 para ganancia de peso excesiva. Relación cintura/estatura fue realizada, considerando exceso de adiposidad central valores >0,5. Se utilizó el análisis multivariado para probar la asociación entre los desenlaces y las variables independientes.
RESULTADOS: La prevalencia de ganancia de peso excesiva en el primer año de vida fue de 29,5% de un total de 338 niños. Después del ajuste para las variables sexo, grupo, peso al nacer, tiempo de lactancia materna exclusiva e IMC de la madre, el cambio en el escore z >0,67 del nacimiento hasta los 12 a 16 meses se presentó como factor de riesgo para excesos de peso (RR 2,81; IC95% 1,535,16) y elevada relación cintura/altura en la edad pre-escolar (RR 2,10; IC95% 1,193,72).
CONCLUSIÓN: Ganancia de peso excesivo en el primer año de vida está asociada a exceso de peso y elevada adiposidad abdominal en la edad pre-escolar.
Palabras clave: ganancia de peso; adiposidad; pre-escolar.
Introduction
The nutritional profile of the population has changed in recent decades, with an increase in the prevalence of overweight and obesity, and a reduction in malnutrition rates, evident in adulthood and documented in childhood(1,2). International studies show variation in the prevalence of obesity in children and adolescents, with values between 7 and 19%(3-5). In Brazil, 33.5 and 14.3% of children from 5 to 9 years are overweight and obese, respectively(6).
Weight gain during the first years of life is a determining factor of nutritional status in childhood, and the association between rapid growth and obesity in children and adults has been reported in several studies(7-10). The high rate of weight gain is a major risk factor for chronic diseases such as type 2 diabetes, hypertension, dyslipidemia, and heart disease, morbidities present in adult life(11). Developing insulin resistance, sleep disorders, gastrointestinal diseases, and orthopedic syndromes are some complications that may be present in childhood(12-14).
According to the cutoff point >0.67 in BMI/age z score, weight gain in the first years of life may be associated with risk factors for the development of diseases in different stages of life(15). This cutoff point has been used for the calculation of weight gain from birth to six months old, or even from birth to 12 months, compared with body composition at preschool, school and adolescent lives(16). Other outcomes related to the z score >0.67 of BMI/Age are resistance to insulin, cardiovascular risk, age at menarche, adiposity and lipid fractions(15-17).
Thus, studies have shown that accelerated growth in early life is associated with obesity in adulthood, which is a determining factor for future metabolic complications(8). Thus, the objective of this research was to test the hypothesis that a BMI/Age z score greater than 0.67 in the first year of life is associated with overweight in preschool life.
Method
The study consisted of a cohort study nested in a randomized field trial with children aged 34 years, monitored from birth at Hospital Centenário, the only one in the municipality of São Leopoldo, between October, 2001 and July, 2002. The sample size calculation was based on the primary goal of a larger study, which aimed to increase the frequency of exclusive breastfeeding until 4 months. We used the rate of exclusive breastfeeding at this age of 21.6% in the control group and estimated a difference of 65.0% in the frequency of this practice among the groups, after the intervention. Other parameters for this calculation were: power of 80.0% and confidence level of 95.0%, which resulted in a sample size of 177 children in each group, totaling 354 children. Considering estimated losses of 25.0%, 500 pairs of mother-child were recruited for the sample size to be reached.
The mother-infant pairs were recruited at birth. Mothers were informed of the procedures of the study and, after signing the Consent Form, pairs were randomized into intervention and control groups. The intervention involved dietary guidelines based on the program of the Brazilian Ministry of Health, entitled "Dez passos para alimentação saudável para crianças menores de dois anos"(18). This was done through home visits, which occurred in a monthly basis throughout the first 6 months and bi-monthly until 12 months.
The data collection team, composed of graduate students in Nutrition, was previously qualified to data collection. The training aimed to educate the group about the protocols that would be used to perform anthropometry and the administration of the questionnaires, based on the Manual of Data Collection designed specifically for this study. All team members of data collection were blinded regarding the group to which the mother-child pairs belonged.
Data collection began on maternity care, shortly after birth, and later during home visits in three moments: at 68 months, at 1216 months, and at 34 years of age. At birth, we obtained length and weight of the child. The study included only infants with gestational age >37 weeks and birth weight ≥2,500g. At 6 to 8 months, we measured anthropometric data of the mother and obtained socioeconomic and demographic data through a questionnaire prepared for the study. Weight was measured with the mother barefoot, wearing light clothes, in a digital scale (Techline®, São Paulo, Brasil). Height was measured with the mother standing, positioned upright, heels touching the wall, using a Seca® portable stadiometer, with accuracy of 0.1cm, fixed in smooth wall.
Regarding anthropometric data of children, between 1216 months, the anthropometric measurements consisted of weight and length. Weight was measured on a digital scale (Techline®, São Paulo, Brazil) with the child barefoot, without clothes or diapers. The child was weighed on his mother's lap, with subsequent subtraction of mother's weight. The child's length was measured in supine position using a wooden pediatric stadiometer (Serwital Inc, Porto Alegre, Brazil). At 3 and 4 years old, anthropometric measurements included the circumference of the waist. Weight was measured with the child wearing light clothing and barefoot on the same scale used at 12 to 16 months. Height was measured with the child standing, positioned upright, heels touching the wall, with the aid of a Seca® portable stadiometer, with accuracy of 0.1cm, fixed in smooth wall. Waist circumference was measured with an inextensible tape measure, in the smallest circumference between the costal margin and the iliac crest.
Body Mass Index (BMI) was calculated using measurements of weight and height, at birth and at 3 to 4 years old. Weight gain in the 1st year of life was obtained using the difference in BMI z score at 1216 months in relation to BMI z score at birth, according to the criteria of the World Health Organization(19)(WHO). The cutoff point used for classification of weight gain in the first year of life was the one by Ong et al(8), and z score of BMI ≤0.67 was considered adequate and >0.67 considered as excessive weight gain. At 34 years of age, the z score of the BMI/Age was calculated and cutoff points of >1 for overweight and >2 for obesity were used. With the values of waist circumference and height, we calculated the waist/height ratio. This index has been used in the determination of risk factors for cardiovascular diseases, being attributed a cutoff of 0.5 for the classification of this ratio, considering values higher than this as abdominal adiposity(20). Maternal BMI was calculated using data from the anthropometric assessment performed at 6 to 8 months. Maternal nutritional status was considered adequate when BMI <25kg/m2 and overweight when ≥25kg/m2.
Data were subjected to double entry in the Statistical Package for Social Sciences version 16.0 (SPSS Inc., Chicago, USA) and validated using the Epi-Info version 6.4 (CDC, Atlanta, USA). Statistical analyses were performed in the SPSS 16.0 Software. Frequency analyses were performed to describe categorical variables, and mean and standard deviation for continuous variables. The association between the variables of gender, group, birth weight, exclusive breastfeeding, maternal BMI and change in BMI/Age z score at 12 to 16 months regarding the outcome was performed by means of multivariate analysis. The sample size in each analysis differed according to data availability. A significance level of 5% (p<0.05) was adopted, for a confidence interval of 95% (95%CI).
The project was approved by the Research Ethics Committee of Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA). Mothers who accepted to participate in the research signed the Informed Consent Form and were informed about the procedures involved in the study. Children with unfavorable clinical situations were referred to health services for treatment.
Results
In the initial phase of the study, information was collected from 500 mother-child pairs. In the later stages of data collection, 397 and 354 pairs participated at 12 to 16 months and at 3 to 4 years, respectively. Losses that occurred in the initial phase were due to parental refusal to continue follow-up, followed by change of address. Among children assessed in both phases, 16 were excluded due to insufficient data for the calculation of BMI/Age at 12 to 16 months or at 3 to 4 years, totaling a final sample of 338 children.
The socioeconomic and demographic characteristics of the children's families were obtained only in one moment of data collection, when the child was 6 months old. Among the 338 children who participated in the analyses of this study, it was observed that 18.4% of mothers were aged under 20 years and 55.8% had less than 8 years of education. Family income, expressed as the minimum wages prevailing at the time of data collection, showed that 69.9% of families lived with less than 3 minimum wages and that 61.8% of mothers did not have a paid activity.
The prevalence of excessive weight gain in the 1st year of life was 29.5%. Regarding BMI, at 12 to 16 months 34.2% presented overweight and 9.4% presented obesity. At 3 and 4 years 20.9% of children were classified as overweight and 5.5% as obese.
Table 1 presents the variables associated with BMI/Age at 3 to 4 years old. There was no significant difference regarding sex, group, birth weight, duration of breastfeeding, and maternal BMI. Regarding weight gain, children with a change of >0.67 in the BMI/Age z score, presented 2.81-fold higher chances of having excess weight in preschool in comparison to those whose variation in BMI/Age z score was lower than the cutoff point used in this study.
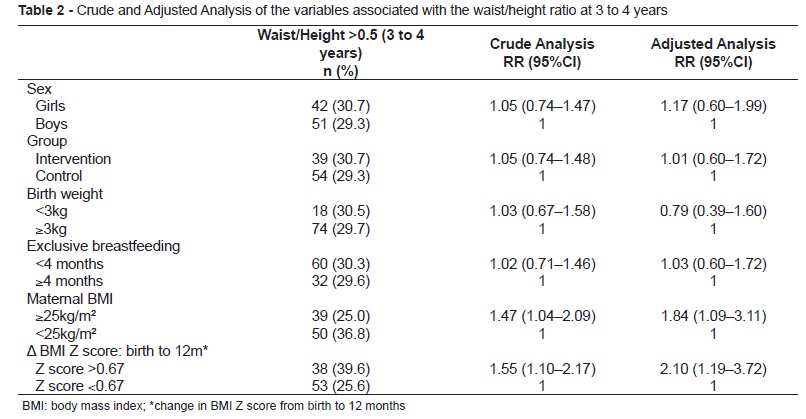
Variables associated with waist/height are described in Table 2. Regarding the change in BMI/Age z score >0.67, children with excessive weigh gain in the 1st year of life presented a 2.10-fold higher risk of developing abdominal adiposity when compared to those who had changes in the BMI/Age z score <0.67. Children whose mothers had BMI ≥25kg/m2 presented 1.84-fold higher risk for abdominal adiposity than those whose mothers did not have excess weight. The other variables were not significant in relation to the outcome.
Discussion
The first years of life are a critical period for the development of obesity, considered a risk factor for chronic diseases, in special cardiovascular disease, due to the intense growth speed(21,22). The present study showed a prevalence of excessive weight gain of approximately 30% in the 1st year of life, similar to previous studies that indicated prevalence of 25.4% excess weight in the 1st months(16) and 30.7% in the 2 first years of life(8). A systematic review regarding the determinants of overweight and obesity in early life stressed that accelerated weight gain in this phase has an important influence on nutritional status in childhood, with a consistent association with increased risk of obesity(23). Although the present study has evaluated the change in BMI/Age z score from birth to 16 months, the highest prevalence of children assessed at 12 months allows the results to be discussed regarding the 1st year of life.
Recent data from the Household Budget Survey (HBS 2008/2009) documented that 32.8% of children presented excess weight and 16.2%, obesity, at 5 years old(6). The present study found just over 20% of children classified as overweight and 5.5% as obese, but the age of these children is in a lower range compared to the HBS, showing that the children in our sample probably have not yet been through the period of adiposity rebound, which starts around 5 to 7 years of age, which may explain the lower percentages in this population(24).
This study demonstrated that the risk of presenting excess weigh at 3 to 4 years was nearly three times higher among children with excessive weight gain. Ong et al indicated that children with high growth rate during the first 9 months of life present 48% higher risk of obesity at 10 years old(17). A prospective cohort study conducted in Stockholm showed that excessive weight gain during the first 6 months is a predictor of adolescent obesity and cardiometabolic risk(16). These authors pointed out that several factors act as predictors of accelerated weight gain, including the duration of exclusive breastfeeding and the early and inappropriate introduction of complementary foods(16,17,25).
According to data of Corvalan et al, in a study that aimed to assess the relationship between weight gain in the period of 0 to 4 years and the condition of cardiovascular disease at age 4 in Chilean children with normal birth weight, changes in BMI in all periods analyzed (at birth, 6, 12, 18, 24, 36 and 48 months) were positively associated with higher metabolic score at 4 years old, with the strongest association within 6 to 24 months(22). Authors suggest this period as critical for the development of future obesity as well as related metabolic complications, suggesting prevention measures(22,26).
This study demonstrated that the greatest weight gain in the first year of life was associated with a 2.10 times greater risk of developing abdominal adiposity. Ong et al reported that children with change in BMI/Age z score >0.67 in the first two years of life, developed higher abdominal adiposity at 5 years old, compared to those without excessive weigh gain in the first year. These authors emphasized that these children, at birth, were smaller and slimmer compared to others, suggesting a possible role of a postnatal compensatory mechanism due to intra-uterine growth restriction(8). However, it is important to mention that low birth weight was considered an exclusion criterion in the present study.
Freedman et al, using the same indicators of this study, studied the relationship of BMI/Age z score and waist/height ratio with risk factors for cardiovascular diseases in children and adolescents, demonstrating that both indicators were strongly associated with these factors. Abdominal adiposity correlated with the total cholesterol /HDL-cholesterol ratio and with LDL-cholesterol levels, while BMI showed association with fasting insulin concentration(27). A similar study, conducted in the municipality of Belo Horizonte with children and adolescents, showed that excess weight and body fat distribution in the trunk, along with physical inactivity, were associated with high levels of blood pressure, total cholesterol, LDL-C, as well as with decreased levels of HDL-C(28).
Another association regarding the waist/height ratio was the 1.84-fold greater risk of excess abdominal adiposity in children whose mothers had a BMI≥25kg/m2. There is evidence of the influence of family nutritional status on body composition of children(29). Several factors may be involved in determining obesity, among which the genetic contribution, that, according to some authors, may explain from 20 to 90% of weight heredity(23).
This study did not access the level of physical activity of children in the sample, which can be considered a limitation, because the association between obesity and this practice has been previously demonstrated(30). However, there are no validated protocols for measuring the degree of physical activity in this age, limiting, thus, the reliability of data. It is important to highlight that the influence of low birth weight on the development of obesity and abdominal adiposity could not be investigated in this study, since the randomization included only children with birth weight ≥2,500g. Another limitation refers to the study design and sample size, which were not designed for the primary purpose of the analysis presented in this study, but to the main research that evaluated the impact of an intervention on the eating habits of children.
In this study, the change in BMI/Age z score >0.67 in the first year of life was associated with excess weight, as well as with the presence of abdominal adiposity in preschool, confirming the initial hypothesis of the study. According to Victora et al(31), the two first years of life constitute the window of opportunity to promote the healthy growth of children through appropriate feeding practices, such as longer duration of breastfeeding and healthy complementary feeding.
References
- 1. Martins EB, Carvalho MS. Birth weight and overweight in childhood: a systematic review. Cad Saude Publica 2006;22:2281-300.
- 2. Santos AL, Leão LS. Anthropometric profile of preschool children of a day-care center in Duque de Caxias, Rio de Janeiro, Brazil. Rev Paul Pediatr 2008;26:218-24.
- 3. Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007-2008. JAMA 2010;303:242-9.
- 4. Moraes SA, Beltrán Rosas J, Mondini L, Freitas IC. Prevalence of overweight and obesity, and associated factors in school children from urban area in Chilpancingo, Guerrero, Mexico, 2004. Cad Saude Publica 2006;22:1289-301.
- 5. Branca F, Nikogosian H, Lobstein T. The challenge of obesity in the WHO European region and the strategies for response. Copenhagen: World Health Organization; 2007.
-
6Brasil. Ministério do Planejamento, Orçamento e Gestão, Instituto Brasileiro de Geografia e Estatística. Pesquisa de Orçamentos Familiares 2008-2009: antropometria e estado nutricional de crianças, adolescentes e adultos no Brasil. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2010.
- 7. Stettler N, Kumanyika SK, Katz SH, Zemel BS, Stallings VA. Rapid weight gain during infancy and obesity in young adulthood in a cohort of African Americans. Am J Clin Nutr 2003;77:1374-8.
- 8. Ong KK, Ahmed ML, Emmett PM, Preece MA, Dunger DB. Association between postnatal catch-up growth and obesity in childhood: prospective cohort study. BMJ 2000;320:967-71.
- 9. Baird J, Fisher D, Lucas P, Kleijnen J, Roberts H, Law C. Being big or growing fast: systematic review of size and growth in infancy and later obesity. BMJ 2005;331:929.
- 10. Monteiro PO, Victora CG. Rapid growth in infancy and childhood and obesity in later life - a systematic review. Obes Rev 2005;6:143-54.
- 11. Barker DJ, Osmond C, Kajantie E, Eriksson JG. Growth and chronic disease: findings in the Helsinki Birth Cohort. Ann Hum Biol 2009;36:445-8.
- 12. Taveras EM, Rifas-Shiman SL, Belfort MB, Kleinman KP, Oken E, Gilmann MW. Weight status in the first 6 months of life and obesity at 3 years of age. Pediatrics 2009;123:1177-83.
- 13. Shibli R, Rubin L, Akons H, Shaoul R. Morbidity of overweight (>or=85th percentile) in the first 2 years of life. Pediatrics 2008;122;267-72.
- 14. Abrams P, Levitt Katz LE. Metabolic effects of obesity causing disease in childhood. Curr Opin Endocrinol Diabetes Obes 2011;18:23-7.
- 15. Mamabolo RL, Alberts M, Steyn NP, Delemarre-van de Waal HA, Levitt NS. Prevalence and determinants of stunting and overweight in 3-year-old black South African children residing in the Central Region of Limpopo Province, South Africa. Public Health Nutr 2005;8;501-8.
- 16. Ekelund U, Ong K, Linné Y, Neovius M, Brage S, Dunger DB et al Upward weight percentile crossing in infancy and early childhood independently predicts fat mass in young adults: the Stockolm Weight Development Study (SWEDES). Am J Clin Nutr 2006;83:324-30.
- 17. Ong KK, Emmett P, Northstone K, Golding J, Rogers I, Ness AR et al Infancy weight gain predicts childhood body fat and age at menarche in girls. J Clin Endocrinol Metab 2009;94:1527-32.
-
18Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção à Saúde. Dez passos para uma alimentação saudável: guia alimentar para crianças menores de dois anos - um guia para o profissional da saúde na atenção básica. [Série A. Normas e Manuais Técnicos] Brasília: Ministério da Saúde; 2002.
-
19World Health Organization. WHO child growth standards - methods and development: length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age. Geneva: WHO; 2006.
- 20. McCarthy HD, Ashwell M. A study of central fatness using waist-to-height ratios in UK children and adolescents over two decades supports the simple message - 'Keep your waist circumference to less than half your height'. Int J Obes (Lond) 2006;30;988-92.
- 21. González DA, Nazmi A, Victora CG. Growth from birth to adulthood and abdominal obesity in a Brazilian birth cohort. Int J Obes (Lond) 2010;34:195-202.
- 22. Corvalán C, Uauy R, Stein AD, Kain J, Martorell R. Effect of growth on cardiometabolic status at 4 y of age. Am J Clin Nutr 2009;90:547-55.
- 23. Monasta L, Batty GD, Cattaneo A, Lutje V, Ronfani L, Van Lenthe FJ et al Early-life determinants of overweight and obesity: a review of systematic reviews. Obes Rev 2010;11:695-708.
- 24. Dietz WH. Critical periods in childhood for the development of obesity. Am J Clin Nutr 1994;59:955-9.
- 25. Baker JL, Michaelsen KF, Rasmussen KM, Sorensen TI. Maternal prepregnant body mass index, duration of breastfeeding, and timing of complementary food introduction are associated with infant weight gain. Am J Clin Nutr 2004;80:1579-88.
- 26. Ong KK, Loos RJ. Rapid infancy weight gain and subsequent obesity: systematic reviews and hopeful suggestions. Acta Paediatr 2006;95:904-8.
- 27. Freedman DS, Kahn HS, Mei Z, Grummer-Strawn LM, Dietz WH, Srinivasan SR et al Relation of body mass index and waist-to-height ratio to cardiovascular disease risk factors in children and adolescents: the Bogalusa Heart Study. Am J Clin Nutr 2007;86:33-40.
- 28. Ribeiro RQ, Lotufo PA, Lamounier JA, Oliveira RG, Soares JF, Botter DA. Additional cardiovascular risk factors associated with excesso weigth in children and adolescents. The Belo Horizonte Heart Study. Arq Bras Cardiol 2006;86:408-18.
- 29. Monteiro PO, Victora CG, Barros FC, Monteiro LM. Birth size, early childhood growth, and adolescent obesity in a Brazilian birth cohort. Int J Obes Relat Metab Disord 2003;27:1274-82.
- 30. Ortega FB, Ruiz JR, Sjöström M. Physical activity, overweight and central adiposity in Swedish children and adolescents: the European Youth Heart Study. Int J Behavioral Nutr Phys Act 2007;4:61.
- 31. Victora CG, de Onis M, Hallal PC, Blössner M, Shrimpton R. Worldwide timing of growth faltering: revisiting implications for interventions. Pediatrics 2010;125:e473-80.
Endereço para correspondência:
Publication Dates
-
Publication in this collection
04 Jan 2013 -
Date of issue
Dec 2012
History
-
Received
09 Feb 2012 -
Accepted
11 June 2012