Abstract
Since fluoridation of water is an established public health measure for the prevention of dental caries and considering that monitoring of the method is crucial to its success, this study aimed to analyze the results of the analysis of the fluorine content of public water supply of 40 municipalities in the state of São Paulo, from November 2004 to December 2016. Samples were analyzed monthly using the potentiometric method. Of the 32,488 samples, 50.94% contained fluoride levels within the recommended range. In 2004, it was verified that 21 cities (52.50%) had mean levels within the recommended parameter, increasing to 32 cities (80.00%) in 2016. It was observed that 15 municipalities that initially had levels of fluoride below 0.55 mgF/L in their water supply adjusted to adequate levels during the project. In the first year of the study, 47.76% of the samples had values in the recommended range, which increased to 58.22% in 2016. Most of the municipalities adjusted the levels of fluoride in their waters over the years, evidencing the performance of heterocontrol programs as important strategies that assist in the monitoring of the method and have significant participation in the control of the water quality supplied to the population.
Key words
Fluoridation; Public health; Oral health; Water supply
Resumo
Sendo a fluoretação das águas uma medida de saúde pública consagrada na prevenção de cárie dentária e considerando que a vigilância do método é fundamental para o seu sucesso, este estudo objetivou analisar os resultados das análises dos teores de flúor das águas de abastecimento público de 40 municípios do estado de São Paulo, de novembro de 2004 a dezembro de 2016. A análise das amostras foi realizada mensalmente por meio do método potenciométrico. De 32.488 amostras, 50,94% continham níveis de flúor dentro do intervalo recomendado. Em 2004, verificou-se que 21 cidades (52,50%) apresentaram teores médios dentro do parâmetro recomendado, passando, em 2016, para 32 cidades (80,00%). Observou-se que 15 municípios que possuíam inicialmente níveis de flúor abaixo de 0,55 mgF/L em suas águas de abastecimento adequaram-se no decorrer do projeto. No primeiro ano do estudo, 47,76% das amostras possuíam valores no intervalo preconizado e, em 2016, houve um aumento para 58,22%. Foi verificado que no decorrer dos anos, a maioria dos municípios adequou os níveis de flúor em suas águas, evidenciando a atuação dos programas de heterocontrole como importantes estratégias que auxiliam na vigilância do método, tendo participação fundamental no controle da qualidade da água ofertada à população.
Palavras-chave
Fluoretação; Saúde pública; Saúde bucal; Abastecimento de água
Introduction
Public water supply fluoridation is a safe, efficient, low-cost, widely available scientific method of prevention of dental caries and is the most important collective fluoride application in Public Health, and continuity and regularity of the recommended levels should be respected11 Moimaz SAS, Saliba NA, Saliba O, Sumida DH, Souza NP, Chiba FY, Garbin CAS. Water fluoridation in 40 Brazilian cities: 7 year analysis. J Appl Oral Sci 2013; 21(1):13-19.,22 Viegas AR. Fluoretação da água de abastecimento público. Rev Bras Med 1989; 46(6): 209-216.. The method is recommended by the World Health Organization (WHO), Pan American Health Organization33 Murray JJ. Uso correto de fluoretos na saúde pública. São Paulo: Ed. Santos; 1992., and other national and international health organizations. The United States Centers for Disease Control and Prevention (CDC) considers it one of the top ten achievements of public health in the twentieth century, matching it to the level of importance of vaccinations44 Centers for Disease Control and Prevention. Achievements in Public Health, 1900-1999: fluoridation of drinking water to prevent dental caries. MMWR 1999; 48(41):933-940..
In 1945, for the first time, the addition of fluoride in the public supply waters was carried out aiming at the prevention of dental caries. Pilot studies were conducted in the cities of Grand Rapids and Newburgh, in the United States; and in Brantford, Canada, evaluating and comparing the results found with those of the control cities of Muskegon and Kingston in the United States; and Sarnia, Canada. The investigations were carefully monitored for medical and sanitary aspects. Besides the reduction of dental caries, the coefficients of some diseases, among them cancer, cardiovascular/renal/hepatic diseases and diabetes, were evaluated in all cities, which ascertained, as early as the 1950s, the efficacy, safety, low cost and comprehensiveness of the method55 Arnold Junior FA, Dean HT, Knutson JW. Effect of fluoridated public water supplies on dental caries prevalence. Public Health Rep 1956; 71(7):652-658.
6 Ast DB, Szwejda LF, Wilcox R. Newburgh-Kingston caries fluorine study. XV. Further observations of dental caries experience among children in Newburgh and Kingston, ages7-16 based on DMF frequency per child. New York J Dent 1958; 28:173-175.-77 Brown HK, McLaren HR, Stewart B. Brantford fluoridation caries study: 1954 report. J Canad Dent Assoc 1954; 20:585-602..
After the discovery of these findings, studies were conducted to improve the implementation of the method. Thus, in 1957, a study showed that the variability in the volume of water consumed by the population due to the climatic conditions of each region can significantly change the amount of fluoride ingested from this source. Thus, the recommended levels of fluoride in the public water supply were established by the maximum temperature means of each location88 Galagan DJ, Vermillion JR. Determining optimum fluoride concentrations. Public Health Rep 1957; 72(6):491-493..
In Brazil, the first city to add fluoride to the public water supply was Baixo Guandu, Espírito Santo, in 1953, under the responsibility of the Foundation of Special Services in Public Health (FSESP) of the Ministry of Health99 Pinto VG. Prevenção da cárie dental. In: Pinto VG. Saúde bucal: odontologia social e preventiva. 3ª ed. São Paulo: Santos; 1992. p. 275-328.. An epidemiological study conducted in this municipality showed that the DMFT index of its inhabitants was much lower in comparison to the rest of the country, evidencing the efficacy of the method in the long term1010 Saliba NA, Moimaz SAS, Casotti CA, Pagliari AV. Dental caries of lifetime residents in Baixo Guandu, Brazil, fluoridated since 1953. J Public Health Dent 2008; 68(2):119-121..
The second municipality to add fluoride to its waters was Marília, in the state of São Paulo, in December 19561111 Buendia OC. Fluoretação de águas de abastecimento público no Brasil: atualização. Rev Assoc Paul Cir Dent 1984; 38(2):138-158.. A year later, Taquara, in Rio Grande do Sul, also adopted the method, which was the first state in the country to draft a law that made fluoridation mandatory in 19571212 Pires Filho FM, Bernd B, Ely HC, Pegoraro MT. Flúor: manual informativo. Porto Alegre: SSMA-RS/UFRGS; 1989.. In 1958, Curitiba is the fourth city in Brazil and also the first capital to fluoride its waters1313 Muniz A. Prevalência da cárie dentária em escolares de Curitiba, antes e após exposição contínua à água fluoretada: 1958-1968. Curitiba: SSP-PR; 1969.. Although it was started in the 1950s in Brazil, the method becomes mandatory throughout the national territory in 1974, through the approval of Federal Law Nº 6.050, in public supply systems of locations with water treatment plants1414 Brasil. Lei nº 6.050, de 24 de maio de 1974. Dispõe sobre a obrigatoriedade da fluoretação das águas em sistema de abastecimento. Diário Oficial da União 1974; 27 maio..
In the state of São Paulo, after the approval of Federal Law Nº 6.050, the first epidemiological studies of dental caries began, and Barretos was one of the municipalities whose population was analyzed: it was found that, after 10 years of fluoridation of its waters, in the age group of 7-10 years, 50% of the children had no permanent teeth attacked by caries, and in children aged 3-5 years, 51.6% did not have any primary teeth affected by the disease1515 Viegas Y, Viegas AR. Análise dos dados de prevalência de cárie dental na cidade de Barretos, SP, Brasil, depois de dez anos de fluoretação da água de abastecimento público. Rev Saude Publica 1985; 19(4):287-299.. In the city of Campinas, which was also the subject of research, was aimed at evaluating the prevalence of dental caries after fourteen years of fluoridation of its waters, and it was evidenced that the declining caries prevalence found was similar to the investigations found in Brazil and other countries at the time1616 Viegas Y, Viegas AR. Prevalência de cárie dental na cidade de Campinas, SP, Brasil, depois de quatorze anos de fluoração da água de abastecimento pública. Rev Assoc Paul Cir Dent 1985; 39(5):272-282.. Since the 1980s, more studies that evidenced caries prevalence and water fluoridation were conducted in several cities in the northwest region of the state of São Paulo, such as Birigui1717 Saliba NA, Arcieri RM, Moimaz SAS, Sundefeld MLMM. Redução na prevalência da cárie dentária, após dez anos de fluoretação da água de abastecimento público, no município de Birigui, SP. Brasil. Rev Fac Odontol Lins 1995; 8:41-45., Penápolis1818 Saliba NA, Saliba O, Ayres JPS, Rey CR. Prevalência de cárie dentária em escolares da cidade de Penápolis-SP. Rev Gaúcha Odontol 1980; 28:287-289. and Araçatuba1919 Saliba NA, Saliba O, Rey CR, Vieira SMM, Ayres JPS. Prevalência da cárie dentária, após 5 anos de fluoretação das águas do sistema público de abastecimento, em escolares de Araçatuba, Estado de São Paulo. Odontól Mod 1981; 8:6-8..
The importance of expanding the implementation of the method was discussed in the National Oral Health Conferences of 1986, 1993 and 20042020 Narvai PC, Frazão P, Fernandez RAC. Fluoretação da água e democracia. Saneas 2004; 2:29-33.. Water fluoridation is one of the National Oral Health Policy Guidelines established in 2004:
It is understood that access to treated and fluoridated water is fundamental to the health conditions of the population. Thus, making public policies that ensure the implementation of water fluoridation, expanding the program to municipalities with treatment systems is the most comprehensive and socially fair way of access to fluorine. Thus, developing intersectoral actions to expand water fluoridation in Brazil is a governmental priority, ensuring continuity and adequate levels under the Law Nº 6.050 and complementary standards, with the establishment or development of compatible surveillance systems. The organization of such systems is the responsibility of the management bodies of SUS2121 Brasil. Ministério da Saúde (MS). Diretrizes da Política Nacional de Saúde Bucal. [acessado 2015 Abr 6]. Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/politica_nacional_brasil_sorridente.pdf
http://bvsms.saude.gov.br/bvs/publicacoe...
.
Public water supply fluorine content monitoring projects are developed in Brazil and aim to ensure the safety and continuity of the method, helping to maintain the recommended ion content and providing the population with access to quality water. Monitoring by a public or private institution other than that responsible for the addition of fluoride was called heterocontrol2222 Narvai PC. Cárie dentária e flúor: uma relação do século XX. Cien Saude Colet 2000; 5(2):381-392..
In 1991, the Araçatuba Dental School (UNESP) started a heterocontrol project with the São Paulo Association of Dental Surgeons, which aimed to implement the “Oral Disease Prevention Program”. Infrequently, analyses of water samples collected in municipalities in the northwest of the state of São Paulo were performed. The agreement expired, but the university continued it and, in 2004, the project was reformulated and analyzed monthly and systematically water samples from all 40 municipalities of the II Regional Department of Health (Araçatuba region) of the State Health Secretariat (SP).
The method requires constant monitoring to promote maximum efficacy in dental caries prevention, thus ensuring the population’s access to quality water and recommended fluorine levels that provide maximum benefit in disease prevention and minimal risk in the development of dental fluorosis.
Objective
This study aimed to analyze the public water supply fluorine content from 40 municipalities in the state of São Paulo from November 2004 to December 2016.
Methods
This is a longitudinal study, in which the results of the analyses of the project “Surveillance of the fluoride content of the public water supply in the municipalities of the northwest region of the state of São Paulo”, developed by the Public Health Research Group (NEPESCO) of the Faculty of Dentistry of Araçatuba (UNESP), which promotes the heterocontrol of fluorine levels in 40 cities in the northwest of São Paulo.
The municipalities included in the research belong to the area covered by the II Regional Health Department of the State of São Paulo, administrative division of the SES-SP: Alto Alegre, Andradina, Araçatuba, Auriflama, Avanhandava, Barbosa, Bento de Abreu, Birigui, Bilac, Braúna, Brejo Alegre, Buritama, Castilho, Clementina, Coroados, Gabriel Monteiro, Glicério, Guaraçai, Guararapes, Guzolândia, Ilha Solteira, Itapura, Lavínia, Lourdes, Luiziânia, Mirandópolis, Murutinga do Sul, Nova Castilho, Nova Independência, Nova Luzitânia, Penápolis, Pereira Barreto, Piacatú, Rubiácea, Santo Antônio do Aracanguá, Santópolis do Aguapeí, Sud Mennucci, Suzanápolis, Turiúba and Valparaíso.
Establishing collection points
The collection points of the samples were established after analyzing the maps of the water distribution networks of each municipality, as per the quantity and location of their water abstraction sources. Three collection points were defined in the area supplied by its source for each source of water supply of the locations. The addresses of the points were selected by convenience, preferably in public places (health posts, schools, nursing homes, squares, PHC facilities, among others) due to the greater ease of access. Formal contacts were established with the Secretaries of Health, Oral Health Coordinators and those responsible for water supply in each municipality.
Collection of water samples
Water samples were always collected in the first week of each month, directly from the supply network. In total, 40 ml polyethylene bottles, previously washed with deionized water to prevent contamination, were used to store collected water. They were hermetically sealed and identified by a label, with data referring to the sampling procedure: location, day, month, time at which it was performed and the name of the individual responsible for the collection. The samples were transported to the laboratory of the Public Health Research Center (NEPESCO) of the Faculty of Dentistry of Araçatuba (FOA-UNESP) for analysis within 150 days.
Laboratory analyses
The laboratory analyses were performed by an ion analyzer (Model 940EA; Orion Research, Inc., Beverly, MA, USA) coupled to a fluoride ion-reading combination electrode (Model 9609BN; Orion Research, Inc.), as per the method described by Cury et al.2323 Cury JA, Lima YBO, Vieira Filho W. Análise de flúor com eletrodo específico. Campinas: Unicamp; 2001..
The margin of error was reduced by calibration of the equipment in triplicate by constructing a calibration curve, taking into account the expected values for the samples with standards ranging from 0.1 to 1.6 milligrams of fluoride per liter (mgF/L). Dilutions were used from a standard fluoride solution at 100 mg/L (Orion, 940907). One ml of each of the five standards was collected, and 1 ml of “Total Ionic Strength Adjustment Buffer” (TISAB II) was added, a pH adjustment buffer, ionic strength and decomplexing agent, widely used in fluorine ion analyzes. Once the calibration curve was reached and the equipment was ready to perform the analyses, the samples were read in duplicate and the TISAB II compound was added at a 1:1 ratio. The values obtained in the ion analyzer were in millivolts (mV) and were converted into milligrams of fluoride per liter (mgF/L) when transferred to a Microsoft Office Excel spreadsheet.
Sending the results to the municipalities
The results of the water sample analyses were sent monthly to the water treatment managers, Health Secretaries and Oral Health Coordinators of each location.
Classifying fluorine contents
The classification of the samples’ fluorine content adopted the recommendation drafted by the Collaborating Center of the Ministry of Health in Oral Health Surveillance (CECOL), which is based on the principle of more significant benefit to caries prevention and lower risk of developing dental fluorosis, also considering the mean of the maximum annual temperatures of each location. For the studied region, the recommended bracket ranges from 0.55 to 0.84 mgF/L2424 Universidade de São Paulo. Consenso técnico sobre classificação de águas de abastecimento público segundo o teor de flúor. São Paulo: Universidade de São Paulo; 2011. (Chart 1).
Fluoride concentrations and benefit and risk levels for locations whose maximum temperature averages are between 26.3ºC and 32.5ºC, according to CECOL.
Results
In the period from November 2004 to December 2016, 32,488 samples of public water supply were collected and analyzed, in duplicate. In the percentage distribution of the samples (Table 1), it was observed that 50.94% of them were within the range that provides the maximum benefit in the prevention of caries and minimal risk in the development of dental fluorosis; 20.12% were included in the maximum benefit interval and moderate risk. Only a small proportion (4.48%) of the samples had fluorine contents higher than 1.14 mgF/L. Approximately a quarter of the samples had fluorine levels below the minimum level in order to achieve maximum preventive benefit.
Absolute and percentage distribution of water samples from 40 municipalities in the northwest of São Paulo, from November 2004 to December 2016, by fluorine content.
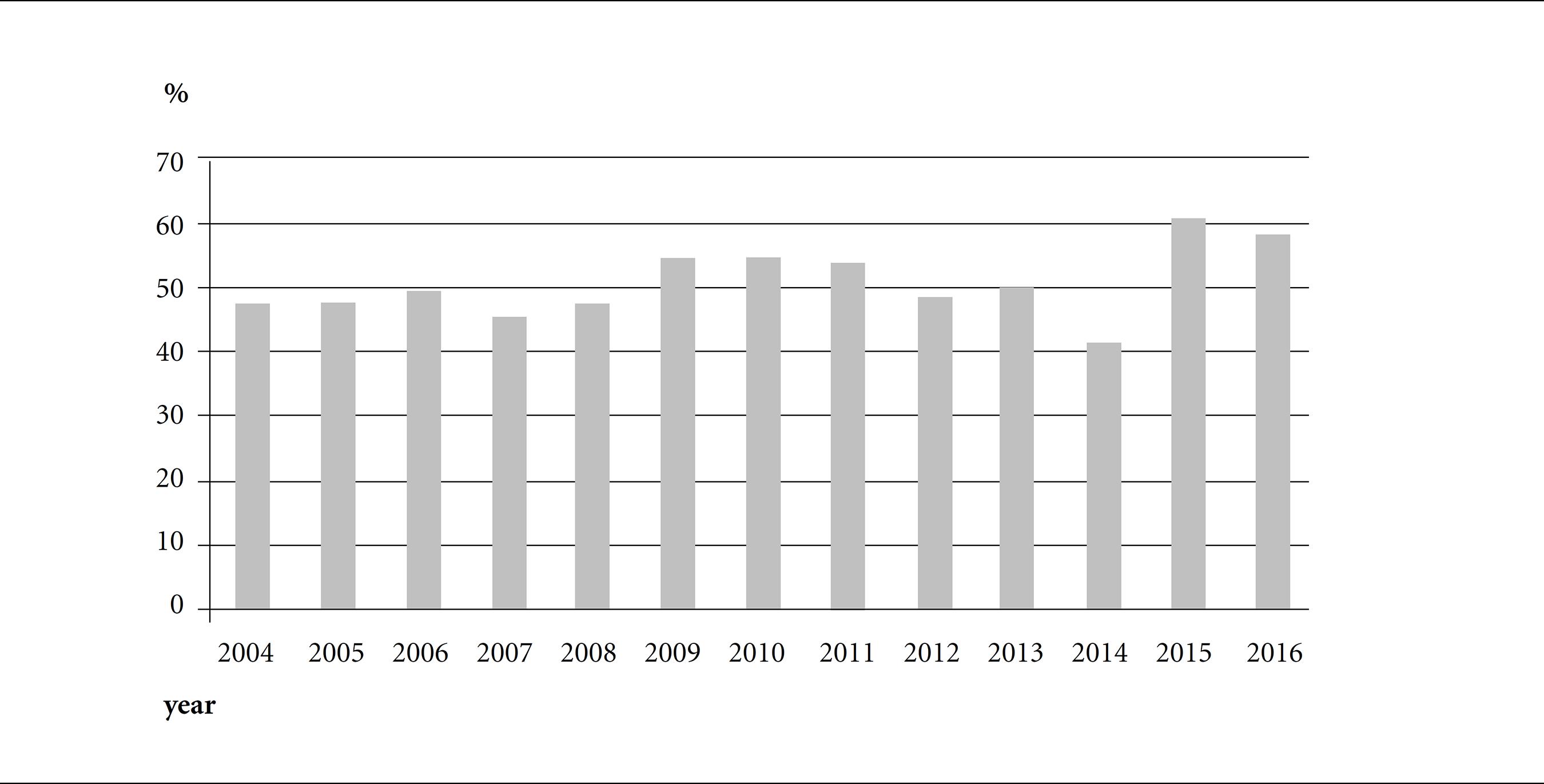
In 2004, the analysis of the annual means of fluorine levels of each locality (Table 2) throughout 12 years found that 21 cities (52.50%) had mean levels within the recommended parameter, and in 2016, this number increased to 32 cities (80.00%). In 2004, 47.76% of samples had values in the range 0.55-0.84 mgF/L, and this increased to 58.22% in 2016 (Graphic 1).
Annual means (and standard deviations) of the fluorine levels (mgF/L) of 40 municipalities in the northwest of São Paulo, from November 2004 to December 2016.
Proportion of water samples from 40 São Paulo municipalities containing fluorides in the range of 0.55 to 0.84 mgF/L, by year.
Fifteen municipalities that initially had mean levels of fluoride below 0.55 mgF/L in their public water supply adapted their levels during for the project: Barbosa, Bento de Abreu, Birigui, Braúna, Brejo Alegre, Buritama, Castilho, Clementina, Glicério, Itapura, Lourdes, Nova Castilho, Santo Antônio do Aracanguá, Sud Mennucci and Valparaiso. However, not all of them could develop the method adequately, as observed in the municipality of Murutinga do Sul, which evidenced fluoride concentrations below the recommended level during the whole period of the study. An improvement was evidenced by comparing the proportion of samples that had values between 0.55 and 0.84 mgF/L in 2004 and 2016 (Graphic 1).
In 2004, considering its means, the municipality of Lavínia had below-recommended levels. Over the years, it began to adjust them, maintaining ideal concentrations for six years. In 2016, its annual average was 0.47 mgF/L. Suzanápolis initially had mean levels of fluoride above the ideal range, which was adequate in the second year, remaining as such until 2011. Then, from this year on, the mean values of fluorine levels decreased and were below the recommended level in 2016.
Discussion
In this study on water fluoridation in municipalities in the state of São Paulo, 50.94% of the analyzed samples were within the recommended range (0.55 to 0.84 mgF/L), based on the criterion of maximum benefit of caries prevention and minimal risk in the development of fluorosis (clinically, this condition causes opaque spots on the enamel of affected teeth, and in more severe cases, can damage the normal mineral structure of the dental element, causing brownish or yellowish regions), and 20.12% were in the range of maximum benefit and moderate risk (0.84 to 1.14 mgF/L). While the classification developed by CECOL assumes 0.55 to 0.84 mgF/L as the ideal range, much is discussed about the range of 0.84 to 1.14 mgF/L, because although it does not provide the minimal risk, it promotes the maximum benefit in preventing tooth decay. Thus, we can consider that 71.06% of the analyzed samples have fluoride levels that ensure maximum efficiency in the prevention of the disease.
The water fluoridation heterocontrol project became a valuable tool that helped for twelve years 15 municipalities that did not meet the minimum levels required adjust fluorine levels in their waters, as well as collaborated with many others towards maintaining the recommended levels. Worth highlighting is the establishment of partnerships between the university, municipalities and health services, since the monthly results systematically sent to water treatment managers, health secretaries and oral health coordinators assisted the municipal managers to better elaborate their strategies and actions, aiming at adapting or changing the operationalization of the method considering the plans of each location.
Joint work and collaborations between the Institutions have proved to be effective, so that in 2016, only three of the 40 municipalities of the DRS-II did not reach the minimum recommended water supply fluorine content, namely, Murutinga (0.35 mgF/L), Suzanápolis (0.34 mgF/L) and Lavínia (0.47 mgF/L). Thus, a thorough analysis should be performed in these locations to identify and remedy the method operationalization’s difficulties, which are mainly related to the maintenance of the available equipment, financial resources to implement the method, human resources training or the complex water distribution network2525 Moimaz SAS, Garbin CAS, Iglesias GF, Chiba FY, Sumida DH, Saliba O. Dificuldades enfrentadas no processo de fluoretação das águas de abastecimento público. Rev Bras Pesq Saúde 2015; 17(1):87-94..
In this context, one of the cities included in the project, Birigui, has a complex distribution network, consisting of Water Treatment Plant (WTP), semi-artesian wells, artesian and deep wells, deep well pipeline joints with WTP and alternative sources, totaling 42 collection points. Some studies performed in this location showed that approximately 51% of their water samples had contents above 0.84 mgF/L2626 Moimaz SAS, Santos LFP. Estudo longitudinal da fluoretação das águas em município com complexa rede de distribuição: dez anos de estudo. Arch Health Invest 2015; 4(5):11-16.,2727 Santos LFP, Chiba FY, Moimaz SAS, Saliba O. Estudo da concentração de flúor nas águas de abastecimento público relacionada às variações pluviais. Rev Ciênc Plural 2016; 2(2):3-13.. It is known that deep wells generally contain high concentrations of fluoride2727 Santos LFP, Chiba FY, Moimaz SAS, Saliba O. Estudo da concentração de flúor nas águas de abastecimento público relacionada às variações pluviais. Rev Ciênc Plural 2016; 2(2):3-13., and this may become a hindrance since the defluoridation processes are expensive, which is a technological challenge, reflected in the technical and economic aspects. One of the suggested strategies to solve this problem was mixing the water to reach the recommended fluoride content and, thus, new pipes were acquired to restructure the distribution network, promoting the combination of deep well water with other abstraction sources to dilute high ion levels. It should be emphasized that while Birigui has most of its average annual fluorine levels in the recommended range, the samples from the collection points of the areas supplied by the deep wells evidence higher values in comparison to their other abstraction sources2828 Moimaz SAS, Saliba NA, Barbosa TF, Garbin CAS, Rovida TAS, Saliba O. Fluoretação das águas de abastecimento público em um município com diferentes fontes de captação. Rev Odontol UNESP 2011; 40(5):203-207..
Thus, we highlight the criteria established by the heterocontrol project developed by FOA-UNESP, when selecting the sample collection points according to the number and location of the water supply sources in the municipality. This is because analyzing the fluorine content and the efficacy of the method based only on the annual mean of the municipality may not represent the real condition to which the entire population is exposed, especially in the locations with different of water abstraction sources. For example, the municipality of Itapura, in 2016, had 0.61 mgF/L and 1.04 mgF/L as the lowest and highest average fluorine content at its collection points, respectively. However, the annual means of the municipality was 0.82 mgF/L. The methodology adopted by the project allows the identification of areas where the population may be exposed to fluoride levels in the waters outside the recommended parameters, thus directing the planning actions in specific regions within the municipality to solve the issue.
The maximum value observed in the samples concerning the fluorine content was 2.19 ppm (parts per million), but it was a one-off result, and high values were not rechecked at this point. One should be watchful when high levels are found repeatedly in the same collection points, a condition that can bring complications, especially the development of dental fluorosis in the population consuming water from this abstraction source.
Meetings were held with water supply managers, health secretaries and oral health coordinators of each city every year since the beginning of the project to update information on the water supply network and operationalization of the fluoridation method, where the main difficulties in controlling the recommended levels of fluoride were verified, analyzed and discussed with the municipal authorities, and discussions about the importance of heterocontrol in the prevention of caries and dental fluorosis were held.
In locations with the highest variability of fluorine levels, meetings were held “in loco” with the technical officer responsible for water treatment to identify and understand the difficulties observed to maintain the recommended values. These events assist municipal authorities and managers in the planning of their public health actions, aiming at ensuring quality water to the entire population, especially in municipalities with more than one gross water abstraction source.
In 2006, a study was carried out with the same 40 municipalities of the DRS-II of the state of São Paulo, in which only 38.19% of the samples collected in them had fluoride contents with acceptable concentrations in their waters2929 Saliba NA, Moimaz SAS, Tiano AVP. Fluoride level in public water supplies of cities from the northwest region of São Paulo State, Brazil. J Appl Oral Sci 2006; 14(5):346-350.. Such research showed that five municipalities had not adopted the fluoridation method in that period. The findings of this study reveal improved control of the water fluoridation process and in the adequacy of the method in the locations. Certain developed countries, especially European high-HDI countries, are withdrawing the method of fluoridation in their water supply. This served as justification for some authors, and even for public information that the measure is outdated and may be exposing people who have access to health risks. The oral health condition of the Brazilian population cannot be compared to the condition of the inhabitants of developed countries.
The significant disparity between the Brazilian regions regarding the value of DMFT3030 Brasil. Ministério da Saúde (MS). SB Brasil 2010: Pesquisa Nacional de Saúde Bucal: resultados principais. Brasília: MS; 2012., which is an index used in epidemiological studies in the dental area to record the number of teeth that are or have been affected by caries, emphasizes that fluoridation is still very necessary in the country, especially in less developed locations, where its inhabitants can hardly have access to gels, varnishes, or other fluoridated products3131 Garbin CAS, Santos LFP, Garbin AJI, Moimaz SAS, Saliba O. Fluoretação da água de abastecimento público: abordagem bioética, legal e política. Bioética 2017; 25(2):328-337..
We found that the method is low-cost and, thus, indicated for the Brazilian population: in São Paulo, the average cost per capita/year was R$ 0.08 (US$ 0.03) in 2003, and the accumulated value from 1985 to 2003 was R$ 1.44 per inhabitant3232 Frias AC, Narvai PC, Araújo ME, Zilbovicius C, Antunes JLF. Custo da fluoretação das águas de abastecimento público, estudo de caso: município de São Paulo, Brasil, período de 1985-2003. Cad Saude Publica 2006; 22(6):1237-1246.. The value is significantly lower when compared with the mean cost of dental procedures, such as restorations, fillings and extractions. International studies have also shown the low price of fluoridation. In 44 Florida (U.S.) locations, the cost was US$ 0.45 per person/year3333 Ringelberg ML, Allen SJ, Brown LJ. Cost of fluoridation: 44 Florida communities. J Public Health Dent 1992; 52(2):75-80.; in the 1980s, in the United States, values found ranged from US$ 0.25 to US$ 0.50 per person/year3434 Newbrun E. The fluoridation war: a scientific dispute or a religious argument? J Public Health Dent 1996; 56(5):246-251..
As previously mentioned, the method’s efficacy has been proven for a long time by several studies1010 Saliba NA, Moimaz SAS, Casotti CA, Pagliari AV. Dental caries of lifetime residents in Baixo Guandu, Brazil, fluoridated since 1953. J Public Health Dent 2008; 68(2):119-121.,1515 Viegas Y, Viegas AR. Análise dos dados de prevalência de cárie dental na cidade de Barretos, SP, Brasil, depois de dez anos de fluoretação da água de abastecimento público. Rev Saude Publica 1985; 19(4):287-299.
16 Viegas Y, Viegas AR. Prevalência de cárie dental na cidade de Campinas, SP, Brasil, depois de quatorze anos de fluoração da água de abastecimento pública. Rev Assoc Paul Cir Dent 1985; 39(5):272-282.
17 Saliba NA, Arcieri RM, Moimaz SAS, Sundefeld MLMM. Redução na prevalência da cárie dentária, após dez anos de fluoretação da água de abastecimento público, no município de Birigui, SP. Brasil. Rev Fac Odontol Lins 1995; 8:41-45.
18 Saliba NA, Saliba O, Ayres JPS, Rey CR. Prevalência de cárie dentária em escolares da cidade de Penápolis-SP. Rev Gaúcha Odontol 1980; 28:287-289.-1919 Saliba NA, Saliba O, Rey CR, Vieira SMM, Ayres JPS. Prevalência da cárie dentária, após 5 anos de fluoretação das águas do sistema público de abastecimento, em escolares de Araçatuba, Estado de São Paulo. Odontól Mod 1981; 8:6-8.. The systematic review by McDonalgh et al.3535 McDonalgh MS, Whiting PF, Wilson PM, Sutton AJ, Chestnutt I, Cooper J, Misso K, Bradley M, Treasure E, Kleijnen J. Systematic review of water fluoridation. BMJ 2000; 321(7265):855-859. on the subject showed that fluoridated regions evidenced more children without caries compared to non-fluoridated areas. Another systematic review work that aimed to analyze the effects of water fluoridation on caries prevention and also on the risks of developing dental fluorosis has shown that the measure is effective in reducing caries levels in the deciduous and permanent dentition in children3636 Iheozor-Ejiofor Z, Worthington HV, Walsh T, O’Malley L, Clarkson JE, Macey R, Alam R, Tugwell P, Welch V, Glenny A. Water fluoridation for the prevention of dental caries. Cochrane Database Syst Rev 2015; 6:CD010856.. There is also evidence that inadequate ion levels in public water supply may be associated with a high incidence of dental caries, considering that it is not enough to adopt the method: the preventive effect is not achieved3737 Brito CA, Garbin RR, Mussi A, Rigo L. Vigilância da concentração de flúor nas águas de abastecimento público na cidade de Passo Fundo - RS. Cad Saúde Coletiva 2016; 24(4):452-459.,3838 Panizzi M, Peres MA. Dez anos de heterocontrole da fluoretação de águas em Chapecó, Estado de Santa Catarina, Brasil. Cad Saude Publica 2008; 24(9):2021-2031. when adequate levels are not maintained continuously.
Regarding the potential harmful effects of fluorine, animal-tested laboratory research has shown that the ion can cause damage to the central nervous system, bone tissue, and other tissues3131 Garbin CAS, Santos LFP, Garbin AJI, Moimaz SAS, Saliba O. Fluoretação da água de abastecimento público: abordagem bioética, legal e política. Bioética 2017; 25(2):328-337.. However, such experiments use much higher doses than those recommended for drinking water and do not prove that fluoridation is harmful but that fluoride can be dangerous if not used with caution. Some authors argue that there seems to be no way out of this moral dilemma, even if the measure were risk-free, since it would still violate the principle of citizen autonomy, and people are not at liberty of refusing to use fluoridated water3939 Cohen H, Locker D. The science and ethics of water fluoridation. J Can Dent Assoc 2001; 67(10):578-580.. If there is no solution from an ethical point of view, decisions regarding the measure must be taken at the political level, which meets some interests and, at the same time, contradicts others, directly interlinking public health and democratic values.
Conclusions
Public water supply fluoridation is a useful public health measure provided for and regulated by law so that public health policymakers should develop strategies or promote partnerships to ensure that all citizens have access to fluoridated water and within recommended standards. Most of the municipalities of this study have fluorine at the recommended levels in their public water supply. Heterocontrol programs are essential strategies that assist in the surveillance of the method, with fundamental participation in the provision of quality water to the population.
Referências
-
1Moimaz SAS, Saliba NA, Saliba O, Sumida DH, Souza NP, Chiba FY, Garbin CAS. Water fluoridation in 40 Brazilian cities: 7 year analysis. J Appl Oral Sci 2013; 21(1):13-19.
-
2Viegas AR. Fluoretação da água de abastecimento público. Rev Bras Med 1989; 46(6): 209-216.
-
3Murray JJ. Uso correto de fluoretos na saúde pública São Paulo: Ed. Santos; 1992.
-
4Centers for Disease Control and Prevention. Achievements in Public Health, 1900-1999: fluoridation of drinking water to prevent dental caries. MMWR 1999; 48(41):933-940.
-
5Arnold Junior FA, Dean HT, Knutson JW. Effect of fluoridated public water supplies on dental caries prevalence. Public Health Rep 1956; 71(7):652-658.
-
6Ast DB, Szwejda LF, Wilcox R. Newburgh-Kingston caries fluorine study. XV. Further observations of dental caries experience among children in Newburgh and Kingston, ages7-16 based on DMF frequency per child. New York J Dent 1958; 28:173-175.
-
7Brown HK, McLaren HR, Stewart B. Brantford fluoridation caries study: 1954 report. J Canad Dent Assoc 1954; 20:585-602.
-
8Galagan DJ, Vermillion JR. Determining optimum fluoride concentrations. Public Health Rep 1957; 72(6):491-493.
-
9Pinto VG. Prevenção da cárie dental. In: Pinto VG. Saúde bucal: odontologia social e preventiva 3ª ed. São Paulo: Santos; 1992. p. 275-328.
-
10Saliba NA, Moimaz SAS, Casotti CA, Pagliari AV. Dental caries of lifetime residents in Baixo Guandu, Brazil, fluoridated since 1953. J Public Health Dent 2008; 68(2):119-121.
-
11Buendia OC. Fluoretação de águas de abastecimento público no Brasil: atualização. Rev Assoc Paul Cir Dent 1984; 38(2):138-158.
-
12Pires Filho FM, Bernd B, Ely HC, Pegoraro MT. Flúor: manual informativo Porto Alegre: SSMA-RS/UFRGS; 1989.
-
13Muniz A. Prevalência da cárie dentária em escolares de Curitiba, antes e após exposição contínua à água fluoretada: 1958-1968 Curitiba: SSP-PR; 1969.
-
14Brasil. Lei nº 6.050, de 24 de maio de 1974. Dispõe sobre a obrigatoriedade da fluoretação das águas em sistema de abastecimento Diário Oficial da União 1974; 27 maio.
-
15Viegas Y, Viegas AR. Análise dos dados de prevalência de cárie dental na cidade de Barretos, SP, Brasil, depois de dez anos de fluoretação da água de abastecimento público. Rev Saude Publica 1985; 19(4):287-299.
-
16Viegas Y, Viegas AR. Prevalência de cárie dental na cidade de Campinas, SP, Brasil, depois de quatorze anos de fluoração da água de abastecimento pública. Rev Assoc Paul Cir Dent 1985; 39(5):272-282.
-
17Saliba NA, Arcieri RM, Moimaz SAS, Sundefeld MLMM. Redução na prevalência da cárie dentária, após dez anos de fluoretação da água de abastecimento público, no município de Birigui, SP. Brasil. Rev Fac Odontol Lins 1995; 8:41-45.
-
18Saliba NA, Saliba O, Ayres JPS, Rey CR. Prevalência de cárie dentária em escolares da cidade de Penápolis-SP. Rev Gaúcha Odontol 1980; 28:287-289.
-
19Saliba NA, Saliba O, Rey CR, Vieira SMM, Ayres JPS. Prevalência da cárie dentária, após 5 anos de fluoretação das águas do sistema público de abastecimento, em escolares de Araçatuba, Estado de São Paulo. Odontól Mod 1981; 8:6-8.
-
20Narvai PC, Frazão P, Fernandez RAC. Fluoretação da água e democracia. Saneas 2004; 2:29-33.
-
21Brasil. Ministério da Saúde (MS). Diretrizes da Política Nacional de Saúde Bucal [acessado 2015 Abr 6]. Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/politica_nacional_brasil_sorridente.pdf
» http://bvsms.saude.gov.br/bvs/publicacoes/politica_nacional_brasil_sorridente.pdf -
22Narvai PC. Cárie dentária e flúor: uma relação do século XX. Cien Saude Colet 2000; 5(2):381-392.
-
23Cury JA, Lima YBO, Vieira Filho W. Análise de flúor com eletrodo específico Campinas: Unicamp; 2001.
-
24Universidade de São Paulo. Consenso técnico sobre classificação de águas de abastecimento público segundo o teor de flúor São Paulo: Universidade de São Paulo; 2011.
-
25Moimaz SAS, Garbin CAS, Iglesias GF, Chiba FY, Sumida DH, Saliba O. Dificuldades enfrentadas no processo de fluoretação das águas de abastecimento público. Rev Bras Pesq Saúde 2015; 17(1):87-94.
-
26Moimaz SAS, Santos LFP. Estudo longitudinal da fluoretação das águas em município com complexa rede de distribuição: dez anos de estudo. Arch Health Invest 2015; 4(5):11-16.
-
27Santos LFP, Chiba FY, Moimaz SAS, Saliba O. Estudo da concentração de flúor nas águas de abastecimento público relacionada às variações pluviais. Rev Ciênc Plural 2016; 2(2):3-13.
-
28Moimaz SAS, Saliba NA, Barbosa TF, Garbin CAS, Rovida TAS, Saliba O. Fluoretação das águas de abastecimento público em um município com diferentes fontes de captação. Rev Odontol UNESP 2011; 40(5):203-207.
-
29Saliba NA, Moimaz SAS, Tiano AVP. Fluoride level in public water supplies of cities from the northwest region of São Paulo State, Brazil. J Appl Oral Sci 2006; 14(5):346-350.
-
30Brasil. Ministério da Saúde (MS). SB Brasil 2010: Pesquisa Nacional de Saúde Bucal: resultados principais Brasília: MS; 2012.
-
31Garbin CAS, Santos LFP, Garbin AJI, Moimaz SAS, Saliba O. Fluoretação da água de abastecimento público: abordagem bioética, legal e política. Bioética 2017; 25(2):328-337.
-
32Frias AC, Narvai PC, Araújo ME, Zilbovicius C, Antunes JLF. Custo da fluoretação das águas de abastecimento público, estudo de caso: município de São Paulo, Brasil, período de 1985-2003. Cad Saude Publica 2006; 22(6):1237-1246.
-
33Ringelberg ML, Allen SJ, Brown LJ. Cost of fluoridation: 44 Florida communities. J Public Health Dent 1992; 52(2):75-80.
-
34Newbrun E. The fluoridation war: a scientific dispute or a religious argument? J Public Health Dent 1996; 56(5):246-251.
-
35McDonalgh MS, Whiting PF, Wilson PM, Sutton AJ, Chestnutt I, Cooper J, Misso K, Bradley M, Treasure E, Kleijnen J. Systematic review of water fluoridation. BMJ 2000; 321(7265):855-859.
-
36Iheozor-Ejiofor Z, Worthington HV, Walsh T, O’Malley L, Clarkson JE, Macey R, Alam R, Tugwell P, Welch V, Glenny A. Water fluoridation for the prevention of dental caries. Cochrane Database Syst Rev 2015; 6:CD010856.
-
37Brito CA, Garbin RR, Mussi A, Rigo L. Vigilância da concentração de flúor nas águas de abastecimento público na cidade de Passo Fundo - RS. Cad Saúde Coletiva 2016; 24(4):452-459.
-
38Panizzi M, Peres MA. Dez anos de heterocontrole da fluoretação de águas em Chapecó, Estado de Santa Catarina, Brasil. Cad Saude Publica 2008; 24(9):2021-2031.
-
39Cohen H, Locker D. The science and ethics of water fluoridation. J Can Dent Assoc 2001; 67(10):578-580.
Publication Dates
-
Publication in this collection
08 July 2020 -
Date of issue
July 2020
History
-
Received
16 Feb 2018 -
Accepted
03 Oct 2018 -
Published
05 Oct 2018