Abstract
Introduction:
Diastasis of the rectus abdominis muscle (DRAM) is characterized by the separation of the rectus abdominis muscles beams, caused by enlargement of the linea alba, a common condition during pregnancy. Physical therapy has been shown necessary in women health, to help them adjust the physical changes throughout the pregnancy and puerperium.
Objectives:
To verify the DRAM prevalence in the immediate puerperium in a sample of women attended by the Unified Health System in Guarapuava, PR, Brazil, and investigate possible correlations between the DRAM presence and the delivery type, pregnancies number, maternal age, pregnancy type and weight gain during pregnancy.
Materials and Methods:
This is a transversal study, that included 88 samples of women in the immediately puerperium. It was realized a specific assessment and verified the DRAM presence and its measures. The checkpoints were in the umbilical, 4.5 cm above and below this point. It was considered present and relevant when there was any separation from the linea alba.
Results:
The study showed 61.36% DRAM prevalence. Its averages were 0.88 cm supra-umbilical, 1.23 cm umbilical and 0.3 cm infra-umbilical. Puerperium women who had DRAM, 31.5% were primiparous and 68.5% multiparous.
Conclusion:
The DRAM prevalence was considered high and relevant. The DRAM measure was higher in the umbilical region compared with infra and supra-umbilical. The multiparous women had a higher correlation with the DRAM than the primiparous.
Keywords:
Pregnancy; Diastasis of the rectus abdominis; Puerperium; Prevalence.
Resumo
Introdução:
Diástase do músculo reto abdominal (DRAM) caracteriza-se pela separação dos feixes do músculo reto abdominal, causada pelo alargamento da linha alba, condição comum durante a gestação. A fisioterapia tem se mostrado necessária na saúde da mulher, para auxiliá-las a se ajustarem às mudanças físicas do começo ao fim da gravidez e no puerpério.
Objetivos:
Verificar a prevalência de DMRA no puerpério imediato em uma amostra de mulheres atendidas pelo Sistema Único de Saúde no município de Guarapuava-PR, Brasil, e investigar possíveis relações entre a presença de DMRA e o número de gestações, tipo de gestação e ganho de peso durante a gestação.
Materiais e Métodos: Estudo transversal, que incluiu amostra de 88 mulheres no puerpério imediato. Foi realizada uma avaliação específica e verificada a presença de DRMA e suas medidas. Os pontos de medida foram na cicatriz umbilical e 4,5 cm acima e abaixo da mesma. Considerou-se presente e relevante quando houvesse qualquer afastamento da linha alba.
Resultados:
O estudo mostrou uma prevalência da DRAM de 61,36%. As médias de DRAM foram 0,88 cm supraumbilical, 1,23 cm umbilical e 0,3 cm infraumbilical. Das puérperas que apresentaram DRMA, 31,5% eram primíparas e 68,5% multíparas.
Conclusão:
A prevalência de DRMA foi considerada alta e relevante. A medida da DRMA foi maior na região umbilical quando comparada com infra e supra-umbilical. As mulheres multíparas tiveram maior correlação com a presença de DRMA que as primíparas.
Palavras-chave:
Gestação; Diástase do Musculo Reto Abdominal; Puerpério; Prevalência.
Introduction
During pregnancy many changes occur, both biomechanical and physiological in the woman's body 1Costa ES, Pinon GMB, Costa TS, Santos RCA, Nóbrega AR, Souza LB. Alterações fisiológicas na percepção de mulheres durante a gestação. Rev Rene. 2010; 11(2):86-93 .,2Mann L, Kleinpaul JF, Teixeira CS, Konopka CK. Dor Lombo Pélvica e exercício físico durante a gestação. FisioterMov. 2008; 21(2):99-105.. Changes in the mechanics of the locomotor system occur due to various factors such as weight gain, shift of the gravity center and the action of hormones, which increase the ligamentous laxity 3Marnach ML, Ramin KD, Ramsey PS, Song SW, Stensland JJ, An KN. Characterization of the relationship between joint laxity and maternal hormones in pregnancy. Obstet Gynecol. 2003; 101(2):331-5. and lead to alterations that cause structural changes in the static and dynamic of the body 4Birch K, Fowler NE, Rodacki AL, Rodacki CL. Stature loss and recovery in pregnant women with and without low back pain. Arch Phys Med Rehabil, 2003, 84(4):507-12.?. 2000 May; 82(5):625-32.. The body balance changes start to be more evident from the second trimester of pregnancy and, generally, remain a few weeks after giving birth 5Mann L, Kleinpaul JF, Mota CB, Santos SG. Alterações biomecânicas durante o período gestacional: uma revisão. Motriz: Rev Ed Fís. 2010; 16(3):730 - 41..
During pregnancy, the body undergoes major changes by the increase in weight of the uterus and the hormonal action of relaxin, progesterone and estrogen, which are released and can influence in various ligaments in the body. The hormonal action, especially relaxin, is what causes the increased relaxation in joints and ligaments, which makes the joints more flexible and unstable 4Birch K, Fowler NE, Rodacki AL, Rodacki CL. Stature loss and recovery in pregnant women with and without low back pain. Arch Phys Med Rehabil, 2003, 84(4):507-12.?. 2000 May; 82(5):625-32.,6Corrêa MC, Corrêa MD. Puerpério. In: Corrêa MD. Noções práticas de obstetrícia. 12. ed. Rio de Janeiro: Medsi; 1999. p. 95-104.. Stresses are imposed on the muscles of the abdominal wall tissue and structures as the uterus and the baby increase in size and weight and pregnancy progresses 7Boxer S, Jones S. Intra-rater reliability of rectus abdominis diastasis measurement using dial calipers. Austral J Physiother. 1997; 43(2):109 - 14.. The pregnant uterus growing will contribute to stretch these muscles as a result of the laxity of the linea alba and facilitating the separation of the abdominis rectus 8Thompson A, Skinner A, Piercy J. Fisioterapia de Tidy. 12. ed. São Paulo: Santos; 1994.. Thus, the main biomechanical factor to consider comes from the steady growth of the uterus, with forward position, leaning to the abdominal wall, besides the increase in weight and size of the breasts, that contribute to the displacement of the center of gravity of the body, hanging forward, as well as the spacing of the beams of the anterior abdominal wall muscles 9Rudge MVC, Borges VTM, Calderon IMP. Adaptações do Organismo Materno à Gravidez. In: Neme B. Obstetrícia Básica. 3. ed. São Paulo: Sarvier; 2005. p. 36-62.,10Barbosa AMP. Efeito da via de parto sobre a força muscular do assoalho pélvico. Rev Bras Ginecol Obstet. 2005 Nov: 27(11): 677-82..
As a result of such hormonal and biomechanical changes, it is highlighted the Diastasis of the Rectus Abdominis Muscle (DRAM). The DRAM is characterized by the separation of the abdominis rectus, as a result of enlargement of the linea alba and the increase in volume of the uterus 7Boxer S, Jones S. Intra-rater reliability of rectus abdominis diastasis measurement using dial calipers. Austral J Physiother. 1997; 43(2):109 - 14.,11Polden M, Mantle J. Fisioterapia em obstetrícia e ginecologia. 2. ed. São Paulo: Santos, 2000.. In this separation may occur a variation of a small vertical gap of up to 2 or 3 centimeters wide and 12 to 15 centimeters in length, up to a space measuring from 12 to 20 centimeters wide, and extends over almost the entire length of the rectus muscle, in which gravity varies from one woman to another 11Polden M, Mantle J. Fisioterapia em obstetrícia e ginecologia. 2. ed. São Paulo: Santos, 2000.,12Souza ELB. Fisioterapia aplicada à obstetrícia. Rio de Janeiro: Medsi; 2002.. It is painless and has lower incidence in women with good abdominal tone before pregnancy 13Baracho E. Fisioterapia aplicada à obstetrícia, uroginecologia e aspectos de mastologia. 4. ed. Rio de Janeiro: Guanabara Koogan; 2007..
The DRAM is more prevalent in obese, multiparous women, in cases of fetal macrosomia, flaccid abdominal muscles, multiple pregnancies and polyhydramnios 14Rett TM, Braga MD, Bernardes NO, Andrade SC. Prevalência de diástase dos músculos retoabdominais no puerpério imediato: comparação entre primíparas e multíparas. Rev Bras Fisioter. 2009; 13(4):275-80.. Women who have greater predisposition to suffer DRAM are those with multiple births, the multiparous and those with narrow pelvis, because during pregnancy, the baby will be located more anteriorly. The dysfunction may extend both above and below the navel, only occur below the navel or even include most of the linea alba 11Polden M, Mantle J. Fisioterapia em obstetrícia e ginecologia. 2. ed. São Paulo: Santos, 2000..
In most women, over the days after delivery, the separation tends to be smaller, but may not disappear without carrying out a treatment program 11Polden M, Mantle J. Fisioterapia em obstetrícia e ginecologia. 2. ed. São Paulo: Santos, 2000.. After delivery, usually the involution of the uterus remains in a 14-day period, but the abdominal muscles can take six weeks or more to get back on their pre-gravitational state and six months to return to full strength 8Thompson A, Skinner A, Piercy J. Fisioterapia de Tidy. 12. ed. São Paulo: Santos; 1994.. After delivery, puerperium starts, which corresponds to the period between birth and when the maternal organism returns to their pre-gravidic conditions 15Carvalho GM. Enfermagem em obstetrícia. São Paulo: EPU; 2004..
From the above, this study aimed to determine the prevalence of DRAM in immediate puerperium, in women attending the Unified Health System (SUS) in Guarapuava-PR, as well as investigate possible links between the presence of DRAM and be primiparous or multiparous; compare the average weight before pregnancy, during pregnancy and in the puerperium period and the presence of DRAM, and check the averages of separation of the rectus abdominis in supra-umbilical areas, umbilical and infra-umbilical.
Materials and methods
This study is characterized by a descriptive research, of the transversal type.
Considering the ethical aspects, the study was approved by the Ethics Committee in Research involving human beings of the Universidade Estadual do Centro-Oeste - COMEP/UNICENTRO, according to resolution no 119/2011. After clarification about the goals and procedures of the study, women who met the inclusion criteria listed below were invited to participate in it and, upon their accession, the Free and Informed Consent was read and signed in duplicate. One copy was given to the participant and the other was kept by the responsible researcher. Strict condition of confidentiality were assured their names as well as cost-free guarantee, according to Resolution 196/96 of the National Health Council.
The inclusion criteria were being female; aged 18 at least; reside in the city of Guarapuava, PR; and have realized the prenatal care at one of the 32 Basic Health Units (UBAS) or at Women's Clinic.
The invitation to attend the study was conducted in two UBAS, at the Women's Clinic and Maternity of Hospital de Caridade São Vicente de Paulo, being those care facilities attending via SUS in the city of Guarapuava, PR, from May 2011 to December 2012.
The study included a sample of 88 women.
Procedures and tools for assessment and data collection
The evaluation of the participants was at their home until the tenth day after delivery.
Data were collected through medical records and specific evaluation. These data were entered into an evaluation form, elaborated specifically for this research. In that data sheet information were recorded such as age; marital status; weight; level of education; obstetric history: number of pregnancies; about the current pregnancy: type of delivery; weight before pregnancy; the first and last visit of prenatal care; weight at the evaluation date and type of pregnancy. In that same data sheet was recorded the presence or absence of DRAM and its measurements in centimeters.
For anthropometric assessment after delivery it was used a mechanical scale of brand Britannia with a capacity of 120 kg. To measure the DRAM, when present, an analog caliper of brand Zaas Precision was used, with a sensitivity of 0.1 centimeters.
The DRAM measurement was performed according to Rett et al. 14Rett TM, Braga MD, Bernardes NO, Andrade SC. Prevalência de diástase dos músculos retoabdominais no puerpério imediato: comparação entre primíparas e multíparas. Rev Bras Fisioter. 2009; 13(4):275-80.,16Mesquita LA, Machado AV, Andrade AV. Fisioterapia para redução da diástase dos músculos retos abdominais no pós-parto. Rev Bras Ginecol Obstetr. 1999; 21(5): 267-272.,17Rett TM, Bernardes NO, Santos AM, Oliveira MR, Andrade SC. Atendimento de puérperas pela fisioterapia em uma maternidade pública humanizada. Fisiot Pesqui. 2008nov; 15(4): 361-6., with the puerperal woman in the supine position, in which she maintained hips and knees flexed at 90°, being the feet supported and upper limbs extended along the body. In this position the puerperal woman was requested to flex the trunk until the inferior angle of the scapula got out of bed. The umbilicus was the reference point during forward flexion motion of the trunk, in which the reference was 4.5 cm above and below the umbilicus, in which supra-umbilical, umbilical and infra-umbilical measures were named, and fingers were placed perpendicularly between the medial edges of the rectus abdominis muscles. At the same time that occurred palpation the analog caliper was used for measuring in cases which occurred DRAM. DRAM was considered present when there was any distance between the medial edges of the rectus abdominis muscle.
Data analysis
Statistical analysis included percentage rate calculation for the DRAM prevalence rate. The descriptive analysis included measures of central tendency (average), dispersion (standard deviation), frequency and percentage. Additionally, we used the Student t test to verify the probability distribution of numerical variables and independent variables.
The Pearson correlation was used to verify the existence and magnitude of the correlation, if present, between being primiparous or multiparous and having DRAM. Data were analyzed using SPSS 11.0 software, and was considered a significance level of p < 0,05.
Results

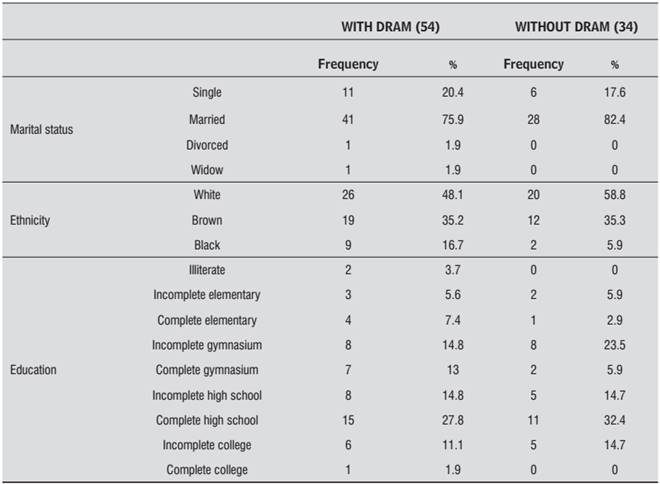
Table 1 shows the socio demographic data of the participants.
Socio Demographic data of the participants, according to the presence or absence of DRAM, 2012
Table 2shows data relating to the participants' reproductive history.
Data concerning the participants' reproductive histories, according to the presence or absence of DRAM, 2012
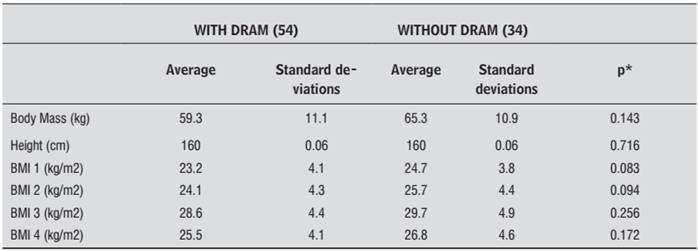
Table 3shows a comparison of the mean values and their respective standard deviations of body composition before pregnancy 1Costa ES, Pinon GMB, Costa TS, Santos RCA, Nóbrega AR, Souza LB. Alterações fisiológicas na percepção de mulheres durante a gestação. Rev Rene. 2010; 11(2):86-93 ., at the first prenatal visit 2Mann L, Kleinpaul JF, Teixeira CS, Konopka CK. Dor Lombo Pélvica e exercício físico durante a gestação. FisioterMov. 2008; 21(2):99-105., at the last prenatal visit 3Marnach ML, Ramin KD, Ramsey PS, Song SW, Stensland JJ, An KN. Characterization of the relationship between joint laxity and maternal hormones in pregnancy. Obstet Gynecol. 2003; 101(2):331-5. and assessing during the puerperal period 4Birch K, Fowler NE, Rodacki AL, Rodacki CL. Stature loss and recovery in pregnant women with and without low back pain. Arch Phys Med Rehabil, 2003, 84(4):507-12.?. 2000 May; 82(5):625-32., among women who presented DRAM and those who did not present it.
Comparison of the average body weight before, during and after pregnancy, according to group, Guarapuava, PR, 2012. Student's t test, significance level p < 0.05
These results show average weight gain similar between the two groups, as well as a loss of weight postpartum at the same levels, but these data have not showed to be statistically significant, as regards the presence of DRAM.
Table 4 shows the average values and their respective standard deviations concerning the DRAM in the measured regions supra-umbilical, umbilical and infra-umbilical.
Average values and standard deviation for DRAM supra-umbilical, umbilical and infra-umbilical, Guarapuava/PR, 2012
Discussion
The literature suggests that the advancement of pregnancy influences the integrity of the linea alba, so DRAM is more common in the third trimester and immediate puerperium 18Lemos, A, Caminha MA, Melo Jr EF, Dornelas de Andrade A. Avaliação da Força Muscular Respiratória no Terceiro Trimestre de Gestação. Rev Bras Fisioter. 2005; 9(2):151-156.. However, values that refer to the DRAM are variable 7Boxer S, Jones S. Intra-rater reliability of rectus abdominis diastasis measurement using dial calipers. Austral J Physiother. 1997; 43(2):109 - 14.,16Mesquita LA, Machado AV, Andrade AV. Fisioterapia para redução da diástase dos músculos retos abdominais no pós-parto. Rev Bras Ginecol Obstetr. 1999; 21(5): 267-272.,19Spitznagle TM, Leong FC, Van Dillen LR. Prevalence of diastasis recti abdominis in a urogynecological patient population. Int Urogynecol J Pelvic Floor Dysfunct. 2007; 18(3):321-8., for there is a disagreement as to the measures of DRAM to be considered as a clinically relevant problem, there is no scientific evidence to determine the exact numerical value for the diastasis to be considered pathological. The prevalence of DRAM rate in immediate puerperium reported in this study (61.36%) is in agreement with the literature, which shows the prevalence rate of DRAM from 32% to 68% 17Rett TM, Bernardes NO, Santos AM, Oliveira MR, Andrade SC. Atendimento de puérperas pela fisioterapia em uma maternidade pública humanizada. Fisiot Pesqui. 2008nov; 15(4): 361-6.,20Boissonnault JS, Blaschak MJ. Incidence of diastasis recti abdominis during the childbearing year. Phys Ther. 1988July; 68(7):1082-6.. Rett et al. 14Rett TM, Braga MD, Bernardes NO, Andrade SC. Prevalência de diástase dos músculos retoabdominais no puerpério imediato: comparação entre primíparas e multíparas. Rev Bras Fisioter. 2009; 13(4):275-80. found prevalence rates of DRAM supra-umbilical of 68% and infra- umbilical of 32%. The supra-umbilical prevalence among primiparous and multiparous was identical (68%) and infra-umbilical higher in multiparous (19.8% e 29.2%). Boissonnault and Blaschak 20Boissonnault JS, Blaschak MJ. Incidence of diastasis recti abdominis during the childbearing year. Phys Ther. 1988July; 68(7):1082-6., in their study with primiparous, found the presence of DRAM in 66% of the group studied in the third trimester of pregnancy, 53% of the immediate postpartum group, and 36% in the postpartum group which were between five and seven weeks after giving birth. There is a difference in studies 14Rett TM, Braga MD, Bernardes NO, Andrade SC. Prevalência de diástase dos músculos retoabdominais no puerpério imediato: comparação entre primíparas e multíparas. Rev Bras Fisioter. 2009; 13(4):275-80.,20Boissonnault JS, Blaschak MJ. Incidence of diastasis recti abdominis during the childbearing year. Phys Ther. 1988July; 68(7):1082-6., Rett et al. 14Rett TM, Braga MD, Bernardes NO, Andrade SC. Prevalência de diástase dos músculos retoabdominais no puerpério imediato: comparação entre primíparas e multíparas. Rev Bras Fisioter. 2009; 13(4):275-80. investigated both primiparous and multiparous, while Boissonnault e Blaschak 20Boissonnault JS, Blaschak MJ. Incidence of diastasis recti abdominis during the childbearing year. Phys Ther. 1988July; 68(7):1082-6. evaluated only primiparous.
In previous studies 14Rett TM, Braga MD, Bernardes NO, Andrade SC. Prevalência de diástase dos músculos retoabdominais no puerpério imediato: comparação entre primíparas e multíparas. Rev Bras Fisioter. 2009; 13(4):275-80.,16Mesquita LA, Machado AV, Andrade AV. Fisioterapia para redução da diástase dos músculos retos abdominais no pós-parto. Rev Bras Ginecol Obstetr. 1999; 21(5): 267-272.,17Rett TM, Bernardes NO, Santos AM, Oliveira MR, Andrade SC. Atendimento de puérperas pela fisioterapia em uma maternidade pública humanizada. Fisiot Pesqui. 2008nov; 15(4): 361-6.,20Boissonnault JS, Blaschak MJ. Incidence of diastasis recti abdominis during the childbearing year. Phys Ther. 1988July; 68(7):1082-6., the criteria used to measure the DRAM were subjective. Physiotherapists need a reliable tool to give reliability to the measurement of such measures in their clinical practice 7Boxer S, Jones S. Intra-rater reliability of rectus abdominis diastasis measurement using dial calipers. Austral J Physiother. 1997; 43(2):109 - 14.) and verify the reduction in DRAM objectively. In this study, an analog caliper was originally employed for this purpose.
The physical therapy assessment and treatment of DRAM are critical to the health and biomechanics of the woman's body 19Spitznagle TM, Leong FC, Van Dillen LR. Prevalence of diastasis recti abdominis in a urogynecological patient population. Int Urogynecol J Pelvic Floor Dysfunct. 2007; 18(3):321-8.. It can be considered damaging a DRAM above 2.5 cm 19Spitznagle TM, Leong FC, Van Dillen LR. Prevalence of diastasis recti abdominis in a urogynecological patient population. Int Urogynecol J Pelvic Floor Dysfunct. 2007; 18(3):321-8., from that value, the abdominal muscles may not be performing efficiently the stabilization of the trunk, and functions as posture, defecation, parturition, trunk movements 22Sapsford R. Rehabilitation of pelvic floor muscles utilizing trunk stabilization. Man Ther. 2004; 9(1):3-12. and lumbar stabilization 11Polden M, Mantle J. Fisioterapia em obstetrícia e ginecologia. 2. ed. São Paulo: Santos, 2000.. The physical therapy will be favoring the improvement of abdominal muscle tone and trophism, the reduction of diastasis in a shorter period than physiological 23Borges FS, Valentin CE. Tratamento da flacidez e diástase do reto abdominal no puerpério de parto normal com uso de eletroestimulação muscular com corrente de média frequência - Estudo de caso. Rev Bras Fisioter Derm-Func. 2002; 1(1)..
It was found that, regardless of parity, the prevalence and average of DRAM in the overall sample is below in the infra-umbilical region, compared to the supra-umbilical region. The mean values found in this study were 0.88 cm for supra-umbilical, 1.23 cm umbilical and 0.3 cm for infra-umbilical. Rett et al. 14Rett TM, Braga MD, Bernardes NO, Andrade SC. Prevalência de diástase dos músculos retoabdominais no puerpério imediato: comparação entre primíparas e multíparas. Rev Bras Fisioter. 2009; 13(4):275-80. found a higher supra-umbilical separation, equivalent to 2.8 cm, and infra-umbilical 1.5 cm. Boissonnault e Blaschak 20Boissonnault JS, Blaschak MJ. Incidence of diastasis recti abdominis during the childbearing year. Phys Ther. 1988July; 68(7):1082-6. concluded that most of the diastases were seen in the navel area (52%), although a large number of women also showed it above the navel (36%). Only 11% of diastases were found below the navel. In Aragão's research 24Aragão ASL, Jesus CS, Spinola FD. Prevalência da diástase dos músculos retos abdominais em gestantes em um hospital geral público do interior da Bahia. Rev Dig Buenos Aires. 2009; 13(129)., there was an average of 14.60 mm for supra-umbilical measure, 22.88 mm umbilical and 12.70 mm for infra-umbilical. In the study of Leite and Araujo 25Leite ACNMT, Araújo KKBC. Diástase dos retos abdominais em puérperas e sua relação com variáveis obstétricas. FisioterMov. 2012; 25(2):389-397. there was a higher incidence in the supra-umbilical region associated with the umbilical separation (50%) and umbilical associated with infra-umbilical and supra-umbilical (23%). In the study of Luna et al. 26Luna DCB, Cavalcanti ALAMH, Guendler JA, Brito VC, Oliveira BDR. Frequência da Diástase Abdominal em Puérperas e Fatores de Risco Associados. Rev Fisioter S Fun. Fortaleza, 2012; 1(2):10-17. numerically greater diastasis were presented in umbilical and infra umbilical levels. The supra-umbilical DRAM is the most significant and most frequent during pregnancy, due to stretching of the abdominal muscles, which is necessary to allow uterine growth, therefore, occurring the separation of the beams of the abdominis rectus muscles 23Borges FS, Valentin CE. Tratamento da flacidez e diástase do reto abdominal no puerpério de parto normal com uso de eletroestimulação muscular com corrente de média frequência - Estudo de caso. Rev Bras Fisioter Derm-Func. 2002; 1(1)..
The fact that the DRAM have lower prevalence in the infra-umbilical region, can be explained by anatomical differences existing between the dispositions of the fascia overlying the rectus abdominis. The sheath of the rectus abdominis muscle is formed, anteriorly, by the aponeurosis of the external oblique muscle and the anterior layer of the aponeurosis of the internal oblique muscle and, posteriorly, by the posterior layer of the aponeurosis of the internal oblique muscle and the aponeurosis of the transverse abdominal muscle. In the infra-umbilical region, the anatomical arrangement is modified. All elements of the posterior sheath begin to position themselves anterior to the rectus abdominis muscle, merging with the elements of the anterior sheath. In the posterior sheath of this muscle this transition can be clearly seen, a line of firmer consistency than the caudal segment, structure called semicircular line. Thus, in the final portion of these muscles, the aponeurotic arrangement is different, avoiding dispelling 27Fonseca T, Franco D, Arbex GL, Franco T. Estudo anatômico da linha semicircular e sua importância cirúrgica na reconstrução da mama. Rev Bras Cir Plást. 2010; 25(2):325-9.,28Silva CB, Lemos A, Oliveira BDR. A diástase do músculo reto abdominal interfere na prensa abdominal no período expulsivo do parto? {Internet} Rio de Janeiro; 2009. {cited 2013 apr 20}. Available from: Available from: http://interfisio.com.br/especialidade/?gineco_obstetricia/artigo&ID=374
http://interfisio.com.br/especialidade/?...
. Authors 16Mesquita LA, Machado AV, Andrade AV. Fisioterapia para redução da diástase dos músculos retos abdominais no pós-parto. Rev Bras Ginecol Obstetr. 1999; 21(5): 267-272.,19Spitznagle TM, Leong FC, Van Dillen LR. Prevalence of diastasis recti abdominis in a urogynecological patient population. Int Urogynecol J Pelvic Floor Dysfunct. 2007; 18(3):321-8. indicate that the DRAM is most prevalent in multiparous and multigestas 25Leite ACNMT, Araújo KKBC. Diástase dos retos abdominais em puérperas e sua relação com variáveis obstétricas. FisioterMov. 2012; 25(2):389-397., so the present study is in accordance with that literature. This can be explained by the parity itself and multiple pregnancies, which can facilitate the mechanical stress in the connective tissue of the abdominal wall 14Rett TM, Braga MD, Bernardes NO, Andrade SC. Prevalência de diástase dos músculos retoabdominais no puerpério imediato: comparação entre primíparas e multíparas. Rev Bras Fisioter. 2009; 13(4):275-80.. Consecutive pregnancies that do not respect the gestational period, or have diastasis, but are untreated, have a higher possibility of increasing the DRAM 24Aragão ASL, Jesus CS, Spinola FD. Prevalência da diástase dos músculos retos abdominais em gestantes em um hospital geral público do interior da Bahia. Rev Dig Buenos Aires. 2009; 13(129)..
When comparing the average body weight or BMI before, during and after pregnancy, these apparently did not demonstrate a direct correlation with respect to the presence of DRAM, because the medium remained similar in both groups, with and without DRAM. The group that showed DRAM averaged body mass of 59.3 kg and average BMI of 23.2 kg/m² before pregnancy, 24.1 kg/m² in the first consultation, 28.6 kg/m² in the last consultation and 25.5 kg/m² to 10 days after delivery, and the group that did not present DRAM, had as average body mass 65.3 kg and average BMI of 24.7 kg/m² before pregnancy, 25.7 kg/m² in the first consultation, 29.7 kg/m² in the last consultation and 26.8 kg/m² to 10 days after delivery.
This study has some limitations, such as the sample size, which can be considered small for the city as a whole, considering the number of inhabitants.
Conclusion
The results of the presented study showed a considerable prevalence of DRAM, where this average was higher in the umbilical region compared to infra and supra-umbilical. Multiparous women had higher correlation with DRAM than primiparous.
It is suggested to continue research on the topic, so that, in possession of a larger sample, more conclusive data might be obtained regarding the prevalence of DRAM in postpartum women in Guarapuava, PR.
In face of this study results, which showed a lot of women with DRAM in immediate puerperium, it is concluded that further clarification and dissemination of the work done by the physiotherapist with the obstetric and gynecological patients is necessary, as they are necessary and can be very beneficial.
References
- Costa ES, Pinon GMB, Costa TS, Santos RCA, Nóbrega AR, Souza LB. Alterações fisiológicas na percepção de mulheres durante a gestação. Rev Rene. 2010; 11(2):86-93 .
- Mann L, Kleinpaul JF, Teixeira CS, Konopka CK. Dor Lombo Pélvica e exercício físico durante a gestação. FisioterMov. 2008; 21(2):99-105.
- Marnach ML, Ramin KD, Ramsey PS, Song SW, Stensland JJ, An KN. Characterization of the relationship between joint laxity and maternal hormones in pregnancy. Obstet Gynecol. 2003; 101(2):331-5.
- Birch K, Fowler NE, Rodacki AL, Rodacki CL. Stature loss and recovery in pregnant women with and without low back pain. Arch Phys Med Rehabil, 2003, 84(4):507-12.?. 2000 May; 82(5):625-32.
- Mann L, Kleinpaul JF, Mota CB, Santos SG. Alterações biomecânicas durante o período gestacional: uma revisão. Motriz: Rev Ed Fís. 2010; 16(3):730 - 41.
- Corrêa MC, Corrêa MD. Puerpério. In: Corrêa MD. Noções práticas de obstetrícia. 12. ed. Rio de Janeiro: Medsi; 1999. p. 95-104.
- Boxer S, Jones S. Intra-rater reliability of rectus abdominis diastasis measurement using dial calipers. Austral J Physiother. 1997; 43(2):109 - 14.
- Thompson A, Skinner A, Piercy J. Fisioterapia de Tidy. 12. ed. São Paulo: Santos; 1994.
- Rudge MVC, Borges VTM, Calderon IMP. Adaptações do Organismo Materno à Gravidez. In: Neme B. Obstetrícia Básica. 3. ed. São Paulo: Sarvier; 2005. p. 36-62.
- Barbosa AMP. Efeito da via de parto sobre a força muscular do assoalho pélvico. Rev Bras Ginecol Obstet. 2005 Nov: 27(11): 677-82.
- Polden M, Mantle J. Fisioterapia em obstetrícia e ginecologia. 2. ed. São Paulo: Santos, 2000.
- Souza ELB. Fisioterapia aplicada à obstetrícia. Rio de Janeiro: Medsi; 2002.
- Baracho E. Fisioterapia aplicada à obstetrícia, uroginecologia e aspectos de mastologia. 4. ed. Rio de Janeiro: Guanabara Koogan; 2007.
- Rett TM, Braga MD, Bernardes NO, Andrade SC. Prevalência de diástase dos músculos retoabdominais no puerpério imediato: comparação entre primíparas e multíparas. Rev Bras Fisioter. 2009; 13(4):275-80.
- Carvalho GM. Enfermagem em obstetrícia. São Paulo: EPU; 2004.
- Mesquita LA, Machado AV, Andrade AV. Fisioterapia para redução da diástase dos músculos retos abdominais no pós-parto. Rev Bras Ginecol Obstetr. 1999; 21(5): 267-272.
- Rett TM, Bernardes NO, Santos AM, Oliveira MR, Andrade SC. Atendimento de puérperas pela fisioterapia em uma maternidade pública humanizada. Fisiot Pesqui. 2008nov; 15(4): 361-6.
- Lemos, A, Caminha MA, Melo Jr EF, Dornelas de Andrade A. Avaliação da Força Muscular Respiratória no Terceiro Trimestre de Gestação. Rev Bras Fisioter. 2005; 9(2):151-156.
- Spitznagle TM, Leong FC, Van Dillen LR. Prevalence of diastasis recti abdominis in a urogynecological patient population. Int Urogynecol J Pelvic Floor Dysfunct. 2007; 18(3):321-8.
- Boissonnault JS, Blaschak MJ. Incidence of diastasis recti abdominis during the childbearing year. Phys Ther. 1988July; 68(7):1082-6.
- Foti T, Davids JR, Bagley A. A biomechanical analysis of gait during pregnancy. 2000May; 82(5):625-32.
- Sapsford R. Rehabilitation of pelvic floor muscles utilizing trunk stabilization. Man Ther. 2004; 9(1):3-12.
- Borges FS, Valentin CE. Tratamento da flacidez e diástase do reto abdominal no puerpério de parto normal com uso de eletroestimulação muscular com corrente de média frequência - Estudo de caso. Rev Bras Fisioter Derm-Func. 2002; 1(1).
- Aragão ASL, Jesus CS, Spinola FD. Prevalência da diástase dos músculos retos abdominais em gestantes em um hospital geral público do interior da Bahia. Rev Dig Buenos Aires. 2009; 13(129).
- Leite ACNMT, Araújo KKBC. Diástase dos retos abdominais em puérperas e sua relação com variáveis obstétricas. FisioterMov. 2012; 25(2):389-397.
- Luna DCB, Cavalcanti ALAMH, Guendler JA, Brito VC, Oliveira BDR. Frequência da Diástase Abdominal em Puérperas e Fatores de Risco Associados. Rev Fisioter S Fun. Fortaleza, 2012; 1(2):10-17.
- Fonseca T, Franco D, Arbex GL, Franco T. Estudo anatômico da linha semicircular e sua importância cirúrgica na reconstrução da mama. Rev Bras Cir Plást. 2010; 25(2):325-9.
- Silva CB, Lemos A, Oliveira BDR. A diástase do músculo reto abdominal interfere na prensa abdominal no período expulsivo do parto? {Internet} Rio de Janeiro; 2009. {cited 2013 apr 20}. Available from: Available from: http://interfisio.com.br/especialidade/?gineco_obstetricia/artigo&ID=374
» http://interfisio.com.br/especialidade/?gineco_obstetricia/artigo&ID=374
Publication Dates
-
Publication in this collection
Apr-Jun 2016
History
-
Received
20 June 2013 -
Accepted
18 Aug 2015