Abstracts
OBJECTIVE: To analyze the trends in asthma prevalence in children and adolescents between 1998 and 2008 in Brazil. METHODS: Data on asthma prevalence from the 1998, 2003 and 2008 National Household Sample Surveys were analyzed. The sample was comprised of 141,402, 144,443 and 134,032 individuals in 1998, 2003 and 2008, respectively, and the analysis was adjusted for the sample design. Trends in asthma prevalence were described for sex, Brazilian regions and place of residence of children (zero to nine years of age) and adolescents (ten to 19 years of age). RESULTS: The prevalence of asthma in children was 7.7% in 1998, 8.1% in 2003 and 8.5% in 2008, with an annual increase of 1%. The highest annual increase was observed in the Southeast and North regions (1.4%). Among adolescents, the prevalence of asthma was 4.4% in 1998, 5.0% in 2003 and 5.5% in 2008, with an increase of 2.2% per year. In the Northeast region, the annual increase in the prevalence of asthma was 3.5%. The greatest increases were observed in boys and in residents of rural areas. CONCLUSIONS: Although asthma has decreased in some developing countries, the results found in Brazil point to an increase in this disease in children and adolescents between 1998 and 2008, especially in rural areas.
Child; Adolescent; Asthma, epidemiology; Time Series Studies
OBJETIVO: Analisar as tendências de asma em crianças e adolescentes entre 1998 e 2008 no Brasil. MÉTODOS: Foram analisados os dados de prevalência de asma da Pesquisa Nacional por Amostra de Domicílios, dos anos de 1998, 2003 e 2008. A amostra foi constituída por 141.402, 144.443 e 134.032 indivíduos em 1998, 2003 e 2008, respectivamente, e a análise foi ajustada pelo desenho amostral. As tendências de asma foram descritas por sexo, regiões do Brasil e local de residência, em crianças (zero a nove anos) e adolescentes (dez a 19 anos). RESULTADOS: A prevalência de asma entre crianças foi 7,7% em 1998, 8,1% em 2003 e 8,5% em 2008, com um incremento anual de 1%. O maior aumento anual foi observado nas regiões Sudeste e Norte (1,4%). Entre o grupo de adolescentes, a prevalência de asma foi de 4,4% em 1998, 5,0% em 2003 e 5,5% em 2008, com aumento de 2,2% ao ano. Na região Nordeste, o aumento anual na prevalência de asma foi de 3,5%. Os maiores incrementos foram observados entre os meninos e entre moradores da zona rural. CONCLUSÕES: Apesar de a asma apresentar um decréscimo em países emergentes, no Brasil os resultados apontam um incremento da asma entre crianças e adolescentes no período de 1998 e 2008, especialmente na zona rural.
Criança; Adolescente; Asma, epidemiologia; Estudos de Séries Temporais
OBJETIVO: Analizar las tendencias de asma en niños y adolescentes entre 1998 y 2008 en Brasil. MÉTODOS: Se analizaron los datos de prevalencia de asma de la Investigación Nacional por Muestra de Domicilios, de los años de 1998, 2003 y 2008. La muestra fue constituida por 141.402, 144.443 y 134.032 individuos en 1998, 2003 y 2008, respectivamente y el análisis fue ajustado por el diseño muestral. Las tendencias de asma fueron descritas por sexo, regiones de Brasil y lugar de residencia, en niños (cero a nueve años) y adolescentes (diez a 19 años). RESULTADOS: La prevalencia de asma entre niños fue de 7,7% en 1998, 8,1% en 2003 y 8,5% en 2008, con un incremento anual de 1%. El mayor aumento anual fue observado en la región Sureste y Norte (1,4%). Entre el grupo de adolescentes, la prevalencia de asma fue de 4,4% en 1998, 5,0% en 2003 y 5,5% en 2008, con aumento de 2,2% al año. En la región Noreste, el aumento anual en la prevalencia de asma fue de 3,5%. Los mayores incrementos fueron observados entre los varones y entre habitantes de la zona rural. CONCLUSIONES: A pesar de el asma presentar una disminución en países en desarrollo, en Brasil, los resultados señalan un incremento del asma entre niños y adolescentes en el período de 1998 y 2008, especialmente en la zona rural.
Niño; Adolescente; Asma, epidemiología; Estudios de Series Temporales
ORIGINAL ARTICLES
Time trend of asthma in children and adolescents in Brazil, 1998-2008
Fernando César WehrmeisterI; Ana Maria Baptista MenezesI, II; Andreia Morales CascaesI; Jeovany Martínez-MesaI; Aluisio J D BarrosI, III
IPrograma de Pós-Graduação em Epidemiologia. Universidade Federal de Pelotas (UFPel). Pelotas, RS, Brasil
IIDepartamento de Clínica Médica. Faculdade de Medicina (FM). UFPel. Pelotas, RS, Brasil
IIIDepartamento de Medicina Social. FM-UFPel. Pelotas, RS, Brasil
Correspondence Correspondence: Fernando César Wehrmeister R. Marechal Deodoro, 1160 - 3º piso Centro 96020-220 Pelotas, RS, Brasil E-mail: fcwehrmeister@yahoo.com.br
ABSTRACT
OBJECTIVE: To analyze the trends in asthma prevalence in children and adolescents between 1998 and 2008 in Brazil.
METHODS: Data on asthma prevalence from the 1998, 2003 and 2008 National Household Sample Surveys were analyzed. The sample was comprised of 141,402, 144,443 and 134,032 individuals in 1998, 2003 and 2008, respectively, and the analysis was adjusted for the sample design. Trends in asthma prevalence were described for sex, Brazilian regions and place of residence of children (zero to nine years of age) and adolescents (ten to 19 years of age).
RESULTS: The prevalence of asthma in children was 7.7% in 1998, 8.1% in 2003 and 8.5% in 2008, with an annual increase of 1%. The highest annual increase was observed in the Southeast and North regions (1.4%). Among adolescents, the prevalence of asthma was 4.4% in 1998, 5.0% in 2003 and 5.5% in 2008, with an increase of 2.2% per year. In the Northeast region, the annual increase in the prevalence of asthma was 3.5%. The greatest increases were observed in boys and in residents of rural areas.
CONCLUSIONS: Although asthma has decreased in some developing countries, the results found in Brazil point to an increase in this disease in children and adolescents between 1998 and 2008, especially in rural areas.
Descriptors: Child. Adolescent. Asthma, epidemiology. Time Series Studies.
INTRODUCTION
Asthma affects approximately 300 million people worldwide,12 with negative consequences for individuals and society. These consequences, such as days and costs resulting from hospitalizations, have an economic and social impact in Brazil,ª a Globl Strtegy for Asthm Mngement nd Prevention: updted 2009. Cpe Town: University of Cpe Town Lung Institute; 2009. where asthma is an important public health problem.8 A Brazilian study assessed death certificates and included asthma as a cause of death, revealing a mortality rate of 2.29 per 100,000 inhabitants, standardized for the Brazilian population in 2000.18 Asthma affects all ages, especially children and adolescents.6 Although several studies on asthma prevalence have been performed worldwide, there is no consensus on a single accurate measure to define this disease,ª a Globl Strtegy for Asthm Mngement nd Prevention: updted 2009. Cpe Town: University of Cpe Town Lung Institute; 2009. which is usually assessed with a medical diagnosis or the presence of its symptoms.
Time trends of asthma show different patterns according to geographical areas. In the United States, between 1980 and 2007, there was a stabilization in the prevalence of asthma in childhood, with a reduction in mortality rates in the same period.1 A study conducted by Pearce et al,15 with data from the International Study of Asthma and Allergy in Childhood (ISAAC), showed a reduction in asthma in English-speaking countries and Western Europe. In contrast, there was an increase in the asthma prevalence throughout the years in countries where the prevalence was considered to be low. In Latin America, the prevalence of asthma symptoms has increased.15 Nonetheless, in South America, a systematic review pointed to inconsistencies in the decreasing or increasing pattern of asthma prevalence in studies that use the ISAAC methodology.3
The Pesquisa Nacional por Amostra de Domicílios (PNAD - National Household Sample Survey), performed by the Instituto Brasileiro de Geografia e Estatística (IBGE - Brazilian Institute of Geography and Statistics), regularly investigates health aspects of the population. This survey is conducted with a representative sample of states, Brazilian regions and the country. A total of three studies on the health of the Brazilian population have been conducted, including the question of the medical diagnosis of asthma, which enables the establishment of a time trend of this problem in Brazil, thus contributing to the monitoring of the medical diagnosis of asthma throughout time and the implementation of public policies.
The present study aimed to analyze the trends of asthma prevalence in children and adolescents between 1998 and 2008, in Brazil.
METHODS
The study was conducted with data derived from the 1998, 2003 and 2008 PNAD health supplements.
The PNAD sampling plan follows three stages (cities, census tracts and households), being representative for the country, regions, states and certain metropolitan areas.21 In 1998, the sample was comprised of 344,975 individuals; in 2003, 384,834; and in 2008, 391,868. More information about the methodological aspects can be obtained on the website of IBGE.b b Instituto Brasileiro de Geografia e Estatística. Pesquisa Nacional por Amostra de Domicílios. [cited 2012 Jan 13]. Available from: http://www.ibge.com.br/home/estatistica/populacao/ trabalhoerendimento/pnad2008/default.shtm para o ano de 2008; http://www.ibge.com.br/home/estatistica/ populacao/trabalhoerendimento/pnad2003/default.shtm for 2003; the year 1998 is not accessible through the worldwide web.
The study population was comprised of individuals aged between zero and 19 years, thus characterizing the periods of childhood and adolescence, in accordance with the World Health Organization (WHO). According to the DATASUS Health Information System, the age group included in this study corresponded to 42% of the country's population in 1998, 40% in 2003, and 35% in 2008.c c DATASUS. Sistema de Informações em Saúde. Brasília (DF) [cited 2011 Feb 22]. Available from: http://tabnet.datasus.gov.br/cgi/deftohtm.exe?ibge/cnv/popuf.def
The following closed-ended question was used to define asthma prevalences in each year: "Has any doctor or health professional said that (...) has/have asthma or bronchitis?".
The analyses were performed for the country and also stratified per age groups, Brazilian regions and area of residence. Age groups were dichotomized into participants aged between zero and nine years and participants aged between ten and 19 years. Asthma prevalences were also analyzed according to regions (North, Northeast, Southeast, South and Central-West). Finally, the area of residence was dichotomized into "urban" (city or village in an urban area, city or village in a non-urban area and isolated urban area) and "rural" (rural cluster with an urban extension, isolated rural cluster and settlement, isolated rural cluster - nucleus, isolated rural cluster - other types of cluster, and rural area except for rural cluster).
The databases were obtained from the IBGE. Data were analyzed in the STATA statistical package, version 11.0, using the svyset command to define sample weights and clusters and the svy command for all analyses performed, considering the sampling process complexity. Asthma prevalences were obtained for the country and per region, in addition to annual percentage variations. Moreover, this information was stratified per area of residence and sex.
The mean annual percentage variation of the prevalences observed was calculated with the values found in 1998 and 2008. The total percentage variation was calculated, with the mean annual variation being estimated as a tenth root:
where p1998 and p2008 are the prevalences calculated for 1998 and 2008, respectively. The Wald test for linear trend was used to observe the time trend.
RESULTS
The sample of children and adolescents studied in 1998, 2003 and 2008 was comprised of 141,402, 144,443 and 134,032 individuals, respectively. This age group including childhood and adolescence corresponded to 41% of the sample in 1998, 35% in 2003, and 34% in 2008.
The sample characteristics in each year of the PNAD are shown in Table 1. In all years studied, there was a slight predominance of males among children and adolescents. The most frequent area of residence was the urban area in all years studied. There was an increase of approximately 5.0 percentage points in children living in the urban area in 2008, when compared to 1998. Among adolescents, this increase totaled 2.5 percentage points in the same period. In addition, there was a reduction in the proportion of children and adolescents living in the Northeast, Southeast and South regions, whereas the North and Central-West regions had an increase in the proportion of residents aged between zero and 19 years (Table 1). The mean per capita household income increased in the period studied, totaling R$ 359.30 in 2008 (SD = 580.90) in the zero-to-nine-year age group, and R$ 407.20 in the ten-to-19-year age group (SD = 606.70).
Figure 1 shows the asthma prevalences according to the area of residence and sex in children aged between zero and nine years, per year of PNAD. Regardless of the area of residence, there was an increase in prevalence in the period studied. In the urban area, the prevalences varied from 8.6% in 1998 to 8.7% in 2003 and 9.1% in 2008. In the rural area, they varied between 4.9% and 5.9%, from 1998 to 2008. The prevalence of asthma was higher in male children, in both rural and urban areas.
Table 2 shows the prevalence of asthma and annual variation in children aged between zero and nine years, in general and per Brazilian region. The prevalence of asthma in children varied from 7.7% to 8.5% in 1998 and 2008, respectively. With the exception of the Central-West region, where there was a decline that varied between 0.7% (when the female sex was evaluated) and 3.0% (in the rural area), all Brazilian regions and the country as a whole showed an increase in asthma prevalence, although not statistically significant in some cases. In Brazil, the annual increase was lower in the urban area (0.6%, p=0.006) than in the rural area (1.8%, p=0.002). In the rural area, annual increases in asthma prevalence were 3.5% (p<0.001) in the Northeast region and 2.2% (p=0.035) in the Southeast region.
The trend in asthma prevalence in adolescents according to area of residence and sex is shown in Figure 2. This prevalence also increased in the period studied, although the differences between sexes were not as relevant as they were in children. The exception was the urban area in 2003, when male adolescents had a prevalence of 6.1%, whereas female adolescents had a prevalence of approximately 4.7%. In the urban area, the prevalences varied from 4.9% to 5.9% between 1998 and 2008, while this variation ranged from 2.5% to 3.5%, in 1998 and 2008, respectively.
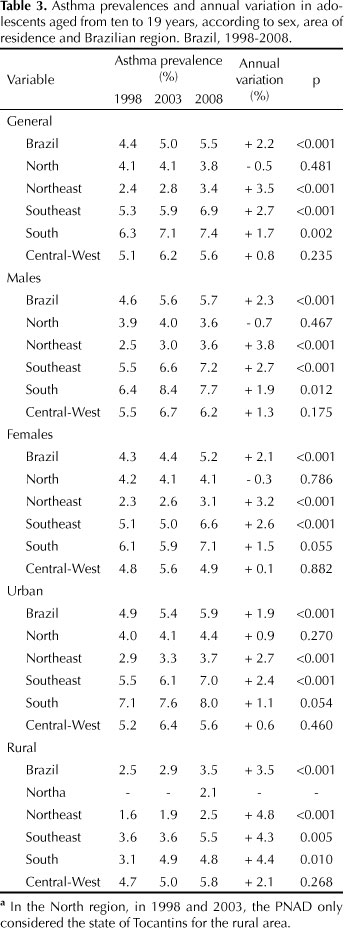
The annual variations and prevalences for adolescents are shown in Table 3. The variation in asthma prevalence was between 4.4% and 5.5%. Although with lower prevalences, adolescents had higher percentage variations than children. The percentage variation in the country points to an annual increase in asthma prevalence of 2.2% (p<0.001) in the ten-to-19-year age group. This increase corresponded to 1.9% (p<0.001) in the urban area and 3.5% (p<0.001) in the rural area. Although the North region showed an annual decrease of 0.5% in this prevalence in the ten-to-19-year age group, this same region pointed to an increase of 0.9% in the urban area, both of which were not statistically significant. Once again, the annual increase in asthma prevalence in the rural area was emphasized, totaling 4.8% (p<0.001) in the Northeast region, and 4.3% (p=0.005), 4.4% (p=0.010) and 2.1% (p=0.268) in the Southeast, South and Central-West regions, respectively.
DISCUSSION
The results of the present study indicate a general increase in the diagnosis of asthma in children and adolescents in different Brazilian regions, in both sexes, and in the rural and urban areas, between 1998 and 2008. The greatest increases were observed in males and in those living in the rural area.
Despite the national scope, with representativeness for states and regions, and methodological rigor, analyses based on PNAD data can have certain limitations. One of them is the possible underestimation of asthma prevalence, as it depends on the diagnosis by a medical doctor or health professional. If the asthma assessment criteria had taken its symptoms into account, prevalences could have been higher in all the years studied. Another point to be considered as a limitation is that the outcome was assessed in all years in a retrospective way, which could also have led to an underestimation of magnitude.
One of the main difficulties in the comparison of results is the way the disease is assessed, which could vary from the presence of symptoms such as wheezing in the last 12 months; a medical diagnosis; to tests being performed, such as the bronchoprovocation test with methacoline conducted in a hospital environment. As an example, asthma prevalences are usually higher in studies that use the presence of symptoms to define the outcome,22 which can be partly explained by the greater access to health services.
The recent literature on time trends in asthma shows the large use of the comparison between stages I and III of ISAAC,2,5,11,15,16,20 which observed this prevalence in the six-and-seven-year age group, in the 13-and-14-year age group, or in both. However, the majority of these studies were performed in Europe and Asia; only three of these were conducted in Latin America, of which one was in Chile11 and two in Brazil.16,20 The ISAAC investigates the prevalences of wheezing in the last 12 months and self-reported asthma in life as outcomes of this disease. Nonetheless, ISAAC studies make a comparison between two periods and, consequently, characterize its evolution rather than its time trend, as the latter requires at least three points in time.
The present study showed the increase in prevalence of asthma in children and adolescents during a period of ten years (from 1998 to 2008). This result is similar to that of other studies, although these assessed the outcome differently. In Greece, Anthracopoulos et al4 found an increase from 8.0% in 1991 to 12.4% in 2003 by assessing the medical diagnosis of children aged between eight and ten years. In the United States, data from the Centers for Disease Control and Prevention pointed to an increase of 4.6% from 1980 to 1996 and a stability in the prevalence of asthma in individuals aged between zero and 17 years, between 1997 and 2007.1
By analyzing information from all countries that participated in the ISAAC, Pearce et al15 observed an annual increase in asthma prevalence in adolescents that varied between 0.07% in Africa and 0.93% in Oceania. Only in the Indian subcontinent was there an annual decrease of 0.01%. In children aged between six and seven years, the annual increase varied from 0.12% on the Asian side of the Pacific Ocean to 0.74% in North America. In Africa, Eastern Mediterranean and Latin America, there was an annual decrease in prevalence of 0.01%, 0.05% and 0.15%, respectively.
There were disagreements among the findings when studies conducted in South America were compared. In Chile,11 a study derived from the ISAAC project pointed to a reduction in prevalence from 12.5% in 1994 to 10.7% in 2002 in the six-to-seven-year age group, although not being statistically significant. In contrast, among adolescents aged between 13 and 14 years, there was an increase from 10.2% to 14.9% in the same period. In Brazil,20 also as part of the ISAAC, the prevalence of asthma remained stable in individuals aged between 13 and 14 years (from 14.9% in 1994 to 14.7% in 2002). However, it should be emphasized that studies using the ISAAC methodology provide a self-reported prevalence of asthma rather than the medical diagnosis of this disease, as in the PNAD.
The prevalence of asthma increased at least ten times in recent decades, especially in developed countries, but also in developing countries such as Brazil and other Latin American countries.8 Some explanations can be attributed to the increase in primary health care services and the number of family health teams in all Brazilian regions. As an example, the expansion of family health teams between 1999 and 2004 was greater in the Northeast region than in the South region.9 Considering the fact that the outcome was assessed with the question about medical diagnosis, it is assumed that the increase in access to and use of health services could partly explain the increase in asthma prevalences, especially in the rural area.
Another factor that could explain the increase in asthma in rural populations is their greater exposure to pesticides. Although this is only a hypothesis in the theoretical sphere and based on scientific speculation, researchers consider it to be an important aspect to be approached in future Brazilian studies.
The highest prevalences of asthma in males coincide with what has been described in previous publications. A study conducted with students in 1984, 1994, 1999 and 2004 by Osman et al14 found higher prevalences and time trends of asthma in males. In children, the highest prevalences of asthma in males, when compared to females, can be explained by physiological disadvantages.23 Boys at this age tend to have higher IgE concentrations than girls,19 in addition to lower respiratory flow rates.10,17
Asthma management conditions in Brazil are below what is ideal. Considering the fact that asthma is a disease sensitive to primary health care management, hospitalizations are viewed as inevitable.13 A study on the trend of medical diagnosis of asthma in the United States7 pointed out that, in addition to medication, good asthma self-management training is also required. Thus, it becomes important to improve primary health care coverage in Brazil, including public policies aimed at asthma control and management.
REFERENCES
Received: 5/17/2011
Approved: 10/9/2011
The authors declare no conflicts of interests.
- 1. Akinbami LJ, Moorman JE, Garbe PL, Sondik EJ. Status of childhood asthma in the United States, 1980-2007. Pediatrics 2009;123 (Suppl 3):S131-45. DOI:10.1542/peds.2008-2233C
- 2. Al-Rawas OA, Al-Riyami BM, Al-Maniri AA, Al-Riyami AA. Trends in asthma prevalence and severity in Omani schoolchildren: comparison between ISAAC phases I and III. Respirology 2008;13(5):670-3. DOI:10.1111/j.1440-1843.2008.01313.x
- 3. Anandan C, Nurmatov U, van Schayck OC, Sheikh A. Is the prevalence of asthma declining? Systematic review of epidemiological studies. Allergy 2010;65(2):152-67. DOI:10.1111/j.1398-9995.2009.02244.x
- 4. Anthracopoulos MB, Liolios E, Panagiotakos DB, Triantou K, Priftis KN. Prevalence of asthma among schoolchildren in Patras, Greece: four questionnaire surveys during 1978-2003. Arch Dis Child 2007;92(3):209-12. DOI:10.1136/adc.2006.106153
- 5. Asher MI, Stewart AW, Clayton T, Crane J, Ellwood PI, Mackay R, et al. Has the prevalence and severity of symptoms of asthma changed among children in New Zealand? ISAAC Phase Three. N Z Med J 2008;121(1284):52-63.
- 6. Bousquet J, Clark TJ, Hurd S, Khaltaev N, Lenfant C, O'Byrne P, et al. GINA guidelines on asthma and beyond. Allergy 2007;62(2):102-12. DOI:10.1111/j.1398-9995.2006.01305.x
-
7Centers for Disease Control and Prevention. Vital signs: asthma prevalence, disease characteristics, and self-management education: United States, 2001-2009. MMWR Morb Mortal Wkly Rep 2011;60(17):547-52.
- 8. Cooper PJ, Rodrigues LC, Cruz AA, Barreto ML. Asthma in Latin America: a public heath challenge and research opportunity. Allergy 2009;64(1):5-17. DOI:10.1111/j.1398-9995.2008.01902.x
- 9. Facchini LA, Piccini RX, Tomasi E, Thumé E, Silveira DS, Siqueira FV, et al. Desempenho do PSF no Sul e no Nordeste do Brasil: avaliação institucional e epidemiológica da Atenção Básica à Saúde. Cienc Saude Coletiva 2006;11(3):669-81. DOI:10.1590/S1413-81232006000300015
- 10. Hibbert M, Lannigan A, Raven J, Landau L, Phelan P. Gender differences in lung growth. Pediatr Pulmonol 1995;19(2):129-34.
- 11. Mallol J, Aguirre V, Aguilar P, Calvo M, Amarales L, Arellano P, et al. Cambios em la prevalencia de asma em escolares chilenos entre 1994 y 2002: International Study of Asthma and Allergies in Childhood (ISAAC: Chile phases I and III. Rev Med Chil 2007;135(5):580-6. DOI:/S0034-98872007000500005
- 12. Masoli M, Fabian D, Holt S, Beasley R. The global burden of asthma: executive summary of the GINA Dissemination Committee report. Allergy 2004;59(5):469-78. DOI:10.1111/j.1398-9995.2004.00526.x
- 13. Nedel FB, Facchini LA, Martin-Mateo M, Vieira LAS, Thumé E. Programa Saúde da Família e condições sensíveis à atenção primária, Bagé (RS). Rev Saude Publica 2008;42(6):1041-52. DOI:10.1590/S0034-89102008000600010
- 14. Osman M, Tagiyeva N, Wassall HJ, Ninan TK, Devenny AM, McNeill G, et al. Changing trends in sex specific prevalence rates for childhood asthma, eczema, and hay fever. Pediatr Pulmonol 2007;42(1):60-5. DOI:10.1002/ppul.20545
- 15. Pearce N, Ait-Khaled N, Beasley R, Mallol J, Keil U, Mitchell E, et al. Worldwide trends in the prevalence of asthma symptoms: phase III of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax 2007;62(9):758-66. DOI:10.1136/thx.2006.070169
- 16. Riedi CA, Rosario NA, Ribas LF, Backes AS, Kleiniibing GF, Popija M, et al. Increase in prevalence of rhinoconjunctivitis but not asthma and atopic eczema in teenagers. J Investig Allergol Clin Immunol 2005;15(3):183-8.
- 17. Rosenthal M, Bain SH, Cramer D, Helms P, Denison D, Bush A, et al. Lung function in white children aged 4 to 19 years: I. Spirometry. Thorax 1993;48(8):794-802.
- 18. Santo AH. Mortalidade relacionada à asma, Brasil, 2000: um estudo usando causas múltiplas de morte. Cad Saude Publica 2006;22(1):41-52. DOI:10.1590/S0102-311X2006000100005
- 19. Sears MR, Burrows B, Flannery EM, Herbison GP, Holdaway MD. Atopy in childhood. I. Gender and allergen related risks for development of hay fever and asthma. Clin Exp Allergy 1993;23(11):941-8.
- 20. Sole D, Melo KC, Camelo-Nunes IC, Freitas LS, Britto M, Rosario NA, et al. Changes in the prevalence of asthma and allergic diseases among Brazilian schoolchildren (13-14 years old): comparison between ISAAC Phases One and Three. J Trop Pediatr 2007;53(1):13-21. DOI:10.1093/tropej/fml044
- 21. Travassos C, Viacava F, Laguardia J. Os suplementos Saúde na Pesquisa Nacional por Amostra de Domicílios (PNAD) no Brasil. Rev Bras Epidemiol 2008;11 (Supl 1):98-112. DOI:10.1590/S1415-790X2008000500010
- 22. Wandalsen NF, Gonzalez C, Wandalsen GF, Solé D. Avaliação de critérios para o diagnóstico de asma através de um questionário epidemiológico. J Bras Pneumol 2009;35(3):199-205. DOI:10.1590/S1806-37132009000300002
- 23. Wehrmeister FC, Peres KGA. Desigualdades regionais na prevalência de diagnóstico de asma em crianças: uma análise da Pesquisa Nacional por Amostra de Domicílios, 2003. Cad Saude Publica 2010;26(9):1839-52. DOI:10.1590/S0102-311X2010000900017
Correspondence:
Publication Dates
-
Publication in this collection
03 Feb 2012 -
Date of issue
Apr 2012
History
-
Received
17 May 2011 -
Accepted
09 Oct 2011