Abstract
INTRODUCTION: his study evaluated the consumption of major classes of antibiotics, the colonization of the oropharynx of patients on mechanical ventilation, and the risk of ventilator-associated pneumonia (VAP) caused by Staphylococcus aureus in an intensive care unit for adults. METHODS: A case-control study was carried out using colonized patients (cases) by oxacillin-resistant S. aureus (ORSA) and (controls) oxacillin-sensitive S. aureus (OSSA) from May 2009 to August 2010. The occurrence of VAP by S. aureus was also evaluated in the same period. Antibiotic consumption was expressed as the number of defined daily doses (DDD)/1,000 patient-days for glycopeptides, carbapenems, and extended-spectrum cephalosporins. RESULTS: Three hundred forty-six (56.1%) patients underwent mechanical ventilation with a frequency of oropharyngeal colonization of 36.4%, corresponding to 63.5% for ORSA and 36.5% for OSSA. The risk of illness for this organism was significant (p<0.05), regardless of whether colonization/infection was by ORSA or OSSA. The consumption of antibiotics was high, mainly for broad-spectrum cephalosporins (551.26 DDDs/1,000 patient-days). The high density of use of glycopeptides (269.56 DDDs/1,000 patient-days) was related to colonization by ORSA (Pearson r=0.57/p=0.02). Additionally, age >60 years, previous antibiotic therapy, and previous use of carbapenems were statistically significant by multivariate analysis. CONCLUSIONS: There was a significant relationship between the colonization of the oropharyngeal mucosa and the risk of VAP by both phenotypes. The use of glycopeptides was related to colonization by ORSA.
Staphylococcus aureus; Oropharyngeal colonization; VAP; Antibiotic consumption
Resumo
INTRODUÇÃO: Este estudo avaliou o consumo das principais classes de antibióticos, a colonização de orofaringe de pacientes sob ventilação mecânica e o risco de pneumonia associada à ventilação (PAV) causada por Staphylococcus aureus em uma unidade de terapia intensiva (UTI) de adultos. MÉTODOS: Foi realizado um estudo caso-controle, sendo caso os pacientes colonizados pelo oxacillin-resistant Staphylococcus aureus (ORSA), e controle aqueles pelo oxacillin-sensitive Staphylococcus aureus (OSSA), no período de maio de 2009 a agosto de 2010. A ocorrência de PAVs por S. aureus também foi avaliada no mesmo período. O consumo de antibióticos foi expresso pelo número de doses diárias definidas (DDDs)/1.000 pacientes-dia para glicopeptídeos, carbapenêmicos e cefalosporinas de amplo espectro. RESULTADOS: Trezentos e quarenta e seis (56,1%) dos pacientes foram submetidos à ventilação mecânica com uma frequência de colonização de orofaringe de 36,4%, correspondendo a 63,5% e 36,5% de ORSA e OSSA, respectivamente. O risco de adoecimento por este microrganismo foi significativo (p<0,05), considerando se a colonização/infecção foi por ORSA ou OSSA. O consumo de antibióticos foi alto, principalmente para cefalosporinas de amplo espectro (551,26 DDDs/1.000 pacientes-dia). A elevada densidade de uso de glicopetídeos (269,56 DDDs/1.000) foi relacionada com a colonização pelo ORSA (Pearson r=0.57/p=0.02). Adicionalmente, idade > 60 anos, terapia antibiótica prévia e uso prévio de carbapenêmicos foram estatisticamente significantes por análise multivariada. CONCLUSÕES: Foi observada uma relação significativa entre a colonização da mucosa de orofaringe e o risco de PAV por ambos fenótipos. O uso de glicopeptídos foi relacionado com a colonização pelo ORSA.
Staphylococcus aureus; Colonização de orofaringe; PAV; Consumo de antibióticos
ARTICLE ARTIGO
Relationship between antibiotic consumption, oropharyngeal colonization, and ventilator-associated pneumonia by Staphylococcus aureus in an intensive care unit of a Brazilian teaching hospital
Relação entre consumo de antibióticos, colonização de orofaringe e pneumonia associada à ventilação por Staphylococcus aureus em um hospital de ensino brasileiro
Michel Rodrigues Moreira; Paulo Pinto Gontijo Filho
Laboratório de Microbiologia, Instituto de Ciências Biomédicas, Universidade Federal de Uberlândia, Uberlândia, MG
ABSTRACT
INTRODUCTION: his study evaluated the consumption of major classes of antibiotics, the colonization of the oropharynx of patients on mechanical ventilation, and the risk of ventilator-associated pneumonia (VAP) caused by Staphylococcus aureus in an intensive care unit for adults.
METHODS: A case-control study was carried out using colonized patients (cases) by oxacillin-resistant S. aureus (ORSA) and (controls) oxacillin-sensitive S. aureus (OSSA) from May 2009 to August 2010. The occurrence of VAP by S. aureus was also evaluated in the same period. Antibiotic consumption was expressed as the number of defined daily doses (DDD)/1,000 patient-days for glycopeptides, carbapenems, and extended-spectrum cephalosporins.
RESULTS: Three hundred forty-six (56.1%) patients underwent mechanical ventilation with a frequency of oropharyngeal colonization of 36.4%, corresponding to 63.5% for ORSA and 36.5% for OSSA. The risk of illness for this organism was significant (p<0.05), regardless of whether colonization/infection was by ORSA or OSSA. The consumption of antibiotics was high, mainly for broad-spectrum cephalosporins (551.26 DDDs/1,000 patient-days). The high density of use of glycopeptides (269.56 DDDs/1,000 patient-days) was related to colonization by ORSA (Pearson r=0.57/p=0.02). Additionally, age >60 years, previous antibiotic therapy, and previous use of carbapenems were statistically significant by multivariate analysis.
CONCLUSIONS: There was a significant relationship between the colonization of the oropharyngeal mucosa and the risk of VAP by both phenotypes. The use of glycopeptides was related to colonization by ORSA.
Keywords:Staphylococcus aureus. Oropharyngeal colonization. VAP. Antibiotic consumption.
RESUMO
INTRODUÇÃO: Este estudo avaliou o consumo das principais classes de antibióticos, a colonização de orofaringe de pacientes sob ventilação mecânica e o risco de pneumonia associada à ventilação (PAV) causada por Staphylococcus aureus em uma unidade de terapia intensiva (UTI) de adultos.
MÉTODOS: Foi realizado um estudo caso-controle, sendo caso os pacientes colonizados pelo oxacillin-resistant Staphylococcus aureus (ORSA), e controle aqueles pelo oxacillin-sensitive Staphylococcus aureus (OSSA), no período de maio de 2009 a agosto de 2010. A ocorrência de PAVs por S. aureus também foi avaliada no mesmo período. O consumo de antibióticos foi expresso pelo número de doses diárias definidas (DDDs)/1.000 pacientes-dia para glicopeptídeos, carbapenêmicos e cefalosporinas de amplo espectro.
RESULTADOS: Trezentos e quarenta e seis (56,1%) dos pacientes foram submetidos à ventilação mecânica com uma frequência de colonização de orofaringe de 36,4%, correspondendo a 63,5% e 36,5% de ORSA e OSSA, respectivamente. O risco de adoecimento por este microrganismo foi significativo (p<0,05), considerando se a colonização/infecção foi por ORSA ou OSSA. O consumo de antibióticos foi alto, principalmente para cefalosporinas de amplo espectro (551,26 DDDs/1.000 pacientes-dia). A elevada densidade de uso de glicopetídeos (269,56 DDDs/1.000) foi relacionada com a colonização pelo ORSA (Pearson r=0.57/p=0.02). Adicionalmente, idade > 60 anos, terapia antibiótica prévia e uso prévio de carbapenêmicos foram estatisticamente significantes por análise multivariada.
CONCLUSÕES: Foi observada uma relação significativa entre a colonização da mucosa de orofaringe e o risco de PAV por ambos fenótipos. O uso de glicopeptídos foi relacionado com a colonização pelo ORSA.
Palavras-chaves:Staphylococcus aureus. Colonização de orofaringe. PAV. Consumo de antibióticos.
INTRODUCTION
Nosocomial infections pose a significant threat to patients worldwide, and antibiotic-resistant bacteria are related to a greater impact on morbidity/mortality and the costs of such infections1-3. Ventilator-associated pneumonia (VAP) is the most frequent infection acquired in the intensive care unit (ICU), occurring in 9% to 24% of patients intubated for longer than 48h4,5. It is associated with increased morbidity, prolonged hospitalization, and increased healthcare costs58.
Each antibiotic prescription has an environmental and ecological consequence9,10. Many case-control studies demonstrate prior antibiotic exposure, particularly with cephalosporins and fluoroquinolones, as a risk factor for both oxacillin-resistant Staphylococcus aureus (ORSA) colonization and infection2,10. Antibiotics such as fluoroquinolones and cephalosporins are well known to increase the expression of fibronectin adhesions, facilitating adherence and ability to colonize, and many other virulence factors such as toxins that might cause colonization and develop into infection10-12.
Increased numbers of ORSA were demonstrated in the noses of carriers receiving fluoroquinolones or β-lactams compared with controls13. Presumably this is due to a competitive advantage achieved by antibiotic administration, ablating the normal protective commensal flora, including oxacillin-sensitive S. aureus (OSSA), allowing multiplication of the ORSA with increased potential for contaminating the environment10.
The aim of this study was to evaluate the consumption of major classes of antibiotics, the colonization of the oropharynx of patients on mechanical ventilation (MV), and the risk of VAP caused by S. aureus susceptible or resistant to oxacillin, as well as other risk factors in patients in an adult mixed ICU from a Brazilian university hospital.
METHODS
Setting
The Uberlândia Federal University-Hospital Clinic (UFU-HC) is a teaching hospital with 500 beds and a clinical-surgical ICU for adults with 15 beds.
Study design
A case-control study was carried out using colonized patients by ORSA (case) and OSSA (control) from May 2009 to August 2010, when 617 patients were admitted. The cultures of oropharyngeal secretions were taken at baseline (< 24h in the ICU) and every 2 days until the confirmation of colonization or discharge. In the same period the occurrence of VAPs by S. aureus was also evaluated.
The patients with VAP were under MV for a period >48h after being admitted to the ICU, with new and/or progressive radiological infiltrate and experiencing at least two of the following conditions: purulent sputum, temperature higher than 38.5ºC or lower than 35ºC, and leukocyte count higher than 10,000/µL with deviation to the left or lower than 3,000/µL; and positive quantitative culture of the endotracheal aspirate (count >106 CFU/ml)14-16.
Antibiotic consumption was expressed as the number of defined daily doses (DDD)/1,000 patient-days for the following classes: glycopeptides (vancomycin and teicoplanin), carbapenems (imipenem, meropenem, and ertapenem), and extended-spectrum cephalosporins (ceftriaxone and cefepime).
Additionally, the following patient data were collected: age, gender, invasive procedures, admission diagnosis, previous use of antibiotics and corticoids, hospitalization, and MV times.
Microbiological techniques
The collection of clinical specimen obtained from the oropharynx was made with a swab, and the specimen was transported in sterile tube with 1ml of trypticase soy broth supplemented with 6.5% NaCl. Endotracheal aspirate was collected by probe n 12 early in the morning by the health professionals (physiotherapists and nurses) in charge of the procedure, and was transported in a sterile tube to the Microbiology Laboratory of UFU. Oropharynx and endotracheal aspirate samples were cultivated in salty mannitol agar (Biobrás, Brazil) by qualitative and quantitative techniques, respectively. The S. aureus isolates were identified by mannitol fermentation, Gram stain, and catalase, free coagulase, and bond coagulase tests. Resistance to oxacillin was detected by means of a screening test in salty mannitol agar (Biobrás, Brazil) incorporated with 6µg/ml of oxacillin and 4.5% of NaCl.
Statistical analysis
Univariate comparisons were carried out using the Qui-Square (X2) and Fisher's exact tests. Multivariate analysis was carried out by simple or multiple logistic regression when appropriate, and the values were included when significance was <0.25 in univariate analysis or in case of clinical relevance. Pearson's correlation coefficient was used to determine the relationship between antibiotic consumption and trends in resistance. The results were considered statistically significant at a level of 5%. The epidemiological data were analyzed through the programs Epi-Info version 5.017, GraphPad prism 3.018, and BioEstat 5.019.
Ethical considerations
The Ethics Committee for Human Research of UFU approved the project.RESULTSFrom May 2009 to August 2010 a total of 617 adult patients were admitted to the adult ICU of the UFU-HC. Three hundred forty-six (56.1%) patients who were submitted to MV. All these patients were surveyed, and 126 (36.4%) were colonized in the oropharynx with S. aureus; 63.5% were ORSA and 36.5% were OSSA, corresponding to 10.97 ± 6.67 and 6.26 ± 4.49 colonizations/1,000 patient-days for these microorganisms, respectively. Among the 320 (51.9%) patients submitted to MV for longer than 48h, VAP was diagnosed in 81 (25.3%) patients, the main agents being represented by Pseudomonas aeruginosa and Acinetobacter baumannii.
Although high frequencies of colonization of the mucous membranes of the oropharynx by S. aureus (126/346; 36.4%), ORSA (80/346; 23.1%), and OSSA (46/346; 13.3%) were found, the participation of these microorganisms in VAPs was low at 11 (13.6%) of 81, 4 (4.9%)of 81, and 7 (8.6%) of 81, respectively.
The risk of illness in patients colonized in oropharynx was 7 (5.5%) of 126, 4 (5%) of 80, and 3 (6.5%)of 46 for S. aureus, ORSA, and OSSA, respectively. Four patients had episodes of VAP (4 OSSA) without previous colonization by this microorganism. The risk of pneumonia was significant (p < 0.05) by univariate analysis, regardless of whether colonization/infection was by ORSA or OSSA (Table 1).
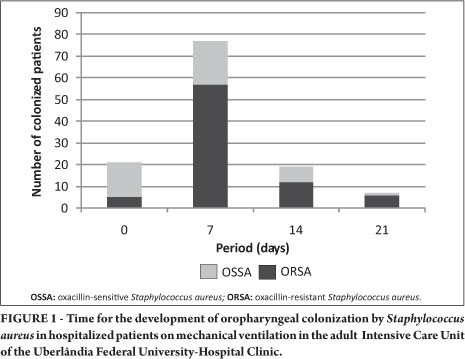
The average time to colonization was slightly longer for ORSA (5.8 days) than for OSSA (5.0 days) (Table 2). Oropharyngeal colonization was associated with the length of stay in the ICU (p = 0.0001), with rates of 93.7% (75/80 patients) for ORSA and 65.2% (30/46 patients) for OSSA, from the first week in the unit (Figure 1); 6.3% (5/80) and 34.8% (16/46) of patients were admitted to the ICU with ORSA and OSSA, respectively.
The consumption of antibiotics was high, mainly for broad-spectrum cephalosporins (551.26 DDDs/1,000 patient-days). The high density of use of glycopeptides (269.56 DDDs/1,000 patient-days) was related to colonization by ORSA (Pearson r = 0.57/p = 0.02) (Figure 2). Additionally, age >60 years (p = 0.04), previous antibiotic therapy (p = 0.04), and previous use of carbapenems (p = 0.03) were statistically significant by univariate and multivariate analysis (Tables 2 and 3).
DISCUSSION
Staphylococcus aureus was colonizing the oropharynx in 36.4% of patients undergoing MV at the ICU of the UFU-HC, with 63.5% corresponding to ORSA and 36.5% to OSSA. The colonization of mucous membranes of the upper respiratory tract with potentially pathogenic microorganisms is particularly common in critically ill patients, especially those with decreased level of consciousness, which occurs frequently in ICUs20. For these patients, especially in the ICU, the normal microbiota undergoes drastic changes due to the use of antibiotics21,22 and the action of proteases that decrease immunoglobulin and fibronectin present in the mucosa, preventing the adherence of microorganisms of the normal microbiota, favoring Gram-negative bacilli and S. aureus22,23.
Oropharyngeal and tracheal colonization plays a central role in the pathogenesis of VAP16,24. In studies of intensive-care patients, ORSA colonizes the throat more frequently than it does either the nose or the groin/axilla25-28, and nasal colonization with ORSA is a poor predictor for the subsequent occurrence of ORSA lower respiratory tract infections that require antimicrobial treatment29. On the other hand, there is less information on the etiopathogenesis for the development of VAP by ORSA. DNA genomic analysis demonstrated that an identical strain was isolated from oropharyngeal or gastric samples and bronchial samples in all but three cases of pneumonia, due to S. aureus30,31. In our study 5.5% of patients colonized by S. aureus developed VAP as opposed to just 1.8% of patients not colonized (p > 0.05), and among individuals colonized by phenotypes ORSA and OSSA, 5% and 6.5% developed VAP, respectively, as opposed to just 0% and 1.3% (p = 0.003/p = 0.05) of patients not colonized for these phenotypes, respectively. However, S. aureus was isolated in only 13.6% of episodes of VAP, the main agents being represented by Pseudomonas aeruginosa and Acinetobacter baumannii.
In a recent multi-centric study including 1,290 patients infected in the ICUs of hospitals in South and Central America, accounting for 60.3% of inpatients, pneumonia accounted for most (66%), predominated (70.9%) by Gram-negative bacteria, while ORSA accounted for just 10.4%32. Recent data from the European Antimicrobial Resistance Surveillance Network show that six countries reported decreasing trends in the proportion of ORSA among S. aureus isolates from invasive infections for the period 2006-2009. This is likely due to sustained efforts to contain the spread of ORSA in hospitals and other healthcare facilities33. In three ICUs in France the acquisition of ORSA was reduced from 7% to 3% through multiple interventions, including active surveillance cultures, contact precautions, and the use of alcohol hand hub34,35. In other regions/countries, however, S. aureus, particularly ORSA, remains endemic in larger hospitals as a major cause of bloodstream infections and pneumonia32,36,37. In this investigation, their participation in VAPs was small compared with that of Gram-negative bacilli, although the rates of oropharyngeal colonization are significant, representing a potential risk for developing this infection.
With a hospital stay of 5 days or longer, the patient is at greater risk of acquiring more resistant pathogens, and empirical treatment with broad-spectrum antimicrobial agents should be prescribed38. In our study, the mean time to colonization was 5.8 for ORSA and 5.0 for OSSA, and oropharyngeal colonization occurred in 93.7% of patients with ORSA and 65.2% with OSSA, from the first week in the unit.
Antibiotic pressure has been described as a risk factor for the acquisition of ORSA39-41, and the use of antibiotics during and prior to hospitalization in ICU has been shown to increase the number of ORSA infections41-44. Our results show an increased risk of acquiring ORSA if antibiotics are administered prior and during hospitalization in ICU (p < 0.05). A meta-analysis has shown that subjects who have been exposed to antibiotic therapy have an almost 2-fold chance of acquiring ORSA as opposed to non-exposed subjects. This risk is almost three times greater after the use of fluoroquinolones and glycopeptides beyond the cephalosporins2. Aldeyab et al.45 built a multivariate ARIMA model (time series analysis) to relate ORSA incidence with antibiotic usage. Retrospective analysis of a 5-year data set showed that temporal variation in ORSA incidence followed temporal variations in the use of fluoroquinolones, broad-spectrum cephalosporins, macrolides, and amoxicillin/clavulanic acid. In our study the use of antibiotics was high compared with that in American and European studies46,47, mainly for broad-spectrum cephalosporins, with higher recovery of ORSA; however, the high density of use of glycopeptides in the ICU was significantly related to the acquisition of the multidrug-resistant phenotype by patients, as well as previous use of carbapenems. In addition, patients who had prior use of fluoroquinolones were two times more likely to acquire ORSA (p > 0.05). The need to improve antibiotic prescribing in hospitals worldwide is urgent. Guidelines from the Society of Hospital Epidemiologists of America and the Infectious Diseases Society of America strongly support the wide diffusion of antibiotic stewardship programs in healthcare settings48,49. Changing hospital antibiotic use is a challenge of formidable complexity. Many determinants (cultural, contextual, and behavioral) affect antibiotic use in hospitals. The great diversity of the determinants dictates that measures or strategies to improve antibiotic use need to be equally diverse50.
Age >60 years was considered an independent risk factor for the acquisition of ORSA (p = 0.04), as were previous antibiotic therapy (p = 0.04) and previous use of carbapenems (p = 0.03). These risk factors correspond to what is reported in the literature, which includes underlying diseases, prior hospitalization, duration of hospitalization, admission to ICU, central venous catheterization, enteral feeding, nursing staff workload, and poor compliance with hand hygiene2,39,51,52.
There was a significant relationship between colonization of the oropharyngeal mucosa and the risk of VAP by ORSA or OSSA. The consumption of antibiotics was high mainly for broad-spectrum cephalosporins, and the high density of use of glycopeptides was associated with colonization by ORSA. Age >60 years, previous antibiotic therapy, and previous use of carbapenems were considered independent risk factors for acquisition of ORSA. However, despite a high rate of colonization by this microorganism, its involvement in the etiology of VAPs was small, overcome by Gram-negative bacilli.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
FINANCIAL SUPPORT
Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES).
Received in 29/06/2011
Accepted in 03/08/2011
References
- 1. Kollef MH. What Is Ventilator-Associated Pneumonia and Why Is It Important? Respir Care 2005; 50:714-724.
- 2. Tacconelli E, Angelis GD, Cataldo MA, Pozzi E, Cauda R. Does antibiotic exposure increase the risk the risk of methicillin-resistant Staphylococcus aureus (MRSA) isolation? A Systematic review and meta-analyisis. J Antimicrob Chemother 2008; 61:26-38.
- 3. Ott E, Bange FC, Reichardt C, Graf K, Eckstein M, Schwab F, et al. Cost of nosocomial pneumonia caused by methicillin-resistant Staphylococcus aureus J Hosp Infect 2010; 76:300-303.
- 4. Morehead RS, Pinto SJ. Ventilator-associated pneumonia. Arch Intern Med 2000; 160:1926-1936.
- 5. Joseph NM, Sistla S, Dutta TK, Badhe AS, Parija SC. Ventilator-associated pneumonia: role of colonizers and value of routine endotracheal aspirate cultures. Int J Infect Dis 2010; 14:723-739.
- 6. Erbay RH, Yalcin AN, Zencir M, Serin S, Atalay H. Costs and risk factors for ventilator-associated pneumonia in a Turkish university hospital's intensive care unit: a case-control study. BMC Pulm Med 2004; 4:3.
- 7. Rello J, Ollendorf DA, Oster G, Vera-Llonch M, Bellm L, Redman R, et al. Epidemiology and outcomes of ventilator-associated pneumonia in a large US database. Chest 2002; 122: 2115-2121.
- 8. Niven DJ, Laupland KD, Gregson DB, Church, DL. Epidemiology of Staphylococcus aureus nasal colonization and influence on outcome in the critically ill. J Critical Care 2009; 24:583-589.
- 9. Sakar P, Gould IM. Antimicrobial agents are societal drugs: how should this influence prescribing? Drugs 2006; 66:893-901.
- 10. Gould IM. Controversies in infection: infection control or antibiotic stewardship to control healthcare-acquired infection? J Hosp Infect 2009; 73:386-391.
- 11. Gould IM. Antibiotic policies to control hospital-acquired infection. J Antimicrob Chemother 2008; 61:763-765.
- 12. Dancer SJ. The effect of antibiotics on methicillin-resistant Staphylococcus aureus J Antimicrob Chemother 2008; 61:246-253.
- 13. Cheng VCC, Li IWS, Wu AKL, Tang BSF, Ng KHL, To KKW, et al. Effect of antibiotics on the bacterial load of methicillin-resistant Staphylococcus aureus colonization in anterior nares. J Hosp Infect 2008; 70:27-34.
- 14. Trouillet JL, Chastre J, Vuagnat A, Joly-Guillou M, Combaux D, Dombret M, et al. Ventilator-Associated Pneumonia Caused by Potentially Drug-resistant Bacteria. Am J Respir Crit Care Med 1998; 157:531-539.
- 15. Leroy O, Jaffré S, Escrivan T, Devos P, Georges H, Alfandari S, et al. Hospital-acquired pneumonia: Risk Factors for Antimicrobial-Resistance Causative Pathogens in Critically Ill Patients. Chest 2003; 123:2034-2042.
- 16. Alp E, Voss A. Ventilator Associated Pneumonia and Infection Control. Ann Clinic Microbiol Antimicrob 2006; 5:7.
- 17. Dean AG. Epi Info: A word processing, database, and statistics program for epidemiology on microcomputers [CD]. Version 5.0. Space Mountain, USD, G.A:CDC/WHO; 1995.
- 18. GraphPad Prism [Internet]. Version 3.0: San Diego, CA, USA. [Accessed 2011 May 3]; Available from: http://www.graphpad.com/prism/Prim.htm/
- 19. Ayres M, Ayres Jr M, Ayres DL, Santos AA. BioEstat: Aplicações Estatísticas nas Áreas de Ciências Biomédicas [Internet]. Belém, Brazil: Ong Mamiraua; 2007. Available from HTTP://www.mamiraua.org.br/download Accessed 2011 May 3.
- 20. Vincent JL. Nosocomial infectious in adult intensive-care units. Lancet 2003; 36:2068-2773.
- 21. Paterson DL. "Collateral Damage" from Cephalosporin or Quinolone Antibiotic Therapy. Clin Infect Dis 2004; 38 (suppl 4):341-345.
- 22. Joseph NM, Sistla S, Dutta TK, Badhe AS, Parija SC. Ventilator-associated pneumonia: A review. Eur J Intern Med 2010; 21:360-368.
- 23. Safdar N, Crnich CJ, Maki DG. The Pathogenesis of Ventilator-Associated Pneumonia: Its Relevance to Developing Effective Strategies for Prevention. Respir Care 2005; 50:725-739.
- 24. Rello J, Diaz E. Pneumonia in the intensive care unit. Crit Care Med 2003; 31:2544-2551.
- 25. Ringberg H, Petersson AC, Walder M, Johansson PJH. The throat: an important site for MRSA colonization. Scand J Infect Dis 2006; 38:888-893.
- 26. Marshall C, Spelman D. Is throat screening necessary to detect methicillin-resistant Staphylococcus aureus colonization in patients upon admission to an intensive care unit? J Clin Microbiol 2007; 45:3855.
- 27. Bignardi GE, Lowes S. MRSA screening: throat swabs are better than nose swabs. J Hosp Infect 2009; 71:373-374.
- 28. Yamamoto T, Nishiyama A, Takano T, Yabe S, Higuchi W, Razvina O, et al. Community-acquired methicillin-resistant Staphylococcus aureus: community transmission, pathogenesis, and drug resistance. J Infect Chemother 2010; 16:225-254.
- 29. Sarikonda KV, Micek ST, Doherty JA, Reichley RM, Warren D, Kollef MH. Methicillin-resistant Staphylococcus aureus nasal colonization is a poor predictor of intensive care unit-acquired methicillin-resistant infections requiring antibiotic treatment. Crit Care Med 2010; 38:1991-1995.
- 30. Garrouste-Orgeas M, Chevret S, Arlet G, Marie O, Rouveau M, Popoff N, et al. Oropharyngeal or Gastric Colonization and Nosocomial Pneumonia in Adult Intensive Care Unit Patients. A Prospective Study Based on DNA Analysis. Am J Resp Crit Care Med 1997; 156:1647-1655.
- 31. Cavalcanti M, Valencia M, Torres A. Respiratory nosocomial infections in the medical intensive care unit. Microbes Inf 2005; 7:292-301.
- 32. Vincent J, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, et al. International Study of the Prevalence and Outcome of Infection in Intensive Care Units. JAMA 2009; 302:2323-2329.
- 33. Struelens MJ, Monnet DL. Prevention of methicillin-resistant Staphylococcus aureus infection: is Europe winning the fight? Infect Control Hosp Epidemiol 2010; 31 (suppl 1):42-44.
- 34. Lucet JC, Paoletti X, Lolom I, Paugam-Burtz C, Trouillet JL, Timsit JF, et al. Successful long-term program for controlling methicillin-resistant Staphylococcus aureus in intensive care units. Intensive Care Med 2005; 31:1051-1057.
- 35. Tacconelli E. Screening and isolation for infection control. J Hosp Infect 2009; 73:371-377.
- 36. Padovese MC, Assis DB, Freire MP, Madalosso G, Ferreira SA, Valente MG, et al.; Surveillance programme for Healthcare Associated Infections in the State of São Paulo, Brazil. Implementation and first three years' results. J Hosp Infect 2010; 76:311-315.
- 37. Welte T, Pletz MW. Antimicrobial treatment of nosocomial methicillin-resistant Staphylococcus aureus (MRSA) pneumonia: current and future options. Internat J Antimicrob Agents 2010; 36:391-400.
- 38. Peleg AY, Hooper DC. Hospital-Acquired Infections Due to Gram-Negative Bacteria. N Engl J Med 2010; 362:1804-1813.
- 39. Graffunder EM, Venezia RA. Risk factors associated with nosocomial methicillin-resistant Staphylococcus aureus (MRSA) infection including previous use of antimicrobials. J Antimicrob Chemother 2002; 49:999-1005.
- 40. Marshall C, Wolfe R, Kossman T, Wesselingh S, Harrington G, Spelman D. Risk factors for acquisition of methicillin-resistant Staphylococcus aureus (MRSA) by trauma patients in the intensive care unit. J Hosp Infect 2004; 57:245-252.
- 41. Bloemendaal ALA, Fluit AC, Jansen WMT, Vriens MR, Ferry T, Argaud L, et al. Acquisition and Cross-Transmission of Staphylococcus aureus in European Intensive Care Units. Infect Control Hosp Epidemiol 2009; 30:117-124.
- 42. Washio M. Risk factors for methicillin-resistant Staphylococcus aureus (MRSA) infection in a Japanese elderly care nursing home. Epidemiol Infect 1997; 119:285.
- 43. Washio M, Mizoue T, Kajioka T, Yoshimitsu T, Okayama M, Hamada T, et al. Risk factors for methicillin-resistant Staphylococcus aureus (MRSA) infection in a Japanese geriatric hospital. Public Health 1997; 111:187-190.
- 44. Onorato M, Borucki MJ, Baillargeon G. Risk factors for colonization or infection due to methicillin-resistant Staphylococcus aureus in HIV-positive patients: a retrospective case-control study. Infect Control Hosp Epidemiol 1999; 20:26-30.
- 45. Aldeyab MA, Monnet DL, López-Lozano JN, Hughes CM, Scott MG, Kearney MP, et al. Modelling the impact of antibiotic use and infection control practices on the incidence of hospital-acquired methicillin-resistant Staphylococcus aureus: a time-series analysis. J Antimicrob Chemother 2008; 62:593-600.
- 46. Meyer E, Jonas D, Schwab F, Rueden H, Gastmeier P, Daschener FK. Design of a Surveillance System of Antibiotic Use and Bacterial Resistance in German Intensive Care Units (SARI). Infection 2003; 31:208-215.
- 47. National Nosocomial Infections Surveillance (NNIS) System Report, data summary from January 1992 through June 2004, issued October 2004. Am J Infect Control 2004; 32:470-485.
- 48. Dellit TH, Owens RC, McGowa Jr JE. Infectious Diseases Society of America an Society for Healthcare Epidemiology of America Guidelines developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis 2007; 44:159-177.
- 49. Tacconelli E. Antimicrobial use: risk driver of multidrug resistant microorganisms in healthcare settings. Curr Opin Infect Dis 2009; 22:352-358.
- 50. Hulscher MEJL, Grol RPTM, Van Der Meer JWM. Antibiotic prescribing in hospitals: a social and behavioural scientific approach. Lancet Infect Dis 2010; 10:167-175.
- 51. Grundmann H, Hori S, Winter B, Tami A, Austin DJ. Risk factor for the transmission of methicillin-resistant Staphylococcus aureus in an adult intensive care unit: fitting a model to the data. J Infect Dis 2002; 185:481-488.
- 52. Ho PL. For the Hong Kong Intensive Care Unit Antimicrobial Resistance Study (HK-ICARE) Group. Carriage of methicillin-resistant Staphylococcus aureus, ceftazidime-resistant Gram-negative bacilli, and Vancomycin-resistant enterococci before and after intensive care unit admission. Crit Care Med 2003; 31:1175-1182.