Abstract:
In this paper we analyze the visual cultures surrounding HIV and AIDS; we are especially interested in tracking the actors, discourses and visual cultures involved in AIDS prevention in Mexico for a period of twenty years: from 1985 to 2005. We use media studies to better comprehend how HIV and AIDS further medicalized human bodies by mobilizing specific discourses, metaphors and visual resources that, though promoting a better understanding of how HIV could be acquired and how it could be prevented, also generated new representations of sexuality, bodies and persons living with HIV or AIDS often biased in favor of different systems of value. Moreover, we try to offer a general characterization of the different publics that were targeted and preconceptions involving ethnicity, gender, sexual orientation, geography and membership in different sociocultural groups.
Keywords:
HIV; AIDS; Medicalization; Media Studies; Visual Cultures
Resumen:
En este artículo analizamos las culturas visuales acerca del VIH y el SIDA, con particular interés en la identificación de actores, discursos y culturas visuales involucradas en la prevención del in SIDA en México a lo largo de veinte años (desde 1985 hasta 2005). Nuestro propósito fue aplicar las herramientas de los estudios sobre medios para comprender como han sido medicalizados los cuerpos humanos a través de la movilización de discursos específicos, metáforas y recursos visuales que, a pesar promover una mejor comprensión sobre como el VIH puede ser adquirido y prevenido, también generó nuevas representaciones sobre la sexualidad, los cuerpos y las personas viviendo con VIH o SIDA a favor de diferentes sistemas de valores. Además, presentamos una caracterización general de los diferentes públicos que fueron blancos de los materiales analizados, y como éstos producen significados en términos de prejuicios de género, etnicidad, orientación sexual, geografía y pertenencia a diferentes grupos socioculturales.
Palabras clave:
VIH; SIDA; Medicalización; Estudios de Medios; Culturas Visuales
Resumo:
O artigo analisa as culturas visuais acerca do HIV e da AIDS focando na identificação de atores, discursos e culturas visuais envolvidas na prevenção da AIDS no México ao longo de vinte anos (desde 1985 até 2005). Nosso intuito foi aplicar as ferramentas dos estudos sobre mídia para compreender como os corpos humanos tem sido medicalizados através da mobilização de discursos específicos, metáforas e recursos visuais que, embora promova uma melhor compreensão sobre como o HIV pode ser adquirido e prevenido, também gerou novas representações sobre a sexualidade, os corpos e as pessoas vivendo com HIV ou AIDS em favor de diferentes sistemas de valores. Além disso, apresentamos uma caracterização geral dos diferentes públicos que foram alvo dos materiais analisados, e como estes produzem significados relativos a preconceitos de gênero, etnicidade, orientação sexual, geografia e pertencimento a diferentes grupos socioculturais.
Palavras chave:
HIV; AIDS; Medicalização; Estudos de Mídia; Culturas Visuais
Introduction
The Human Immunodeficiency Virus (HIV) and its associated condition (the acquired immunodeficiency syndrome - AIDS) have a history that spans over four decades. However, few medical events have resonated so powerfully and globally in such a short amount of time, caused not only by the particular etiology of the infection, but also by deep implications outside of medicine. HIV has entered in social, economic, political and cultural fields; it has rearranged and created a diverse set of relationships on each one. As with any major shock, there is no possibility of reverting to old positions, no matter how much our understanding and control of it has increased.
In the present paper, we analyze one specific effect of this so-called pandemic: the construction of sociocultural entities such as bodies, subjects and publics1 1 These categories are not intended to be mutually exclusive. We recognize that subjects are embodied and that part of their coherence comes from introjected body images that circulate, among other means, through the media here examined. When these images are devised to address specific audiences we are thus facing publics. We elaborate further on this in section 4. . This specific effect is a complex one, as it combines the influx of creation -for example, the emergence of institutions dedicated specifically to HIV, or the category of the HIV-positive patient in itself- and modification, such as the changing perception of the groups labeled as “high-risk populations”, or the inevitable adaptation of foreign influences to national contexts.
To navigate some facets of this multi-layered assembly, we use two theoretical frameworks. The first framework is medicalization theory, which will help us to systematize the ways in which HIV and the context in which it occurs have affected each other’s medical dimensions. Against some views of medicalization which stress processes like disease-mongering (Szasz, 2007SZASZ, Thomas. 2007. The medicalization of everyday life. Syracuse, New York: Syracuse University Press.) or the absorption of non-medical issues into the jurisdiction of medicine (Conrad, 2007CONRAD, Peter. 2007. The medicalization of society: on the transformation of human conditions into treatable disorders. Baltimore, Maryland: Johns Hopkins University Press.), we consider that medicalization can be seen as any one of an indeterminate number of ways in which an entity can be medically considered. Even if our case in point, HIV, has from its inception been conceived as a medical issue, it has been medicalized and re-medicalized in very different ways throughout its history: from the first reports and changing conception of the etiology of HIV infection and its mode of action, the complex story of HIV has touched upon the medicalization of homosexuality (when the latter was structured as a high-risk group) and has absorbed biomedical practices of diagnosis and treatment. Most recently, the shifting medical focus has started to consider both treatment and pre-exposure prophylaxis (PrEP) as prevention (see Nguyen et al. 2011NGUYEN, Vinh-Kim, O’MALLEY, Jeffrey & PIRKLE, Catherine M. 2011. “Remedicalizing an epidemic: from HIV treatment as prevention to HIV treatment is prevention”. AIDS. Vol. 25, no. 11, p. 1435 for an analysis of this remedicalization), managing to include sex practices into medicalization even before there is any positive diagnosis. This shifting remedicalization is also, of course, dependent on geographical context: while in the United States the use of PrEP is on the rise (see Highleyman, 2016Highleyman, Liz (2016) PrEP use exceeds 79,000 in US pharmacy survey, but some groups lagging behind [On line]. NAM - aidsmap, Jul. 19th 2016. http://www.aidsmap.com/PrEP-use-exceeds-79000-in-US-pharmacy-survey-but-some-groups-lagging-behind/page/3072084/ [Accessed on 31.08.2016].
http://www.aidsmap.com/PrEP-use-exceeds-...
), in Latin America in general, and in Mexico in particular, the option of prophylaxis is all but invisible.
The second framework, media studies, will help us trace the characteristics of the different subjects that were constructed and perceived around the HIV pandemic. We have limited our analysis to a specific period of time (from 1985 to 2005), as we believe that this is a period of profound social change, especially in terms of communication and information. It is precisely a transition period in which printed informative media coexisted, but was not yet overpowered, by the “new media” of digital services and the massive scale of public participation that it brought about. The changing balance between public participation and authority-based knowledge that coincided with the increasing public awareness of the viral infection was decisive to model the different subjects, bodies, communities and audiences configured around HIV in Mexico. To begin exploring this dynamic social landscape, we focus on the printed archives of the Academic Center for the Remembrance of Our America (CAMENA, in Spanish).
After presenting a brief overview of HIV history in Mexico (section I), we describe our two theoretical tools: medicalization theory (section 2) and the analysis of visual cultures through media studies (section 3). We follow our analysis of the mentioned printed archive (section 4) with a discussion on the ways it reveals certain trends of subject construction (section 5) and with our concluding remarks (section 6).
1. A succinct history of HIV-AIDS in Mexico.
The history of HIV in Mexico is both epidemiological and political. It is the former because during the three decades since its first clinical manifestations, HIV has suffered a variety of transformations in its distribution and prevalence among different sectors of the Mexican population. For example, HIV is becoming a rural phenomenon even though it originally entered into Mexico through its urban population (Smallman, 2007SMALLMAN, Shawn. 2007. The AIDS Pandemic in Latin America. Chapel Hill: The University of North Carolina Press.). This certainly reflects a change in the dynamics of transmission of the virus, although it hasn’t shifted towards a predominance of transmission via heterosexual contact, as it has occurred in Sub-Saharan Africa in the early stages of the epidemic, where the prevalence derived from heterosexual transmission (2 millions) was far greater than that of MSM (men who have sex with men) transmission (0.4 million) (Chin et al., 1990CHIN, James, SATO, P.A. & MANN Jonathan, M. 1990. “Projections of HIV infections and AIDS cases to the year 2000”. World Health Organization Bulletin. Vol. 68, no. pp. 1 - 11.). This increasingly rural incidence stands in stark contrast to other Latin American countries, where most of the HIV-positive population is concentrated in major urban centers (UNAIDS, 2014UNAIDS. (2014). UNAIDS Outlook 2014. The Cities Report. [On line]. UNAIDS. Available at: Available at: http://www.unaids.org/sites/default/files/media_asset/JC2687_TheCitiesReport_en.pdf
. [ Accessed on 04.08.2015].
http://www.unaids.org/sites/default/file...
)
The history of AIDS in Mexico is also political because both HIV and AIDS cannot be understood without considering the sexual politics of Mexican culture in which machismo, marianismo and homophobia are more than characteristic. Furthermore, increased military presence, caused by Mexico’s current war on drugs and rising rates of crime and violence have reconfigured the epidemiological dynamics, as military deployment is a factor for the spreading of HIV to new regions (Smallman, 2007SMALLMAN, Shawn. 2007. The AIDS Pandemic in Latin America. Chapel Hill: The University of North Carolina Press.). Finally, its history is both epidemiological and political because, globally, Mexico is located between three regions in which the adult prevalence is higher -the U.S., some Caribbean countries and some Central American nations-; locally, the consequences of this can be seen most clearly by paying attention to migration flows and how these have modified the HIV & AIDS landscape in Mexico (Smallman, 2007).
More specifically, according to UNAIDS (2015aUNAIDS.(2015a). AIDS info. Indicators. [On line]. UNAIDS. Available at: Available at: http://aidsinfo.unaids.org/#
. [Accessed on 04.08.2015].
http://aidsinfo.unaids.org/#...
, 2015bUNAIDS. (2015b). Estimaciones sobre el VIH y el sida [On line]. UNAIDS. Available at: Available at: http://www.unaids.org/es/regionscountries/countries/mexico#
[Accessed on 23.07.2015].
http://www.unaids.org/es/regionscountrie...
), in 2014 Mexico had ca. 190,000 persons living with HIV and the incidence rate for the general population was of 0.02%. Of those 190,000, ca. 40,000 were women and 2,900 children. There were 6,000 HIV-related deaths with less than a hundred for children and over 5,000 in male adults. These numbers represent an improvement when compared to, for example, the incidence rate in 1990, which was 0.07% (UNAIDS, 2015a).
In other words, the prevalence in Mexico has declined since 1995 from 0.7% to the actual 0.2%. HIV-related deaths have also diminished, from 11,000 per year in 1990, 24,000 between 1999-2000, to the already mentioned 6,000 in 2014. Moreover, in 2014 there were only 7,500 new cases while in 1990 this number was around 34,000. Of this 7,500, less than one hundred were in children between 0-14 y.o. and ca. 5,900 in adult males (UNAIDS, 2015a).
Nonetheless, these worthy achievements have not altered the fact that this epidemic still mainly affects vulnerable groups composed of: (i) men who have sex with men (MSM), (ii) sex workers (SW) of any gender, (iii) people who inject drugs (IDUs), and (iv) persons serving sentences. Indeed, when we pay attention to MSM, in 2013, 73.1% of MSM reported using condom with their most recent sexual partner but only 47.5% underwent a test for HIV detection in the last 12 months. From an estimate of 911,852 men who engage in sex with men, ca. 17.3% are HIV positive (UNAIDS; 2015a).
In 2005, 95% of MSM reported undergoing a test for HIV in the last 12 months, with a prevalence of 20%, and condom use with the most recent sexual partner in anal sex of 73% (UNAIDS; 2015a). This means that, while the prevalence has also decreased in this segment, it has not decreased as significantly as the rate for the adult population in general; also, while the percentage of MSM who use condoms remains stable, testing has strongly decreased. For these reasons, at least for the time being, we think it justified to aim a larger number of prevention and detection media campaigns, and public health planning, to groups with greater prevalence. Of course, it must be done in a thoughtful manner, and media campaigns must work to avoid neglecting communication with Mexican society in general. As Elsa Fan (2014FAN, Elsa. 2014. “HIV testing as prevention among MSM in China: the business of scaling-up”. Global Public Health. Vol. 9, no. 1-2, pp. 85-97.) has shown in the case of China, MSM are still widely believed to be the highest-risk group, even though heterosexual transmission accounts for more than half of new infections.
A different scenario is found when we analyze sexual workers. In 2013, 86.8% of SW reported using condom with their last client and 78.2% underwent a test for HIV detection in the last 12 months. In 2014, of an estimated number of 237,798 sex workers, ca. 7% are considered HIV positive in comparison with 1.7% in 2009 (UNAIDS, 2015a). So, here, although the proportion of SW testing themselves and using condom is important, the prevalence has not decreased at all.
Also different is the situation for IDUs. In 2014 there were ca. 164,157 IDUs in Mexico according to UNAIDS. Data from 2013 suggest a prevalence rate of 2.5% and a percentage of 35% for those who tested themselves for HIV in the past 12 months. It is worth mentioning that 71.3% reported using sterile syringes. However, from 2013 to 2014 the coverage of health policies in charge of distributing sterile syringes diminished from 19.7% to 3.9%. But the prevalence has diminished, from 3.9% in 2005, 7.02% in 2011, to its actual value of ca. 2.5% (UNAIDS, 2015a).
In general, in 2014 97,402 HIV positive persons received antiretroviral therapies (ART), which represents only 50.2% coverage. Nevertheless, five years ago the coverage rate was about 32.4%. In principle, 5,400 HIV-related deaths are averted each year. However, the retention rate of those receiving ART descended from 91% in 2013 to 83% in 2014. Finally, mother to child transmission in 2014 seems to be better controlled with 1,181 of 1,400 (81.6%) HIV-positive mothers receiving antiretroviral therapies (UNAIDS, 2015aUNAIDS.(2015a). AIDS info. Indicators. [On line]. UNAIDS. Available at: Available at: http://aidsinfo.unaids.org/#
. [Accessed on 04.08.2015].
http://aidsinfo.unaids.org/#...
).
Mexico is the country with the second largest population of persons living with HIV in Latin America, only after Brazil (CENSIDA, 2009CENSIDA. (December, 2009). El VIH/SIDA en México 2009. [On line]. CENSIDA. Available at: Available at: http://www.censida.salud.gob.mx/descargas/2009/VIHSIDAenMexico2009.pdf
. [Accessed on 04.08.2015].
http://www.censida.salud.gob.mx/descarga...
); vulnerable groups show complex dynamics in which improvement is only partial and discrimination and poverty are still major obstacles. The actual prevalence and its behavior for the last thirty years, given Mexico’s geographic location and migration flows with three neighboring regions with higher rates - the U.S., the Caribbean and Central America with 0.6,%, 1.1% y 0.7-1%, respectively-, is also noteworthy. Indeed, Mexico’s prevalence is below Latin America’s average (0.4%); as a frame of reference, the highest prevalence in Latin America is in Guyana, with 2.5%, and the lowest is Nicaragua with 0.2% (CENSIDA; 2009).
Most likely, Mexico’s early response to AIDS, with the creation in 1983 of the Registro Nacional de Casos de SIDA, the creation in 1988 of the Consejo Nacional para la Prevención y Control del SIDA (CONASIDA), later -after 2001- Centro Nacional para la Prevención y Control del VIH/SIDA (CENSIDA), bespeak of some success regarding the management of this epidemic both at the level of prevention and control (Smallman, 2007SMALLMAN, Shawn. 2007. The AIDS Pandemic in Latin America. Chapel Hill: The University of North Carolina Press.). CENSIDA, for example, although part of the Ministry of Health, is a decentralized organ with its own budget and autonomy. Also, each of the 32 federal entities of Mexico has its equivalent to CENSIDA. These last point are specially relevant when judging public policy towards HIV and AIDS, reflected in the total spending on AIDS.
In 2008, of the total spending on AIDS, 23% was on prevention. These numbers rose to 25.7% in 2009 and 31.4% in 2011. Most of this budget is allocated to vulnerable groups such as MSM, SW -especially women- and IDUs. The emphasis on prevention campaigns centered on high-risk sexual activities reflects the data of HIV transmission: 94.1% of new infections occur through sexual intercourse and only 2.5% through blood transfusions, 1.3% through sharing non sterile syringes and 2.1% was perinatal (CENSIDA, 2011).
For 2011, Mexico’s spending was ca. USD 500 millions on AIDS, of which 480M came from domestic sources. In comparison, in 2005 it was only about 170M, in 2008, 260M and in 2009, 330M. Furthermore, if we follow UNAIDS National AIDS Spending Assessment (NASA) methodology, in 2011, Mexico’s Total Spending on AIDS was 0.94% of the National Spending on Health. 90.4% of this came from the Ministry of Health (30.9%) and the Social Services Institutions (42.1%) like the Instituto Mexicano del Seguro Social (IMSS), Instituto de Seguridad y Servicios Sociales para los Trabajadores del Estado (ISSSTE), Petroleos Mexicanos (PEMEX), or other branches of the government, for example States’ governments (16.6%). Only 7.3% came from private sources and 2.3% from international sources (CENSIDA, 2011CENSIDA. (2011). Medición del Gasto en SIDA: México 2010-2011. [On line]. CENSIDA-SSA. Available at: Available at: http://www.unaids.org/sites/default/files/en/media/unaids/contentassets/documents/data-and-analysis/tools/nasa/20141017/mexico_2010_11_es.pdf
. [Accessed on 04.08.2015].
http://www.unaids.org/sites/default/file...
).
This highlights that, regarding the HIV & AIDS epidemic, the role of government is fundamental. In comparison, the National Spending on Health in Mexico, for 2011, showed that 41.6% came from families’ sources, which means that families had to pay for their care with no social institution or government involved. Only 5% came from private sources (CENSIDA, 2011).
Prevention is central in the fight against AIDS. By 2009, CENSIDA funded 70 projects, most of them in Mexico City, the State of Mexico, Jalisco and Chiapas, all under the Estrategia Nacional de Prevención of the Federal Government. However, civil society organizations have so far also played an important role, not only in Mexico but globally (see, for example, Epstein, 1996EPSTEIN, Steve. 1996. Impure Science; AIDS, activism and the politics of knowledge. Berkeley: University of California Press.; Kippax, 2010KIPPAX, Susan. 2010. Reasserting the social in a biomedical epidemic: The case of HIV-Prevention. In Conference on
Reframing the Social Dimensions of HIV in a Biomedicalised Epidemic: The Case of Treatment as Prevention (Vol. 5).; Nguyen, 2007NGUYEN, Vinh-Kim. 2007. “Antiretroviral Globalism, Biopolitics, and Therapeutic Citizenship”. In ONG, Aihwa & COLLIER, Stephen J. Global Assemblages: Technology, Politics, and Ethics as Anthropological Problems. Oxford: Blackwell Publishing Ltd, Oxford, UK.); by 2011, CENSIDA had a census of 211 of these (CENSIDA, 2009). Their role is going to be fundamental to achieve the UNAIDS 2020 90-90-902
2
90% of those who have HIV know their status, 90% of those who know are in treatment and, finally, 90% of those in treatment exhibit a significant decrease in their viral loads.
and 2030 95-95-95 goals (UNAIDS, 2015cUNAIDS. (2015c). Understanding Fast Track. Ending the AIDS Epidemic by 2030. [On line]. UNAIDS. Available at: Available at: http://www.unaids.org/sites/default/files/media_asset/JC2686_WAD2014report_es.pdf
. [Accessed on 04.08.2015].
http://www.unaids.org/sites/default/file...
). It is essential to this paper the contents, language and imagery employed by these different agents, because they highlight the relevance of analyzing the situatedness of the intended targets (audiences or publics) and the organisms or institutions which generate the messages (NGOs, activists, the State, etc.).
It is thus important to study the different aspects of those media employed in raising awareness of the basics of the HIV & AIDS epidemic. In this paper we focus our efforts in analyzing traditional media such as pamphlets, triptychs, booklets and other easily distributable and inexpensive media. We are especially interested in addressing the questions of what is said about AIDS, how it is said, who is addressing and whom is addressed with these media.
Thus, our perspective is broadly intersectional because we are interested in understanding which publics are being considered in these media, who funds these media, and, also, how these publics are constructed in terms of: (i) gender, (ii) sexual orientation, (iii) ethnicity, (iv) age, (v) nationality, (vi) urban vs rural context, (vii) occupation, (viii) level of education, including scientific literacy, and (ix) membership in a vulnerable group. As we detail below (in section 3), we emphasize how the intersectionality comes into play when presenting fundamental information for prevention and treatment, such as modes of transmission, high-risk activities, diagnosis or treatment.
2. AIDS and the dimensions of medicalization.
Traditionally, medicalization has been thought of as a way of producing subjectivities, a mechanism deeply tied to social control practices sponsored by the State and, more recently, as a further example of the commodification of life under capitalism. Thus, it is not surprising that most of the sociological literature dedicated to this notion has centered on the biopolitical dimensions of medicalization or the way in which it works as a governmental technology.
There are, of course, more optimistic narratives in which medicalization is valued as a way of actually improving the life quality of citizens, resisting the temptation to present medicalization as over determining subjectivities and the categories of health/disease in favor of the interest of the State, the capital or a few transnational companies (e.g., Rose, 2009Rose, Nikolas 2009. The politics of life itself: Biomedicine, power, and subjectivity in the twenty-first century. New Jersey: Princeton University Press.).
The literature on AIDS and medicalization is, however, a good example of how to simultaneously pay attention to both aspects, the global and national institutions and the local persons that confront this epidemic. Steven Epstein’s Impure Science (1996EPSTEIN, Steve. 1996. Impure Science; AIDS, activism and the politics of knowledge. Berkeley: University of California Press.) serves as an early but still influential and valuable example. Epstein narrates the way in which HIV and AIDS became scientific and medical facts from the years of 1984 to 1987, although further controversies on the etiology of AIDS persisted well into the 1990s. Additionally, Epstein narrates how activists, mainly but not only gay and lesbian, confronted both the Federal Drug Administration (FDA) and the National Institutes of Health (NIHs) of the United States of America and fundamentally redrawn the very logic of trials for approving drugs such as AZT and other ART.
Indeed, it could be argued that the success of these activists led to a new relationship between the social and the biomedical aspects of AIDS that fundamentally changed how medicalization of people living with AIDS functioned. After these confrontations, it was clear that the medical establishment could not rely on its expertise and power to exert any kind of therapy or trial on those suffering from this disease. It comes as no surprise that since the mid-1990s the topic of human rights and the voice of those living with HIV and AIDS became such a central concern.
Nevertheless, the contours of the medicalization of AIDS are changing once more. The global economic crisis of 2008 has thrown the global actions against AIDS into a new dynamic in which biocapitalism is becoming a central force to reckon with (Nguyen et al., 2011NGUYEN, Vinh-Kim, O’MALLEY, Jeffrey & PIRKLE, Catherine M. 2011. “Remedicalizing an epidemic: from HIV treatment as prevention to HIV treatment is prevention”. AIDS. Vol. 25, no. 11, p. 1435). This can be seen in how the drugs employed in ART are becoming, once more, the privilege of a few rich countries in a reversal of the social activism processes described by Epstein (1996EPSTEIN, Steve. 1996. Impure Science; AIDS, activism and the politics of knowledge. Berkeley: University of California Press.).
Another concomitant but conceptually distinct trend within the literature of AIDS and medicalization is related to the debate between those who defend the approach known as “HIV treatment is prevention” and those who defend a different approach known as “prevention is treatment” (see, for example, Kippax, 2010KIPPAX, Susan. 2010. Reasserting the social in a biomedical epidemic: The case of HIV-Prevention. In Conference on Reframing the Social Dimensions of HIV in a Biomedicalised Epidemic: The Case of Treatment as Prevention (Vol. 5).; Nguyen, 2007NGUYEN, Vinh-Kim. 2007. “Antiretroviral Globalism, Biopolitics, and Therapeutic Citizenship”. In ONG, Aihwa & COLLIER, Stephen J. Global Assemblages: Technology, Politics, and Ethics as Anthropological Problems. Oxford: Blackwell Publishing Ltd, Oxford, UK.; Nguyen et al, 2011). Here, the debate hinges on the kind of public policies which better serve the aim of preventing new infections. For the former, ART and HAART are the right choice and, thus, these authors tend to defend an approach in which physicians play a major role. For the latter, this strategy is not sufficient and, hence, they highlight the relevance of attending to the concerns of activists and community leaders, on the one hand, and, on the other hand, betting for prevention strategies that pay attention to local values, the structure and functioning of communities and, finally, ways of intervening that are less relying on expensive drugs that commodify health.
In light of this, it could be said that the current medicalization of AIDS resembles what Clarke and collaborators (Clarke et al, 2003CLARKE, Adele E., SHIM, Janet K., MAMO Laura, FOSKET, Jennifer Ruth & FISHMAN Jennifer R. 2003. “Biomedicalization: Technoscientific Transformations of Health, Illness, and U.S. Biomedicine”. American Sociological Review. Vol. 68, no. 2, pp. 161-194.) have labeled as biomedicalization, this is, a new type of medicalization in which the role of capital in the commodifying of health is becoming increasingly clear. Additionally, in this new type of medicalization, the interest of companies tends to influence the design and implementation of public policies very much in line with the concerns of Nguyen (2007NGUYEN, Vinh-Kim. 2007. “Antiretroviral Globalism, Biopolitics, and Therapeutic Citizenship”. In ONG, Aihwa & COLLIER, Stephen J. Global Assemblages: Technology, Politics, and Ethics as Anthropological Problems. Oxford: Blackwell Publishing Ltd, Oxford, UK.).
Be this as it may, our interest is restricted to a previous moment (1985-2005), before the new trends above described. Indeed, it is not quite clear that Mexico is experiencing anything similar to the biocapitalization described by Nguyen, although, it seems to us, the discussion between the two prevention approaches seems to be very relevant. Our aim is to understand how different populations have been interpellated and how they have reacted and engaged with these knowledges, on the one hand, and, on the other, how should prevention work to be causally efficacious in diminishing the rate of new HIV infections.
Also, we are especially interested in one topic that has received few attention in these discussions, this is, how global or national institutions are able to communicate the knowledge on HIV or AIDS generated by science and medicine to different audiences. As Airhihenbuwa and Obregon (2000AIRHIHENBUWA, Collins & OBREGON, Rafael. 2000. “A Critical Assessment of Theories /Models Used in Health Communication for HIV/AIDS”. Journal of Health Communication, Vol. 5 (supplement), pp. 5-15.) have shown, different communicative models exist and these are connected with previous discussions regarding how the audiences are conceived: as a collective of individual and abstract subjects or as communities with their own values and culture.
Thus, we believe that paying attention to medicalization and media is central to understand how the global and the national are connected with the local. However, this also demands rethinking some fundamental ideas on how to understand medicalization, resisting linear understandings of how medicalization works or how the body is transformed into an object/subject of knowledge.
Four considerations of the processes of medicalization
Medicalization is a complex process. At first glance it may seem that it requires only a definition that is accepted by the majority of the medical community or sanctioned by a regulative institution, such as the different medical associations at local, national or global scale. However, this is far from the truth. As Conrad (2005CONRAD, Peter. 2005. “The shifting engines of medicalization”. Journal of Health and Social Behavior. Vol. 46, no. 1, pp. 3-14.) argues, there was an important shift which undermined the medical professional position as the only authority which could build the foundations of a newly medicalized area. There are new voices associated with different changes in the medical institution. New technologies and new expertise have emerged, closely followed by a relatively recent vision of the importance of cost control and cost efficiency.
Medicalization is not a linear process. In opposition to what is usually given as an account of the changing medical jurisdiction, there is no particular entity which becomes medicalized. Every object and every assembly is in itself an infinite field of potential medicalization. This means that every object or assembly can give endlessly new forms of relationship with medicine. This does not mean that every medical and clinical relationship is preformed and hidden inside each object; no sustained gaze can extract in any given moment the whole of the possibilities of medicalization. This, indeed, is a case of historical ontology (Hacking, 2002HACKING, Ian. 2002. Historical Ontology. Cambridge, Mass.: Harvard University Press.), because novel arrays of materiality have been summoned out of disjointed parts and have brought about new entities.
HIV infection itself has gone about a changing medicalization dynamic (see, for example, Epstein, 1996EPSTEIN, Steve. 1996. Impure Science; AIDS, activism and the politics of knowledge. Berkeley: University of California Press.; Kippax, 2010KIPPAX, Susan. 2010. Reasserting the social in a biomedical epidemic: The case of HIV-Prevention. In Conference on Reframing the Social Dimensions of HIV in a Biomedicalised Epidemic: The Case of Treatment as Prevention (Vol. 5).; Nguyen, 2007NGUYEN, Vinh-Kim. 2007. “Antiretroviral Globalism, Biopolitics, and Therapeutic Citizenship”. In ONG, Aihwa & COLLIER, Stephen J. Global Assemblages: Technology, Politics, and Ethics as Anthropological Problems. Oxford: Blackwell Publishing Ltd, Oxford, UK.). In its first stages of the 1970s, AIDS was seen as a factor starting an extended terminal care as the progression of the immune failure was witnessed with bafflement; then, in a somewhat quick succession, it was seen as a diagnostic mystery, as a virological medical challenge, as a lethal infection slowed down by a treatment ineffective in the long run, and as a manageable chronic condition with undesirable side effects. At the same time, HIV has disrupted the medical field from other conceptual fields, such as the economy of a high cost pandemic, the sparking and ingression of activist groups or the asymmetry of different national health care systems. The assertion that homosexuality is demedicalized or that HIV is medicalized in a univocal way is a myth, one vision among an undefined multiplicity of perspectives, albeit a hegemonic vision. It invisibilizes the spatial and temporal asymmetries that sprout from the nonlinearity of the medicalization process. We can also note that the shifting foci around HIV require that medicalization be conceptualized as something broader than the ingression into medical jurisdiction of aspects of life previously outside it; any given thing can be simultaneously medicalized in an undefined number of ways.
Medicalization has fuzzy edges. Clarke et al. (2003CLARKE, Adele E., SHIM, Janet K., MAMO Laura, FOSKET, Jennifer Ruth & FISHMAN Jennifer R. 2003. “Biomedicalization: Technoscientific Transformations of Health, Illness, and U.S. Biomedicine”. American Sociological Review. Vol. 68, no. 2, pp. 161-194.) have pointed out many of the issues presently discussed within the framework of biomedicalization. The concept of biomedicalization (a multisited, complex process of change in medicalization brought about by new developments in biomedicine) uses the notion of technoscience. This seems, at present, an unavoidable proposal: the large strides in biomedical diagnosis and treatment have changed the dynamics of medicine. But in turn it signals an overflowing of the medical jurisdiction into a broader set of practices, and in accordance to what they deem a postmodern movement, the process of medicalization becomes completely decentered. A real theoretical problem emerges: how are we to track and limit the movements of medical jurisdiction? With a decentered object, everything can be thought of as medicalized. Possibly this is the reason behind Peter Conrad’s reticence towards the expanded, decentered tone of Clarke et al (2003) conceptualization: they “create a concept that attempts to be so comprehensive and inclusive that the focus on medicalization is lost” (Conrad 2005, p. 5). Bearing in mind this nonlinear theorization, we adopt a multisited biomedicalization concept.
3. Methodology: On how to approach Visual Cultures through Media Studies.
As stated in the last section, the visual culture present in the materials of interest mediates between, on the one hand, the medical establishment, including the State, pharmaceutic companies, NGOs, supranational organizations like UNAIDS, etc., and, on the other, those persons that constitute the intended target of the prevention campaigns sponsored by the aforementioned agents.
Indeed, it could be argued that this mediality is of fundamental importance for modern governmentality practices (Rose et al, 2006ROSE, Nikolas, O’MALLEY, Pat and VALVERDE, Mariana. 2006. Governmentality.” Annual Review of Law and Social Science, Vol. 2, pp. 83-104.) in which populations are managed through expertise and knowledge embodied in specific institutions such as systems of health and education; this is so because a successful governmentality practice -and medicalization is clearly one- cannot afford to suffer communicative breakdowns that would nullify its capacity to mold populations.
The mediating nature of these materials are of interest for those scholars who wonder how the rationalities of the State and other actors are structured in order to interpellate the intended audiences. In a sense, this would make the study of these materials complimentary to a sociology of institutions or to more anthropologically or ethnographically oriented studies in which the foci of interest are, for example, the subpopulations that live with HIV or AIDS and how these cope and understand these phenomena.
Media Studies (MS) provides the conceptual and interpretive tools to develop such an analysis. Media Studies are, after all, an interdisciplinary field within social sciences and humanities. Their scope includes both massive media, like T.V., radio, cinema and the internet, on the one hand, and textual and symbolic productions of various forms, on the other; additionally, media studies’ tools can be deployed in any situation in which meaning and content are present, even if these were not intendedly produced by an author (Brennen, 2013BRENNEN, Bonnie S. 2013. Qualitative Research Methods for Media Studies. New York: Routledge.).
It is worth mentioning that MS focus on how meaning and content are created, communicated, transformed and received, in other words, in how meaning and content are mediated within our communicative practices (Brennen, 2013BRENNEN, Bonnie S. 2013. Qualitative Research Methods for Media Studies. New York: Routledge.). This brief description, nonetheless, runs the risk of suggesting that the very divide between content and form, meaning and medium, is in itself stable or given; but there is nothing further from the truth. Indeed, what is taken as content or meaning depends on how a message is decoded (see below) which in itself depends on criteria deeply entrenched within our communicative practices.
From this, it follows that meaning and content cannot be thought of as given or transcendental, as if anchored in the intentions and beliefs of an author. Hence, the central locus of analysis in MS is mediality per se, i.e., the continuous production and de/stabilization of meaning and content understood as phenomena grounded in communicative practices.
However, this should not be understood as if the material underpinnings of communication were not important and our target of analysis were restricted to communicative actions. On the contrary, paying attention to the material supports of our practices reveals both how matter constrains meanings -not all media are equally apt to transform, store, de/stabilize or simply communicate any meaning or content- and, also, how matter comes to be organized in material cultures that already store meaning and, thus, conditions the communicative process (Brennen, 2013BRENNEN, Bonnie S. 2013. Qualitative Research Methods for Media Studies. New York: Routledge.; see also Hentschel, 2014HENTSCHEL, Klaus. 2014. Visual Cultures in Science and Technology. A Comparative History. Oxford: Oxford University Press.).
Obviously, actions do figure within our communicative practices and, although there is no consensus regarding how best to model these interactions -for example, in terms of networks or in terms of dyads of an addresser and an addressee- or the context that serves as a common background of conventionalized rules of interpretation, there are a number of elements originally developed within cultural studies that might be important to highlight.
The backgrounds of the addresser and addressee might not totally overlap which might give rise to different understandings of an identical action, expression or icon. Thus, it is important to keep in mind the non transcendental dimension of content and meaning and recognize the very possibility of a breakdown in communication when different interpretations are given to the “same” phenomenon.
Following Hall (2012HALL, Stuart. 2012. “Encoding/Decoding”. In DURHAM, Meenakshi and Douglas KELLNER (eds.) Media and Cultural Studies. Keyworks (pp. 137-144). Oxford: Wiley-Blackwell.), we argue that communicative actions are better described in terms of practices of encoding and decoding messages in which the code encompasses the hermeneutic dimensions of meaning, more specifically, the common background given by the large intertextual and interdiscursive network of meaningful signs in which sense is partially given by their anaphoric uses. This, nevertheless, does not preclude developing metaphoric uses but these will depend on the projectibility of the anaphoric uses into new realms of meaning, which might allow for the development of new -cataphoric- senses, emphasizing the agency of both addresser and addressee.
In this particular text our focus is in the Visual Cultures (VC) regarding HIV & AIDS and its prevention. By VC we mean those symbolic elements in the prevention practices that take the form of visual media like triptychs, pamphlets or booklets. VC have already been investigated in, for example, history of biology and medicine (e.g., Hentschel, 2014HENTSCHEL, Klaus. 2014. Visual Cultures in Science and Technology. A Comparative History. Oxford: Oxford University Press.). What we have learned from these studies is that images strongly structure the comprehension -social and/or causal- of particular phenomena. Indeed, they not only serve as tools for popularizing knowledge but are also central elements in research, given their capacity to mold the very heuristics employed by researchers.
Obviously, in our particular case, we are interested in how information might be presented through imagistic and textual elements; this requires distinguishing between information presented in terms of: (i) words, (ii) symbolic imagery or, (iii) a combination of both -including emblems. Regarding the content, we are especially interested in detecting constative/declarative elements that transmit knowledge, interrogative elements that might generate introspective attitudes and self-evaluative behaviors, imperative (conditional or unconditional) elements that mandate some particular response or behavior from the addressee and, finally, performative elements that inform the addressee his/her membership into particular groups and, thus, create publics.
Hence, our aim is to pay attention to both material and symbolic aspects -including linguistic and iconographic elements- within these media. For this reason, our method of analysis is qualitative and centered around textual analysis and semiotics. More specifically, we are interested in tracking who is the addresser and who the intended addressee, tracking as well how -and if- the intended public is intersectionally characterized (including its literacy) and, thus, differentiated in sub-publics. Finally, we are especially interested in how these media depict: (a) modes of transmission, (b) prevention practices, (c) human rights of those who live with HIV or AIDS, with special emphasis in the right of not being discriminated and having access to health services, (d) methods of diagnosis and the importance of undergoing regular testing, (e) information and accessibility of therapies, with special emphasis in ART, (f) the risks of opportunistic infections, and (g) information on hospitals and clinics able to provide medical attention.
There are two other important points to clarify in this methodological section. On the one hand, we would like to explain why we have chosen to analyze the archive “FONDO I”, Identidad, diversidad, disidencia y derechos sexuales (1936-2011) -Identity, diversity, dissidence and sexual rights (1936-2011)- that belongs to the Centro Académico de la Memoria de Nuestra América -Academic Center for the Remembrance of Our America- (CAMENA) of the Universidad Autónoma de la Ciudad de México -Autonomous University of Mexico City- (UACM). On the other, we would like to point out some limitations of our approach.
Regarding the first point, CAMENA became a fundamental archive in this study because it harbors the former archives of the Centro de Documentación y Archivo Histórico Lésbico “Nancy Cárdenas” -Center of Documentation and Historic Archive “Nancy Cárdenas”- (CDAHL) and the Centros de Documentación del Colectivo Sol, -Centers of Documentation of Colectivo Sol- (CIDHOM) and (CRISSOL), both of these given into custody to UACM. Hence, CAMENA harbors two of the most important archives of LGBT history in Mexico that are also public and easily accessible. We centered on the FONDO I, comprised of 56 boxes, half of which contain documents directly related to the topic of HIV and AIDS (see the last section of the present paper for a detailed list of the boxes analyzed). The CAMENA archive has already been analyzed in a previous publication dealing with homophobia in the 20th century (Guerrero Mc Manus, 2015GUERRERO MC MANUS, Fabrizzio. 2015. Ciencia y Contracultura: El Movimiento de Liberación Homosexual y sus Saberes. Ludus Vitalis, Vol. 23, No. 43, pp. 195-221.)
Furthermore, these archives were created by activists that were, by the 1980s and 1990s, organizing groups to inform and support against the HIV and AIDS epidemics (Guerrero Mc Manus, 2015). Thus, they offer a window to the kind of information that these groups collected and helped to spread. Moreover, the archive of Colectivo Sol that now belongs to CAMENA reflects how this group evolved from a prior gay-oriented agenda to a HIV-oriented one in which the concerns of HSH were obviously present but also the concerns of other groups such as SW, UID and a general audience. This of course is of vital importance to our aim of understanding mediality not only in terms of mediating contents/information but also of mediating between different sectors involved in the fight against HIV and AIDS.
Regarding the second point, given the nature of this archive, the media available to us cannot be judged in terms of their representativeness. However, we believe these media still allow us to track the historical transformations between 1985 to 2005.
Our discussion and analysis are thus preliminary because a complete understanding of the VC of HIV & AIDS will demand including ethno historical elements coming from physicians, activists, persons living with HIV and those in charge of designing and implementing public policy. Moreover, a sociological analysis of the field of public health and HIV comes to mind as a major contribution to our project. Nonetheless, we still believe our assessment of these media, as preliminary as it is, can bring light into the semiotic and textual strategies that were employed in the fight against HIV & AIDS in Mexico. Additionally, this might help us detect some problematic aspects in these media, for example, ideological biases or breakdowns in communication, and, hence, lead us to better communicative strategies.
4. Visual Cultures of AIDS prevention in Mexico from 1985 to 2005
We analyzed 206 items from the states of Baja California and Baja California Sur (24 items), Jalisco (21 items), Mexico city (81 items), Michoacán (10 items), Nuevo León (19 items) Oaxaca (23 items) as well as printed media published by CONASIDA, the national organism in charge of national prevention campaigns (28 items) -see Table 1 at the end of this section for a summary of the materials under discussion.
These items encompass a period of twenty years, from 1985 to 2005 and show how HIV & AIDS was thought of from the early responses to the epidemic to the early 2000s in a Mexico, after its so called democratic transition. These items also come from very different regions in Mexico, including major capitals, the northern states, one southern state and one central state.
We classified them according to these general guidelines. First, by State and year of production. Second, by the type of material it was. Here, we had three large groups: (i) one group composed of media in which written text is the main vehicle for transmitting information, (ii) a second group, in which written text and visual (more imagistic) elements play a part and, finally, (iii) mainly visual media. Then, third, we subdivided these items in terms of extension, in the case of group (i), and in terms of the intended use for the item, in case of group (iii). Hence, group (i) included booklets but also triptychs and handouts, group (ii) included comics and photonovels and, finally, group (iii) included postcards, condom-holders, cup holders and book markers. When the item was a very specific type of object, such as the program for a conference, we gave it a special category.
After doing this, we paid attention to who was the addresser and who was the intended target. When the intended target was an abstracted subject, with no further identities or social markers, we judged these items as directed towards a general audience, when, on the contrary, social markers or identities were identifiable, we assigned these items to specific audiences.
The addressers were in general NGOs, the ministries of health (local or national) or international organisms such as UNAIDS or WHO. The intended targets or publics were more or less the same and encompassed, ranked in order of recurrence: (i) the general public, (ii) men that have sex with other men (MSM), (iii) women, (iv) sex workers, (v) youths, (vi) people living with HIV-AIDS, (vii) travelers, (viii) physicians and nurses and, finally, (ix) those engaged in activism in favor of people living with HIV-AIDS.
In general, most handouts and triptychs employ a declarative language that presents information through an objective style deeply indebted to science and medicine. Images are absent or present only with aesthetic aims. Interrogative sentences are often titles and subtitles addressing aspects such as the etiology of AIDS, mechanisms of contagion or prevention, epidemiological facts, myths and realities, the symptomatology of AIDS and, lastly, centers of attention in which free diagnostics, counseling and drugs can be provided -see Image 1. These questions are immediately answered with a direct and impersonal prose.
Interestingly, all but one item have as their contents scientific facts about HIV & AIDS. There was one exception from Mexico City in which approaches from alternative medicine are discussed. Among these, we found bioenergetics, magnetotherapy, reflexology, naturist diets, etc. This one exception came from an NGO with the name “Movimiento de Salud en Defensa de la Vida”.
Regarding the content of these items, it is possible to document an evolution in terms of how vulnerable populations are described, on the one hand, and on the variety of strategies that might work as mechanisms of prevention, on the other. In the 1980s and early 1990s, homosexuals, bisexuals, drug users and sex workers are presented as “risk groups” and those items targeting the general public tend to encourage people to avoid having sex with members of these groups. From the late 1990s to the 2000s, the term “risk group” is abandoned in favor of “risk practice” or “vulnerable group” very much in concert with the rise of a deeper concern with the rights of those living with HIV or AIDS; at the same time, monogamy, abstinence and/or avoidance of those persons who are members of vulnerable groups are discarded as strategies of prevention in favor of mechanisms in which condom and protected sex play a more central role.
Only in the 2000s interrogative sentences with a different aim appear. These seek to promote a self-assessment in which one examines his or her own practices in order to decide if one should visit the physician or modify his or her behavior. What is more notable is not only this turn but also the inclusion of emotions as part of the assessment by focusing on how one might react to a positive result.
Metaphors are sometimes present in the context of making HIV and AIDS more understandable. For example, in one triptych from Oaxaca, AIDS is presented as a disease that does not respect class boundaries. To do this, an image of a king and pawn from a chess set is presented with the slogan “El SIDA no distingue entre reyes y peones” -AIDS does not distinguish between kings and pawns. Of course, these metaphors are not devoid of political signification. Donna Haraway (1991HARAWAY, Donna. 1991. “The biopolitics of postmodern bodies: constitutions of self in immune system discourse.” In Simians, cyborgs and women: The reinvention of Nature. (pp. 203-230) New York: Routledge.) cautions against military metaphors around the immune system in general, which serve to perpetuate an image of individuality across different historical moments (pp. 224-225); similarly, Paula Treichler’s earlier study of the “epidemic of signification” (1987TREICHLER, Paula, 1987. “AIDS, homophobia and biomedical discourse: an epidemic of signification”. Cultural Studies, Vol. 1, no. 3, pp. 263-305.) analyzes the different ways that HIV and AIDS metaphors can be used to put in motion specific, and often discriminatory agendas.
In those occasions in which images play a more central role, they tend to be illustrative or didactic and, in most cases, they explain in visual terms, step by step, how to put on a condom. Additionally, some of the visual explanations also offer a detailed account on how to dispose of a condom after use.
Furthermore, explaining how to use a condom usually comes hand in hand with drawings or cartoons in which condoms are anthropomorphized and depicted as friendly figures -or even superheroes- that seek to protect the user and his partners; alternatively, we might encounter representations in which using condoms in no way affects pleasure but it does offer an emotional assurance regarding safety. A third variation in this topic are those cases in which condoms become engulfing and protecting bubbles in which persons are embedded.
Moreover, some images seem to serve neither didactic nor decorative purpose: they seem to function by transmitting or promoting emotional responses of solidarity and hope. For example, we found numerous instances of drawings of (i) people holding hands or just hands being held, (ii) people hugging each other in large groups, (iii) thoughtful persons staring at the horizon, the sky or the sun and, (iv) finally, figures of authority, such as physicians, supporting patients.
In the early 1990s, some handouts or triptychs employed pictures of famous people -like soccer star Hugo Sánchez- or random but quite emblematic characters -like taxi drivers, see Image 2- with the aim of promoting a culture of safe sex, HIV testing and solidarity for all of those persons living with HIV/AIDS. The message sought to transmit the idea that HIV or AIDS were phenomena present in daily life and not a sort of “outer space” experience only affecting vulnerable persons.
Comics and photonovels were not common, most likely because they are expensive and require funding from the State (e.g. CENSIDA), International organisms like UNAIDS, philanthropic foundations (e.g. the MacArthur foundation), or the combination of resources from multiple NGOs. Nonetheless, these items seem to be much more interesting in terms of media analysis. They usually target a particular sector of the general public, for example MSM or straight men with multiple sexual partners. Discursively, they employ direct speech by literally giving voice to characters that represent members of the intended target.
Thus, comics and photonovels raise fears, concerns and questions by depicting situations that are common for those members of the intended group. They might, for example, represent situations in which putting on a condom might seem disruptive in a sexual encounter by interrupting the dynamics of foreplay. In these depictions, persons might be tempted to forgo a condom; here, comics and photonovels contrast the direct speech or thoughts of the character with a narrator or impersonal voice that offers relevant information that might change the decision of risky practices. Usually, characters realize this and act accordingly and we end up the comic by learning the moral of the story.
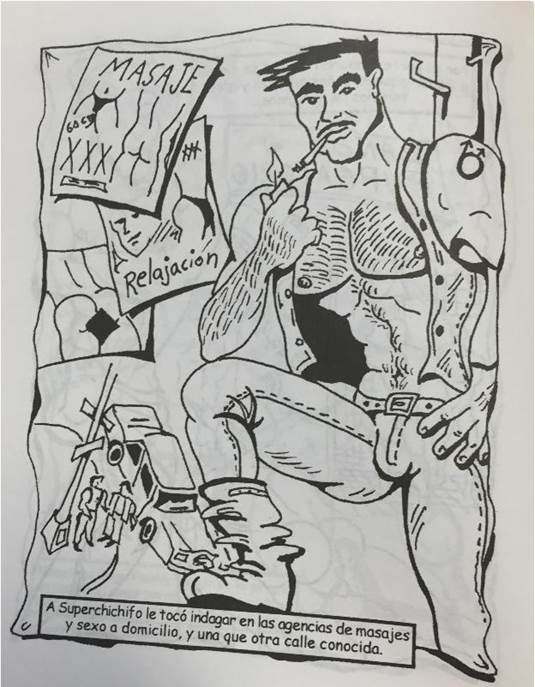
Comics and photonovels mobilize specific cultural resources by using slangs or everyday expressions instead of more medical or scientific terms, by employing particular aesthetics in the drawing of characters or their outfit in the case of photonovels or by presenting particular places like saunas, bars, hotels or events that might serve the role of spaces of socialization for specific publics -see Image 3. The stories are also written with the aim of engaging the reader and they are tailored to promote laughs, moments of deep identifications and, in general, a more introspective attitude regarding the practices in which one might be involved.
Furthermore, comics and photonovels can be more explicit in the depictions of the risk practices of specific audiences, especially sexual practices, without taking the chance of alienating the reader or promoting discriminatory responses or moral judgements. For example, comics targeting MSM illustrate practices such as anal sex, group sex, blow jobs and even “golden showers” or “water sports” -practices in which a partner urinates over another- and, thus, are able to discuss the risks involved in these. This specificity of target group may explain the direct and informal language, which contrasts with the more objective and neutral character of handouts that try to address a range of different audiences.
Something similar can be said of postcards, although there were postcards for a general audience, tend to be more neutral, and postcards for specific audiences, which work in a similar way as comics. For example, postcards intended for the youth employ superheroes to foster a culture of safe sex, HIV testing and AIDS prevention; curiously, these postcards usually promote safe sex by constructing a heroic masculinity in which using condoms makes males the heroes in the battle against HIV & AIDS.
We found a contrast between the items produced in Baja California and Baja California Sur and those from the rest of Mexico. In the first case, the influence of the United States was strong. For example, there were numerous handouts in English and with funding coming from California. Indeed, these items seem to target Latino populations and LGBT Latinos in southern California, and Mexicans and LGBT Mexicans living in the border, although there were a few intended for American teenagers crossing the border seeking sex and drugs.
Their bilingual character has much to do with the migration flows and the continuous border crossing. This not only brought English into the equation but also a racialized construction of the publics. We thus found numerous handouts in which there are persons from African descent but also Whites and Latinos. Paradoxically, race or ethnicity was fully absent from those items coming from other parts of Mexico, in which a stereotypical mestizo is always depicted.
In Baja California and Baja California Sur the forms of organizing civil society mirrored Californians from San Diego, Los Angeles or San Francisco, something explicitly stated in the handouts and triptychs themselves. For example, coalition groups were created as well as circles of mutual support.
Summary of the materials analyzed in this study. The 206 materials come from six Mexican states and federal campaigns by CONASIDA.
5. Constructing Publics and Medicalizing Bodies
A superficial analysis of the materials reveals the discussed shift in the discourse surrounding HIV and AIDS. Materials dated from the late 1980s and early 1990s strive to limit and identify “risk groups”: sex workers, MSM and intravenous drug users. The prevalent, unsaid idea was that these groups were easily defined by an essential trait, and as such composed the demographic fraction that was open to HIV infection. The choice of words that accompanied such presumptions was revealing: we found instances in which seropositive persons and their bodily fluids were referred to as “contaminated”. Documents that addressed health care workers, such as nurses or hospital staff that had to handle personal items that belonged to HIV patients were advised against emergency cardiopulmonary resuscitation procedures -especially mouth to mouth breathing- without special protection. Such discourses started shifting towards a less stigmatizing discourse in the mid-1990s: the different modes of virus transmission were better understood, and individuals were no longer labeled as carriers of contamination or even being contaminants themselves.
However, this is a well-trodden argumentative path, and it has been a subject of analysis. Prevention campaigns have been cast as being rooted on a foundation of homophobia. Thus, public health campaigns, albeit sometimes unwittingly, validated the popular notion of AIDS being a “gay disease”. The depiction of the AIDS epidemic that was put forth since its first manifestation thus modified and resonated with many overtones, which encompassed both the private and the public. Of course, official media related to HIV prevention does not serve the same purpose as control-driven propaganda. Although some medicalization theorists consider that the medical industry holds sway over society through disease-mongering, diagnosis construction and other ethically bankrupt practices (Szasz, 2007SZASZ, Thomas. 2007. The medicalization of everyday life. Syracuse, New York: Syracuse University Press.), many social characteristics of the last quarter of the 20th century prove that view somewhat unidimensional. It is important to stress that even when institutional mass media was a powerful source of social mobilization, it was certainly not the only one. Many activist movements became involved in the dissemination of knowledge about prevention, civil rights or treatment; in so doing, they prevented institutions such as the pharmaceutical or the healthcare industry from becaming the single source of information on HIV awareness.
In spite of all this, institutional HIV campaigns tend to be similar in tone and resources, as our archival analysis has revealed. With the exception of certain local preoccupations (for example, the bilingual materials in the northern state of Baja California), the information presented was almost exactly the same -sometime even repeated verbatim. This homogeneity of the printed mass media produced as health campaigns was justified as being an effort towards prevention. The depictions, whether drawings of photographs, most often represent and address seronegative people or, at least, people who identify as such, uncertain of their own status. The triptychs analyzed overflow with explanations of transmission pathways (mainly unprotected sex and intravenous drug use), demystification of other common activities such as sharing everyday utensils, kissing or hugging, explanations of acronyms and, less frequently, symptoms that could raise a flag for a possible HIV infection. Thus, the imagery used in these mass media products directly portray people who might be readily identified as not presenting any noticeable symptoms. Indeed, it is more common (but still, quite unusual) that HIV was represented as a personification of the disease, such as a schematic cartoon character clearly labeled as “AIDS” or a grotesque monster -this last image conflating both the fear of the pandemic and the perception of illness as an enemy; see Image 4.
This medical media, such as brochures, triptychs, postcards and posters, constructed a specific subject. The materials we analyzed appear to address a general public. Even when some groups are singled out, the information is cast as risk, and the initial infection of HIV is treated somehow as a primal event, a threshold beyond which the message no longer finds a receptor. If we are to take the medical media at face value, the initial HIV infection is a watershed event which separates the public at large with some unknown otherness. The information of public health systems was used as a tool of control for selective invisibilization. Still, the subject we are presently interested in -the HIV positive patient- hovers among the declarative insistence of the discourse of prevention and diagnosis, literally unseen. Even through absence we can discern a silhouetted image with its contours drawn by the image we do possess. In this way, we witness a construction that proceeds through a sort of via negationis, an apophatic way of making up people. The public to which the information is directed must infer the identity of the seropositive patient not through what is said, but through what is not.
First and most obviously, AIDS was presented as a result of a deviation, and campaigns were aimed to create safer practices in sexual and drug cultures. Even when it was stressed that anyone could carry the virus, information was mainly addressed to “high risk groups”, making it a disease that was connected to behavior perceived as morally condemned, such as sexual promiscuity or indulgence on illicit substances. Susan Sontag’s classic essay “AIDS and its metaphors” (1990SONTAG, Susan. 1990. Illness as metaphor and AIDS and its metaphors. New York: Picador.), speaks of the way that HIV infection was perceived as a stigmatization of the already stigmatized, a sort of punishment for people guilty of licentious hedonism. This is a theme that has been explored many times since, but the materials we analyze also show another demarcation. Even if they depict homosexual men engaging in (sometimes graphic) sex, the imagery is always centered in athletic, visibly healthy figures -see Image 5. Again, these figures are situated on the “prevention” side of the discourse, before they pass through the event of primary infection. Even in images directed to the gay community, AIDS is configured as something other than visually pleasing.
In spite of the visual absence of the HIV-positive subject in medical campaigns, the public at large was well aware of the wasting of the body that was readily associated with long-term HIV infection, immunosuppression, and side effects of some of the HAART medications. These fast bodily changes, especially those associated with lipodystrophy, were readily stigmatized. They were increasingly visible in the urban environments of Mexico, not only because seropositive cases were concentrated in large capitals, but also because of the international media focus on AIDS. In 1986, the World Press Photo of the Year award was granted to a picture of a man in a wheelchair, marked by lesions of Kaposi’s sarcoma. The photograph taken by Therese Frare, depicting the agony of AIDS activist David Kirby, became even more iconic: even though it was awarded 2nd prize of General News in the same contest after it was published in Life magazine, it was absorbed into a highly visible controversy as it was used by the clothing company Benetton as a campaign to raise awareness around HIV (Cosgrove, 2014Cosgrove, Ben. (2014). The Foto that Changed the Face of AIDS. [On line] LIFE Magazine, Nov. 25th 2014. http://time.com/3503000/behind-the-picture-the-photo-that-changed-the-face-of-aids/ [Accessed on 12.09.2015].
http://time.com/3503000/behind-the-pictu...
).
It is understandable that shocking images were deliberately purged from the medical printed media. Focusing on the graphic depiction of the most extreme cases of the disease can fuel the identification of the risk of infection with moral danger (Lupton, 1994LUPTON, Deborah. 1994. Moral threats and dangerous desires: AIDS in the news media. London: Taylor and Francis.). However, the via negationis portrayal of the seropositive patient in medical brochures compounded with the public visibility of AIDS when it was deemed to be an important international news item in the late 1980s and early 1990s (Gillett 2003GILLETT, James. 2003. “Media activism and internet use by people with HIV/AIDS”. Sociology of Health & Illness. Vol. 25 No. 6 pp. 608-624.). Both contradictory accounts (visually healthy people as the focus of prevention; activists and patients bearing visible stigmata) complemented each other in constructing a subject who had to go through defined stages: a newly diagnosed asymptomatic seropositive person, a patient visibly affected by the disease or by the side effects of medicine such as stavudine or zidovudine, and the person dying of total immune failure.
To be sure, there were individual persons that could fit into these descriptions. But the subject constructed stringed together these stages as superficial depictions of a much more complex social reality. The stages, indeed, are not a temporal sequence. In each individual case they can be simultaneous, overlapping and sometimes even reversed in order. An immune-depleted patient, who just received his or her diagnosis, could respond positively to the medications and regain a functional number of CD4 lymphocytes; cosmetic surgery was made available for the effects of lipodystrophy, and even today the threshold between HIV and AIDS is a fluid, constantly changing cell count number.
In the time span in which the archival materials of our analysis were produced, a stigmatized health condition was juxtaposed with limited representational possibilities for the expression of the population at large, with the journalistic media hype sparked by AIDS and with the less than optimal understanding of the virus. During this critical time, actual seropositive individuals lacked recognition in printed media, they were a constructed subject made out of voids and absences, a subject whose main characteristic was to be from the start the other. Their own particular situations were hidden away from the official accounts of societies: even the few instances of printed material that addresses the seropositive population do not touch upon the phenomenology of the illness, focusing instead on juridical or emotional advice for the moments immediately following the watershed event of receiving a HIV-positive diagnosis.
6. Concluding Remarks
The archives we studied span two decades of printed media committed to informing and promoting measures to control the growing HIV epidemics. In these twenty years, there has been at least two major shifts: from a period projecting a spotlight on the disease as a focus of media attention to a less “newsworthy topic of consideration” (Gillett 2003GILLETT, James. 2003. “Media activism and internet use by people with HIV/AIDS”. Sociology of Health & Illness. Vol. 25 No. 6 pp. 608-624., p. 609); and from a period in which communication was dominated by institutional printed media to the emergence of new digital media and community forums with the massification of message boards and forums on the internet. Even though each shift lacks a defined timeframe, they weighed in the changing discourse around HIV & AIDS.
In conclusion, we stress the importance of retrospective analyses of printed material, especially in light of the shifting understanding of the human immunodeficiency virus and its social effects. The relevance of a historical understanding is a pressing matter, for we may be witnessing yet another shift, yet another set of construction of subjects, practices, values and morals. HIV is no longer considered a death sentence by the society at large; the current treatments have proved effective to control viral load with minimum side effects. More importantly, medications such as the combined pill of emtricitabine and tenofovir (commercialized as Truvada) have proved effective in Pre-exposure Prophylaxis (PrEP). A 32 month study (Volk et al., 2015) reports no new infections among PrEP users, mostly MSM. These new practices add another dimension of the social dynamics of HIV, and are already finding their way into popular news sources and mass media (Peterson, 2014Peterson, Evan. (2014). The Case for PrEP or How I learned to Stop Worrying and Love HIV Positive Guys. [On line]. The Stranger, Nov. 12th 2014. http://www.thestranger.com/seattle/the-case-for-prep-or-how-i-learned-to-stop-worrying-and-love-hiv-positive-guys/Content?oid=20991643 [Accessed on 12.09.2015].
http://www.thestranger.com/seattle/the-c...
). These new therapies have been supported by some activist groups, but they have been denounced, even by some AIDS activist organizations, as a negative influence which would decrease safer sex practices, even calling it a “party drug” (Peterson, 2014). HIV is still a pressing public health issue, and it is our contention that prevention campaigns must attune with the new historical developments by acknowledging them, not by invisibilizing them through negative subjects, or casting them as a sign of moral laxity - yet again.
-
Resource documents:
-
FONDO I, Identidad, diversidad, disidencia y derechos sexuales (1936-2011):
-
Box 39 QVS63 Campañas del Consejo Nacional para el control y prevención del SIDA (CONASIDA). México.
-
Box 41 QVS80 Campañas para prevención del SIDA en Baja California y Baja California Sur.
-
Box 46 QVS108 Campañas para prevención del SIDA en Jalisco.
-
Box 46 QVS 111 Campañas para prevención del SIDA en la Ciudad de México y zona Metropolitana.
-
Box 47 QVS 116 Campañas para prevención del SIDA en Michoacán.
-
Box 47 QVS 120 Campañas para prevención del SIDA en Nuevo León.
-
Box 47 QVS 121 Campañas para prevención del SIDA en Oaxaca.

A triptych deploying informative, neutral imagery and information. Box 46 QVS111. Grupo de Apoyo de Personas Enlazadas contra el SIDA (GAPES), no date.


A brochure for prevention, using comic-book art style. Box 46 QVS111.Comic “La Liga de la Justicia Gay”. CONASIDA, no date.

A cartoon representing an anthropomophized virus as a metaphoric “enemy”. Box 46 QVS111. INEA-CONASIDA, 1991.

References:
- AIRHIHENBUWA, Collins & OBREGON, Rafael. 2000. “A Critical Assessment of Theories /Models Used in Health Communication for HIV/AIDS”. Journal of Health Communication, Vol. 5 (supplement), pp. 5-15.
- BRENNEN, Bonnie S. 2013. Qualitative Research Methods for Media Studies New York: Routledge.
- CHIN, James, SATO, P.A. & MANN Jonathan, M. 1990. “Projections of HIV infections and AIDS cases to the year 2000”. World Health Organization Bulletin Vol. 68, no. pp. 1 - 11.
- CLARKE, Adele E., SHIM, Janet K., MAMO Laura, FOSKET, Jennifer Ruth & FISHMAN Jennifer R. 2003. “Biomedicalization: Technoscientific Transformations of Health, Illness, and U.S. Biomedicine”. American Sociological Review Vol. 68, no. 2, pp. 161-194.
- CONRAD, Peter. 2005. “The shifting engines of medicalization”. Journal of Health and Social Behavior Vol. 46, no. 1, pp. 3-14.
- CONRAD, Peter. 2007. The medicalization of society: on the transformation of human conditions into treatable disorders Baltimore, Maryland: Johns Hopkins University Press.
- CONRAD, Peter, & SCHNEIDER, Joseph W. 1992. Deviance and medicalization: from badness to sickness Philadelphia: Temple University Press.
- EPSTEIN, Steve. 1996. Impure Science; AIDS, activism and the politics of knowledge Berkeley: University of California Press.
- FAN, Elsa. 2014. “HIV testing as prevention among MSM in China: the business of scaling-up”. Global Public Health Vol. 9, no. 1-2, pp. 85-97.
- GILLETT, James. 2003. “Media activism and internet use by people with HIV/AIDS”. Sociology of Health & Illness Vol. 25 No. 6 pp. 608-624.
- GUERRERO MC MANUS, Fabrizzio. 2015. Ciencia y Contracultura: El Movimiento de Liberación Homosexual y sus Saberes. Ludus Vitalis, Vol. 23, No. 43, pp. 195-221.
- HACKING, Ian. 2002. Historical Ontology Cambridge, Mass.: Harvard University Press.
- HALL, Stuart. 2012. “Encoding/Decoding”. In DURHAM, Meenakshi and Douglas KELLNER (eds.) Media and Cultural Studies. Keyworks (pp. 137-144). Oxford: Wiley-Blackwell.
- HARAWAY, Donna. 1991. “The biopolitics of postmodern bodies: constitutions of self in immune system discourse.” In Simians, cyborgs and women: The reinvention of Nature (pp. 203-230) New York: Routledge.
- HENTSCHEL, Klaus. 2014. Visual Cultures in Science and Technology. A Comparative History Oxford: Oxford University Press.
- KIPPAX, Susan. 2010. Reasserting the social in a biomedical epidemic: The case of HIV-Prevention. In Conference on Reframing the Social Dimensions of HIV in a Biomedicalised Epidemic: The Case of Treatment as Prevention (Vol. 5).
- LUPTON, Deborah. 1994. Moral threats and dangerous desires: AIDS in the news media London: Taylor and Francis.
- NGUYEN, Vinh-Kim. 2007. “Antiretroviral Globalism, Biopolitics, and Therapeutic Citizenship”. In ONG, Aihwa & COLLIER, Stephen J. Global Assemblages: Technology, Politics, and Ethics as Anthropological Problems Oxford: Blackwell Publishing Ltd, Oxford, UK.
- NGUYEN, Vinh-Kim, O’MALLEY, Jeffrey & PIRKLE, Catherine M. 2011. “Remedicalizing an epidemic: from HIV treatment as prevention to HIV treatment is prevention”. AIDS Vol. 25, no. 11, p. 1435
- Rose, Nikolas 2009. The politics of life itself: Biomedicine, power, and subjectivity in the twenty-first century New Jersey: Princeton University Press.
- ROSE, Nikolas, O’MALLEY, Pat and VALVERDE, Mariana. 2006. Governmentality.” Annual Review of Law and Social Science, Vol. 2, pp. 83-104.
- SMALLMAN, Shawn. 2007. The AIDS Pandemic in Latin America Chapel Hill: The University of North Carolina Press.
- SONTAG, Susan. 1990. Illness as metaphor and AIDS and its metaphors New York: Picador.
- SZASZ, Thomas. 2007. The medicalization of everyday life Syracuse, New York: Syracuse University Press.
- TREICHLER, Paula, 1987. “AIDS, homophobia and biomedical discourse: an epidemic of signification”. Cultural Studies, Vol. 1, no. 3, pp. 263-305.
- CENSIDA. (December, 2009). El VIH/SIDA en México 2009 [On line]. CENSIDA. Available at: Available at: http://www.censida.salud.gob.mx/descargas/2009/VIHSIDAenMexico2009.pdf [Accessed on 04.08.2015].
» http://www.censida.salud.gob.mx/descargas/2009/VIHSIDAenMexico2009.pdf - CENSIDA. (2011). Medición del Gasto en SIDA: México 2010-2011 [On line]. CENSIDA-SSA. Available at: Available at: http://www.unaids.org/sites/default/files/en/media/unaids/contentassets/documents/data-and-analysis/tools/nasa/20141017/mexico_2010_11_es.pdf [Accessed on 04.08.2015].
» http://www.unaids.org/sites/default/files/en/media/unaids/contentassets/documents/data-and-analysis/tools/nasa/20141017/mexico_2010_11_es.pdf - Cosgrove, Ben. (2014). The Foto that Changed the Face of AIDS [On line] LIFE Magazine, Nov. 25th 2014. http://time.com/3503000/behind-the-picture-the-photo-that-changed-the-face-of-aids/ [Accessed on 12.09.2015].
» http://time.com/3503000/behind-the-picture-the-photo-that-changed-the-face-of-aids/ - Highleyman, Liz (2016) PrEP use exceeds 79,000 in US pharmacy survey, but some groups lagging behind [On line]. NAM - aidsmap, Jul. 19th 2016. http://www.aidsmap.com/PrEP-use-exceeds-79000-in-US-pharmacy-survey-but-some-groups-lagging-behind/page/3072084/ [Accessed on 31.08.2016].
» http://www.aidsmap.com/PrEP-use-exceeds-79000-in-US-pharmacy-survey-but-some-groups-lagging-behind/page/3072084/ - Peterson, Evan. (2014). The Case for PrEP or How I learned to Stop Worrying and Love HIV Positive Guys [On line]. The Stranger, Nov. 12th 2014. http://www.thestranger.com/seattle/the-case-for-prep-or-how-i-learned-to-stop-worrying-and-love-hiv-positive-guys/Content?oid=20991643 [Accessed on 12.09.2015].
» http://www.thestranger.com/seattle/the-case-for-prep-or-how-i-learned-to-stop-worrying-and-love-hiv-positive-guys/Content?oid=20991643 - UNAIDS. (2014). UNAIDS Outlook 2014. The Cities Report [On line]. UNAIDS. Available at: Available at: http://www.unaids.org/sites/default/files/media_asset/JC2687_TheCitiesReport_en.pdf [ Accessed on 04.08.2015].
» http://www.unaids.org/sites/default/files/media_asset/JC2687_TheCitiesReport_en.pdf - UNAIDS.(2015a). AIDS info. Indicators [On line]. UNAIDS. Available at: Available at: http://aidsinfo.unaids.org/# [Accessed on 04.08.2015].
» http://aidsinfo.unaids.org/# - UNAIDS. (2015b). Estimaciones sobre el VIH y el sida [On line]. UNAIDS. Available at: Available at: http://www.unaids.org/es/regionscountries/countries/mexico# [Accessed on 23.07.2015].
» http://www.unaids.org/es/regionscountries/countries/mexico# - UNAIDS. (2015c). Understanding Fast Track. Ending the AIDS Epidemic by 2030 [On line]. UNAIDS. Available at: Available at: http://www.unaids.org/sites/default/files/media_asset/JC2686_WAD2014report_es.pdf [Accessed on 04.08.2015].
» http://www.unaids.org/sites/default/files/media_asset/JC2686_WAD2014report_es.pdf
-
1
These categories are not intended to be mutually exclusive. We recognize that subjects are embodied and that part of their coherence comes from introjected body images that circulate, among other means, through the media here examined. When these images are devised to address specific audiences we are thus facing publics. We elaborate further on this in section 4.
-
2
90% of those who have HIV know their status, 90% of those who know are in treatment and, finally, 90% of those in treatment exhibit a significant decrease in their viral loads.
Publication Dates
-
Publication in this collection
Dec 2016
History
-
Received
14 Sept 2015 -
Accepted
14 July 2016