Abstracts
OBJECTIVE
To analyze if the distribution of specialized care services for HIV/AIDS is associated with AIDS rates.
METHODS
Ecological study, for which the distribution of 10 specialized care services in the Ceara state, Northeastern Brazil, was obtained, and the mean rates of the disease were estimated per mesoregion. We evaluated 7,896 individuals who had been diagnosed with AIDS, were aged 13 years or older, lived in Ceara, and had been informed of their condition between 2001 and 2011. Maps were constructed to verify the relationship between the distribution of AIDS cases and institutionalized support networks in the 2001-2006 and 2007-2011 periods. BoxMap and LisaMap were used for data analysis. The Voronoi diagram was applied for the distribution of the studied services.
RESULTS
Specialized care services concentrated in AIDS clusters in the metropolitan area. The Noroeste Cearense and west of the Sertoes Cearenses had high AIDS rates, but a low number of specialized care services over time. Two of these services were implemented where clusters of the disease exist in the second period. The application of the Voronoi diagram showed that the specialized care services located outside the metropolitan area covered a large territory. We identified one polygon that had no services.
CONCLUSIONS
The scenario of AIDS cases spread away from major urban areas demands the creation of social support services in areas other than the capital and the metropolitan area of the state; this can reduce access barriers to these institutions. It is necessary to create specialized care services for HIV/AIDS in the Noroeste Cearense and north of Jaguaribe.
Acquired Immunodeficiency Syndrome; Ambulatory Care; Equity in the Resource Allocation; Health Vulnerability; Ecological Studies
OBJETIVO
Analisar se a distribuição dos serviços de assistência especializada em HIV/aids está associada às taxas de aids.
MÉTODOS
Estudo ecológico, pelo qual foi obtida a distribuição de 10 serviços de assistência especializada em HIV/aids, no estado do Ceará. As taxas médias da doença foram calculadas por mesorregião. Estudaram-se 7.896 indivíduos notificados com aids, com idade igual ou superior a 13 anos, residentes no Ceará, no período de 2001 a 2011. Construíram-se mapas para verificar relação entre distribuição dos casos de aids e das redes institucionalizadas de apoio nos períodos de 2001 a 2006 e 2007 a 2011. Utilizou-se BoxMap e LisaMap para análise dos dados. Aplicou-se o diagrama de Voronoi para os serviços estudados.
RESULTADOS
Verificou-se concentração dos serviços de assistência especializada nosclusters de aids na Região Metropolitana do estado. O Noroeste Cearense e o oeste dos Sertões Cearenses apresentaram elevadas taxas de aids, porém baixa quantidade de serviços especializados ao longo do tempo. Houve implantação de dois serviços especializados no segundo período onde existem aglomerados da doença. A aplicação do Diagrama de Voronoi mostrou que os serviços localizados fora da Região Metropolitana abrangem grande extensão territorial. Foi identificado polígono sem nenhum serviço.
CONCLUSÕES
O cenário de interiorização dos casos de aids demanda a necessidade de criação de serviços de apoio social além da capital e da Região Metropolitana do estado, a fim de diminuir as barreiras de acesso a essas instituições. É necessário criar serviços de assistência especializada em HIV/aids no Noroeste Cearense e no norte do Jaguaribe.
Síndrome de Imunodeficiência Adquirida; Assistência Ambulatorial; Equidade na Alocação de Recursos; Vulnerabilidade em Saúde; Estudos Ecológicos
INTRODUCTION
Social support requirements involve, in addition to that given by family and friends, social relationships at institutionalized facilities. Social support networks can provide direct and indirect services, which are part of or complementary to the health service. These services can improve quality of life and disease management and help the adoption of new lifestyles – actions that may culminate in autonomy for the individual and his/her consequent empowerment.11 Arakawa T, Arcêncio RA, Scatolin BE, Scatena LM, Ruffino-Netto A, Villa TCS. Acessibilidade ao tratamento de tuberculose: avaliação de desempenho de serviços de saúde. Rev Latino-Am Enferm. 2011;19(4):1-9. DOI:10.1590/S0104-11692011000400019
The specialized care services (SCS) for people living with HIV/AIDS seek to promote material and emotional support, as well as provide care to the patient and their families, which can take the form of clarifying rights, prevention policies, and health promotion.1212 Renesto HMF, Falbo AR, Souza E, Vasconcelos MG. Enfrentamento e percepção da mulher em relação à infecção pelo HIV. Rev Saude Publica. 2014;48(1):36-42. DOI:10.1590/S0034-8910.2014048003186,1717 Silva JM, Silva CBC. HIV/aids e violência: da opressão que cala à participação que acolhe e potencializa. Saude Soc. 2011;20(3):635-46. DOI:10.1590/S0104-12902011000300010 The SCS are free services provided by the Brazilian Unified Health System (SUS). These services provide comprehensive, humanized, individual care, tend to users' vulnerabilities with multidisciplinary teams, and identify health care challenges, aiming to achieve user satisfaction by meeting the patients' needs and expectations.22 Borges MJL, Sampaio AS, Gurgel IGD. Trabalho em equipe e interdisciplinaridade: desafios para a efetivação da integralidade na assistência ambulatorial às pessoas vivendo com HIV/aids em Pernambuco.Cienc Saude Coletiva. 2012;17(1):147-56. DOI:10.1590/S1413-81232012000100017,1515 Schilkowsky LB, Portela MC, SA MC. Fatores associados ao abandono de acompanhamento ambulatorial em um serviço de assistência especializada em HIV/aids na cidade do Rio de Janeiro, RJ. Rev Bras Epidemiol. 2011;14(2):187-97. DOI:10.1590/S1415-790X2011000200001
Health promotion policies involve intersectoral actions that are always directed towards improving the living conditions for the individual and the population. In the midst of the AIDS epidemic and using the SUS principles and guidelines as a basis, activities that focus on the population's quality of life have emerged. Public policies geared towards these individuals were encouraged, ensuring the free distribution of antiretroviral therapy and looking to expand the SCS.88 Lima ICV, Galvao MTG, Paiva SS, Brito DMS. Ações de promoção da saúde em serviço de assistência ambulatorial especializada em HIV/Aids.Cienc Cuid Saude. 2011;10(3):556-63. DOI:10.4025/cienccuidsaude.v10i3.13193
In Brazil, the HIV/AIDS epidemic is characterized by the geographical diffusion of the disease towards small cities,1010 Nogueira JA, Silva AO, Sá LR, Almeida SA, Monroe AA, Villa TCS. AIDS in adults 50 years of age and over: characteristics, trends and spatial distribution of the risk. Rev Latino-Am Enfermagem. 2014;22(3):355-63. DOI:10.1590/0104-1169.3327.2424 which have little access to specialized health institutions and, consequently, a greater chance of late diagnosis and inadequate management of its associated diseases. In the Brazilian state of Ceara, 96.0% of all its cities have identified at least one case of AIDS.a a Instituto de Pesquisa e Estratégia Econômica do Ceará. Ceará em números. Fortaleza: Instituto de Pesquisa e Estratégia Econômica do Ceará; 2014 [cited 2014 May 21]. Available from: http://www.ipece.ce.gov.br/
Despite it not being an isolated factor, access to health services has been considered an important, impacting factor on the use of health-related services. Thus, the location of health facilities is a critical variable for providing quality health care. Identifying deficiencies in care coverage and disadvantaged groups is essential for managing health resources.2020 Yao J, Murray T. Locational effectiveness of clinics providing sexual and reproductive health services to women in rural Mozambique.Int Reg Sci Rev. 2014;37(2):172-93. DOI:10.1177/0160017614524227
Despite the advances in AIDS research, there are holes regarding the study of distributing specialized care services, which limits a true picture of these patients access to such institutions. The existence of accessible institutions that can meet the requirements that result from AIDS, along with the current dynamics of the disease, is a necessary challenge for modern society. The aim of this study was to analyze whether the distribution of the Specialized Care Services in HIV/AIDS is associated with AIDS rates.
METHODS
This ecological study used a geographical information system (GIS) as a tool. These types of systems make it possible to build a set of data and arrange them to process spatially referenced information using computational techniques, which enables the conditions of vulnerable populations to be evaluated in relation to one variable.33 Barcellos C, Zaluar A. Homicídios e disputas territoriais nas favelas do Rio de Janeiro. Rev Saude Publica. 2014;48(1):94-102. DOI:10.1590/S0034-8910.2014048004822
The address and first year of operation of 10 SCS specialized in AIDS and included in the institutional support network for the disease in Ceara, Northeastern Brazil, were taken from the Cadastro Nacional de Estabelecimentos de Saúde(CNES – National Registry of Health Facilities),b b Ministério da Saúde. Cadastro Nacional de Estabelecimentos de Saúde. Brasil: Cadastro Nacional de Estabelecimentos de Saúde; 2015 [cited 2015 May 2]. Available from: http:// http://cnes.datasus.gov.br/ which provides information regarding the health care network in the three spheres of government (municipal, state and federal). Thus, it was possible to georeference the services on a map built to include AIDS rates.
Each city was an analysis unit. The variables studied were the mean AIDS rates by municipality and the geographic location of the SCS. We used the geographical coordinates of addresses of institutions, and the code from the Brazilian Institute of Geography and Statistics (IBGE) referring to the city of residence of people who reported having the disease within the studied period.
The state of Ceara is located in the Northeastern Region of Brazil. This state is divided into seven mesoregions, comprising 184 cities spread over an area of approximately 148,825.6 km2. In 2012, its population was estimated at approximately 8.6 million inhabitants, with a population density of 57.8 inhab./km2 (Figure 1).a a Instituto de Pesquisa e Estratégia Econômica do Ceará. Ceará em números. Fortaleza: Instituto de Pesquisa e Estratégia Econômica do Ceará; 2014 [cited 2014 May 21]. Available from: http://www.ipece.ce.gov.br/
Map of the cities and mesoregions of the state of Ceara, according to the 2010 demographic census. Northeastern Brazil, 2014.
The evaluation included 7,896 individuals diagnosed with AIDS, aged 13 years or older, who lived in Ceara, and had been informed of their condition between 2001 and 2011, based on records from the Sistema de Informação de Agravos de Notificação (SINAN – Notifiable Diseases Information System).c c DATASUS. Ministério da Saúde. Sistema de Informação de Agravos de Notificação. Brasil: Sistema de Informação de Agravos de Notificação; 2012 [cited 2012 May 2]. Available from: http://www2.datasus.gov.br/ Duplicate cases and repeated notifications were excluded.
The mean rate of AIDS per city was calculated for the 2001-2006 and 2007-2011 periods. In the first period, the mean number of cases and the mean population were respectively obtained through the total number of cases between 2001 and 2006 and through the total added population in those six years, and both totals were then divided by six. In the second period (a five-year period), the mean number of cases and the mean population were obtained by dividing the totals by five. The AIDS rate in each period represents the mean number of cases divided by the mean population, multiplied by 100,000 inhabitants.
The global Moran's index was also used, regarding the mean rate, to test for the existence of spatial autocorrelation. This index, whose calculation tests whether surrounding areas differ from what would be expected in a pattern of complete spatial randomness, gives values ranging from -1 to +1. Spatial aggregation is expressed for positive values, while inverse autocorrelation expresses negative values; spatial autocorrelation is absent when its value tends to zero.1616 Silva DCC, Lourenço RW, Cordeiro RC, Cordeiro MRD. Análise da relação entre a distribuição espacial das morbidades por obesidade e hipertensão arterial para o estado de São Paulo, Brasil, de 2000 a 2010. Cienc Saude Coletiva. 2014;19(6):1709-19. DOI:10.1590/1413-81232014196.15002013
The presence of spatial aggregates was evaluated by the local Moran's index (Local Indicators of Spatial Association – LISA) and can be seen on the LisaMap. This index makes it possible to identify spatial dependence and quantify the degree of spatial association at each location of the sample set. The values of significance are divided into four groups: non-significant, with a 95.0% significance, with a 99.0% significance, and with a 99.9% significance.1414 Santos L, Raia Junior AA. Análise espacial de dados geográficos: a utilização da Exploratory Spatial Data Analysis – ESDA para identificação de áreas críticas de acidentes de trânsito no Município de São Carlos (SP).Soc Natur. 2006;18(35):97-107.
The BoxMap was used to graphically visualize a Moran scatter plot, which divides the area into quadrants with specific characteristics. The areas located in quadrants Q1 (High-High) and Q2 (Low-Low) have positive spatial autocorrelation, meaning that these are cities with AIDS rates similar to their neighbors, characterizing spatial aggregates. Quadrants Q3 (High-Low) and Q4 (Low-High) have negative spatial autocorrelation, which represents cities that have disparate disease rates compared with nearby cities.1414 Santos L, Raia Junior AA. Análise espacial de dados geográficos: a utilização da Exploratory Spatial Data Analysis – ESDA para identificação de áreas críticas de acidentes de trânsito no Município de São Carlos (SP).Soc Natur. 2006;18(35):97-107.
To describe the areas under the influence of the SCS, a Voronoi diagram was built based on the points formed by the geographical coordinates of each institution's address, distributed over the two study periods. This diagram makes it possible to define regions associated with each individual point on a map, rather than segmenting a geographical area into legally defined boundaries, whose polygons are divided in the space according to points, events, or both.77 Duczmal LH, Moreira GJP, Burgarelli D, Takahashi RHC, Magalhães FCO, Bodevan EC. Voronoi distance based prospective space-time scans for point data sets: a dengue fever cluster analysis in a southeast Brazilian town.Int J Health Geogr. 2011;10(29). DOI:10.1186/1476-072X-10-29 This approach, which is useful in epidemiological research, enabled clusters of points to be detected in a given space and time.1313 Rodrigues M, Bonfim C, Portugal JL, Gurgel IGD, Medeiros Z. Using spatial analysis to identify areas vulnerable to infant mortality. Rev Panam Salud Publica. 2013;34(1):36-40.
Maps were constructed for both periods, 2001 to 2006 and 2007 to 2011, along with the AIDS rates and the spatial distribution of the SCS. The state's available health facilities were analyzed to find whether they were distributed near areas with high concentrations of AIDS cases. QuantumGis® v.2.4.0 software was used.
This study is part of expanded research on the spatial distribution and social determinants of health in AIDS sufferers in the Brazilian state of Ceara, approved by the The Ethics Committee of the State Department of Health in Ceara (Protocol 203,911).
RESULTS
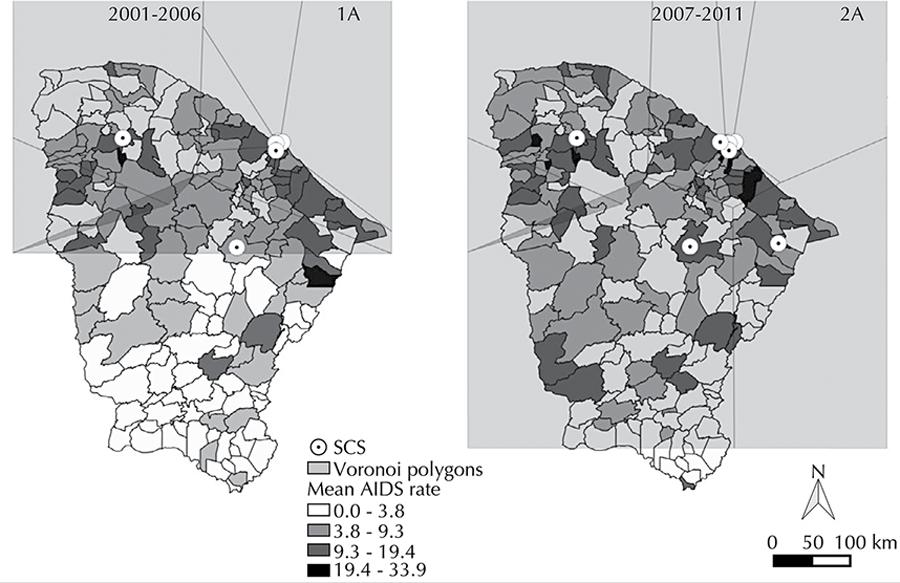
The distribution of AIDS throughout the two periods under study showed clusters of cases in the following regions: the capital of Ceara and its surroundings;Noroeste Cearense, next to the border with the state of Piaui; and north of the Jaguaribe city (Figure 2 - Maps 1A and 2A). Low concentrations were observed in the cities and neighboring areas of the central region and Sul Cearense.
Geographical distribution of Specialized Care Services (SCS), mean rates (maps 1A and 2A), BoxMap (maps 1B and 2B) and LisaMap (maps 1C and 2C) of the AIDS rates according to the Moran scatter plot, in the state of Ceara, Northeastern Brazil, 2001-2011.
Almost the entire Ceara coastline showed high rates of AIDS (Figure 2 - Maps 1A and 2A), and the relationship of cities neighboring the coastline had the same High-High pattern (BoxMap – Figure 2 - Maps 1B and 2B). We observed an expansion of the disease in the west of the state, upon comparing the first and the second period, with the highest amount of cities with the High-Low or Low-High standard. In turn, the LisaMap (Figure 2 – Maps 1C and 2C) shows that the AIDS rates and their spatial correlation with the neighboring regions in the 2001 to 2006 period are statistically significant in Fortaleza (state capital), as well as in part of the Metropolitan Region, in Sobral (central region of Noroeste Cearense) and in Sul Cearense. After the Lisa method was applied, significant growth was observed in cases of AIDS in the southwestern cities of the Sertões Cearenses (mesoregion in Ceara), which had previously not been affected by the disease. Between 2007 and 2011, there was a significant distribution of AIDS in as many cities as in the previous period, and still in the same regions (Metropolitan, Noroeste Cearense andSul Cearense).
While dealing with the distribution of SCS along with the distribution of AIDS in Ceara (Figure 2), eight institutions were observed being initially concentrated in Fortaleza, showing a statistically significant cluster of AIDS cases. However, areas such as the Sertões Cearense and south of Jaguaribe had clusters of the disease, but without any SCS nearby. In the second period, two more SCS opened: one in Fortaleza and other north of Jaguaribe, which is a location with high rates of the disease. However, there was only one SCS in the Noroeste Cearense, a region with significant clustering of cases, with no other service having been opened.
The Voronoi diagram, showing the distribution of the SCS (Figure 3), made it possible to observe that the services further away from state capital covered a larger geographical area. Between 2001 and 2006 (Figure 3 - Map 1A), the polygons referring to the SCS did not manage to cover the entire state's length, indicating possible locations that are a long way from the service. Over the 2007 to 2011 period (Figure 3 - Map 1A), the polygons covered almost all of Ceara. Furthermore, one polygon with no SCS was located in the western portion of the state.
Distribution of Specialized Care Services (SCS) and Voronoi polygons. Ceara, Northeastern Brazil, 2001-2011.
DISCUSSION
Despite the concentration of AIDS in the metropolitan area, the state of Ceara has clusters of the disease in other regions, such as north of Jaguaribe,Noroeste Cearense and west of the Sertões Cearenses, which were observed throughout the two periods under study. Regarding the spread of the epidemic away from major urban areas, access to health services impacts on the quality of life for people living with HIV/AIDS.55 Costa DL, Oliveira DC. Qualidade de vida de pessoas com vírus da imunodeficiência humana e a interiorização: avaliação multidimensional.Rev Enferm UFPE [Online]. 2013;7(10):5866-75. DOI:10.5205/reuol.4377-36619-1-ED.0710201305 Centralizing the specialized care services instead is confronted with the epidemic's geographic expansion, which places obstacles in front of the population living farthest away from having access to care, leaving them with less attention and priority.1111 Reis CT, Czeresnia D, Barcellos C, Tassinari WS. A interiorização da epidemia de HIV/AIDS e o fluxo intermunicipal de internação hospitalar na Zona da Mata, Minas Gerais, Brasil: uma análise espacial. Cad Saude Publica. 2008;24(6):1219-28. DOI:10.1590/S0102-311X2008000600003
The predominance of SCS and clusters of AIDS in the metropolitan region was also verified, which may influence the patients' accessibility to these services. There is a consensus that concentrating care in reference units can make it difficult for the patients to geographically access it, which is due to the traveling costs, time off work, among other factors. However, people who exhibit stigmatizing diseases, such as HIV/AIDS, prefer their homes to be far away from these units, as there is a wish to maintain anonymity and not to be recognized by other individuals who use the service.11 Arakawa T, Arcêncio RA, Scatolin BE, Scatena LM, Ruffino-Netto A, Villa TCS. Acessibilidade ao tratamento de tuberculose: avaliação de desempenho de serviços de saúde. Rev Latino-Am Enferm. 2011;19(4):1-9. DOI:10.1590/S0104-11692011000400019
Research indicates the disproportionate number of SCS in the northwest and west of the Sertões Cearenses in relation to AIDS rates, whose values are high. However, one SCS was created in Jaguaribe during the second period, which responded to the area's demand regarding care to be given to individuals living with HIV/AIDS.
The spatial distribution of the health units directly has a direct effect on geographical accessibility that, in the case of large distances, combined with time and lack of transport, hampers people in need of specialized care from receiving it.66 Cunha ABO, Vieira-da-Silva, LM. Acessibilidade aos serviços de saúde em um município do Estado da Bahia, Brasil, em gestão plena do sistema.Cad Saude Publica. 2010;26(4):725-37. DOI: 10.1590/S0102-311X2010000400015
Still, managers must decide to implement a health service based on demand. This demand can be monitored by various health information systems along with researchers, academic institutions, and users of the SUS,1919 Tamaki EM, Tanaka OY, Felisberto E, Alves CKA, Drumond Junior M, Bezerra LCA, Calvo MCM, Miranda AS. Metodologia de construção de um painel de indicadores para o monitoramento e a avaliação da gestão do SUS. Cienc Saude Coletiva. 2011;17(4):839-49. DOI:10.1590/S1413-81232012000400007 assisting in logistical planning and when looking to open new services. In Brazil, these systems are rarely used in smaller cities, which can lead to health services being implement in places of low demand, at the expense of areas that need more health units.99 Miranda AS, Carvalho ALB, Cavalcante CGCS. Subsídios sobre práticas de monitoramento e avaliação sobre gestão governamental em Secretarias Municipais de Saúde. Cienc Saude Coletiva. 2012;17(4):913-20. DOI:10.1590/S1413-81232012000400013
The Centro-Sul Cearense did not have any SCS. The distance between the smaller cities and the major urban centers, where the SCS are concentrated, makes access to resources provided by these services difficult for many. As a result, people become more vulnerable to the disease's consequences, a challenge for advances against this epidemic.11 Arakawa T, Arcêncio RA, Scatolin BE, Scatena LM, Ruffino-Netto A, Villa TCS. Acessibilidade ao tratamento de tuberculose: avaliação de desempenho de serviços de saúde. Rev Latino-Am Enferm. 2011;19(4):1-9. DOI:10.1590/S0104-11692011000400019
This study is limited by the absence of similar research, making it difficult to challenge data obtained with this situation at other locations. It was not possible to find information on the minimum number of SCS recommended based on the population size or number of people living with HIV/AIDS, which makes wider analysis on service availability in the state difficult.
Studies that have a qualitative approach to understand the social and behavioral dynamics of the individual/SCS ratio is required, which could broaden the understanding of these distances or proximities with support services.
Further information regarding the AIDS epidemic is still required to make geoprocessing and spatial analysis feasible. In addition, it is necessary that the information generated through the research must reach health care institutions and policy makers so that the reality encapsulated by the studies can be changed.1717 Silva JM, Silva CBC. HIV/aids e violência: da opressão que cala à participação que acolhe e potencializa. Saude Soc. 2011;20(3):635-46. DOI:10.1590/S0104-12902011000300010
This study showed that the countryside regions of Ceara have areas with both high rates of AIDS and low numbers of SCS, and the reverse, regarding areas that were chosen to open new services, such as those areas that benefited during the second period under study. Basic health care can contribute for helping these patients, as accessibility to it is greater, which saves the secondary and tertiary institutions for more complex situations.
Methodological resources could be expanded, based on the idea that SCS interfere with the health-disease process of people living with HIV/AIDS, because they provide help during health care activities, as well as the prevention and treatment of these patients.
REFERENCES
-
1Arakawa T, Arcêncio RA, Scatolin BE, Scatena LM, Ruffino-Netto A, Villa TCS. Acessibilidade ao tratamento de tuberculose: avaliação de desempenho de serviços de saúde. Rev Latino-Am Enferm 2011;19(4):1-9. DOI:10.1590/S0104-11692011000400019
-
2Borges MJL, Sampaio AS, Gurgel IGD. Trabalho em equipe e interdisciplinaridade: desafios para a efetivação da integralidade na assistência ambulatorial às pessoas vivendo com HIV/aids em Pernambuco.Cienc Saude Coletiva 2012;17(1):147-56. DOI:10.1590/S1413-81232012000100017
-
3Barcellos C, Zaluar A. Homicídios e disputas territoriais nas favelas do Rio de Janeiro. Rev Saude Publica 2014;48(1):94-102. DOI:10.1590/S0034-8910.2014048004822
-
4Canesqui AM, Barsaglini RA. Apoio social e saúde: pontos de vista das ciências sociais e humanas. Cienc Saude Coletiva 2012;17(5):1103-14. DOI:10.1590/S1413-81232012000500002
-
5Costa DL, Oliveira DC. Qualidade de vida de pessoas com vírus da imunodeficiência humana e a interiorização: avaliação multidimensional.Rev Enferm UFPE [Online]. 2013;7(10):5866-75. DOI:10.5205/reuol.4377-36619-1-ED.0710201305
-
6Cunha ABO, Vieira-da-Silva, LM. Acessibilidade aos serviços de saúde em um município do Estado da Bahia, Brasil, em gestão plena do sistema.Cad Saude Publica 2010;26(4):725-37. DOI: 10.1590/S0102-311X2010000400015
-
7Duczmal LH, Moreira GJP, Burgarelli D, Takahashi RHC, Magalhães FCO, Bodevan EC. Voronoi distance based prospective space-time scans for point data sets: a dengue fever cluster analysis in a southeast Brazilian town.Int J Health Geogr 2011;10(29). DOI:10.1186/1476-072X-10-29
-
8Lima ICV, Galvao MTG, Paiva SS, Brito DMS. Ações de promoção da saúde em serviço de assistência ambulatorial especializada em HIV/Aids.Cienc Cuid Saude 2011;10(3):556-63. DOI:10.4025/cienccuidsaude.v10i3.13193
-
9Miranda AS, Carvalho ALB, Cavalcante CGCS. Subsídios sobre práticas de monitoramento e avaliação sobre gestão governamental em Secretarias Municipais de Saúde. Cienc Saude Coletiva 2012;17(4):913-20. DOI:10.1590/S1413-81232012000400013
-
10Nogueira JA, Silva AO, Sá LR, Almeida SA, Monroe AA, Villa TCS. AIDS in adults 50 years of age and over: characteristics, trends and spatial distribution of the risk. Rev Latino-Am Enfermagem 2014;22(3):355-63. DOI:10.1590/0104-1169.3327.2424
-
11Reis CT, Czeresnia D, Barcellos C, Tassinari WS. A interiorização da epidemia de HIV/AIDS e o fluxo intermunicipal de internação hospitalar na Zona da Mata, Minas Gerais, Brasil: uma análise espacial. Cad Saude Publica 2008;24(6):1219-28. DOI:10.1590/S0102-311X2008000600003
-
12Renesto HMF, Falbo AR, Souza E, Vasconcelos MG. Enfrentamento e percepção da mulher em relação à infecção pelo HIV. Rev Saude Publica 2014;48(1):36-42. DOI:10.1590/S0034-8910.2014048003186
-
13Rodrigues M, Bonfim C, Portugal JL, Gurgel IGD, Medeiros Z. Using spatial analysis to identify areas vulnerable to infant mortality. Rev Panam Salud Publica 2013;34(1):36-40.
-
14Santos L, Raia Junior AA. Análise espacial de dados geográficos: a utilização da Exploratory Spatial Data Analysis – ESDA para identificação de áreas críticas de acidentes de trânsito no Município de São Carlos (SP).Soc Natur 2006;18(35):97-107.
-
15Schilkowsky LB, Portela MC, SA MC. Fatores associados ao abandono de acompanhamento ambulatorial em um serviço de assistência especializada em HIV/aids na cidade do Rio de Janeiro, RJ. Rev Bras Epidemiol 2011;14(2):187-97. DOI:10.1590/S1415-790X2011000200001
-
16Silva DCC, Lourenço RW, Cordeiro RC, Cordeiro MRD. Análise da relação entre a distribuição espacial das morbidades por obesidade e hipertensão arterial para o estado de São Paulo, Brasil, de 2000 a 2010. Cienc Saude Coletiva 2014;19(6):1709-19. DOI:10.1590/1413-81232014196.15002013
-
17Silva JM, Silva CBC. HIV/aids e violência: da opressão que cala à participação que acolhe e potencializa. Saude Soc 2011;20(3):635-46. DOI:10.1590/S0104-12902011000300010
-
18Stephan C, Henn CA, Donalisio MR. Expressão geográfica da epidemia de aids em Campinas, São Paulo, de 1980 a 2005. Rev Saude Publica 2010;44(5):812-9. DOI:10.1590/S0034-89102010005000035
-
19Tamaki EM, Tanaka OY, Felisberto E, Alves CKA, Drumond Junior M, Bezerra LCA, Calvo MCM, Miranda AS. Metodologia de construção de um painel de indicadores para o monitoramento e a avaliação da gestão do SUS. Cienc Saude Coletiva 2011;17(4):839-49. DOI:10.1590/S1413-81232012000400007
-
20Yao J, Murray T. Locational effectiveness of clinics providing sexual and reproductive health services to women in rural Mozambique.Int Reg Sci Rev 2014;37(2):172-93. DOI:10.1177/0160017614524227
-
a
Instituto de Pesquisa e Estratégia Econômica do Ceará. Ceará em números. Fortaleza: Instituto de Pesquisa e Estratégia Econômica do Ceará; 2014 [cited 2014 May 21]. Available from: http://www.ipece.ce.gov.br/
-
b
Ministério da Saúde. Cadastro Nacional de Estabelecimentos de Saúde. Brasil: Cadastro Nacional de Estabelecimentos de Saúde; 2015 [cited 2015 May 2]. Available from: http:// http://cnes.datasus.gov.br/
-
c
DATASUS. Ministério da Saúde. Sistema de Informação de Agravos de Notificação. Brasil: Sistema de Informação de Agravos de Notificação; 2012 [cited 2012 May 2]. Available from: http://www2.datasus.gov.br/
-
Based on the doctoral thesis by Simone de Sousa Paiva, titled: "Distribuição espacial e determinantes sociais de saúde na população com aids do Ceará", presented at the Graduate Program in Nursing at the Universidade Federal do Ceará, in 2013.
-
Research funded by the Conselho Nacional de Pesquisa (CNPq – Process 303130/2013-0) and by the Fundação Cearense de Apoio ao Desenvolvimento Científico e Tecnológico (FUNCAP – Process PNP-0058-00121.01.00/11).
Publication Dates
-
Publication in this collection
2015
History
-
Received
1 Dec 2014 -
Accepted
28 June 2015