Abstract
Some patients with coronavirus disease (COVID-19) present with severe acute respiratory syndrome, which causes multiple organ dysfunction, besides dysfunction of the respiratory system, that requires invasive procedures. On the basis of the opinions of front-line experts and a review of the relevant literature on several topics, we proposed clinical practice recommendations on the following aspects for physiotherapists facing challenges in treating patients and containing virus spread: 1. personal protective equipment, 2. conventional chest physiotherapy, 3. exercise and early mobilization, 4. oxygen therapy, 5. nebulizer treatment, 6. non-invasive ventilation and high-flow nasal oxygen, 7. endotracheal intubation, 8. protective mechanical ventilation, 9. management of mechanical ventilation in severe and refractory cases of hypoxemia, 10. prone positioning, 11. cuff pressure, 12. tube and nasotracheal suction, 13. humidifier use for ventilated patients, 14. methods of weaning ventilated patients and extubation, and 15. equipment and hand hygiene. These recommendations can serve as clinical practice guidelines for physiotherapists. This article details the development of guidelines on these aspects for physiotherapy of patients with COVID-19.
COVID-19; Physiotherapy; Mechanical Ventilation; Oxygen Therapy; Severe Acute Respiratory Syndrome Coronavirus 2
INTRODUCTION
The current outbreak of coronavirus disease 2019 (COVID-19) originated in the Hubei Province of the People’s Republic of China (11. Weston S, Frieman MB. COVID-19: Knowns, Unknowns, and Questions. mSphere. 2020;5(2):e00203-20. https://doi.org/10.1128/mSphere.00203-20.
https://doi.org/10.1128/mSphere.00203-20...
,22. World Health Organization. Clinical management of severe acute respiratory infection when COVID-19 is suspected. 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected. [Accessed March 24th, 2020].
https://www.who.int/publications-detail/...
), and on March 11, 2020, it was declared a pandemic by the World Health Organization Emergency Committee (22. World Health Organization. Clinical management of severe acute respiratory infection when COVID-19 is suspected. 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected. [Accessed March 24th, 2020].
https://www.who.int/publications-detail/...
).
The most common symptoms include fever (89%), cough (68%), fatigue (38%), sputum production (34%), and shortness of breath (19%) (33. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020;382(18):1708-20. https://doi.org/10.1056/NEJMoa2002032.
https://doi.org/10.1056/NEJMoa2002032...
). A considerable proportion of the population with COVID-19 will not require hospitalization as the patients present a mild or uncomplicated form of the disease with a favorable prognosis. However, older patients and those with chronic underlying conditions can develop severe illness and present complications such as acute respiratory disease syndrome (ARDS), sepsis, septic shock, and kidney and cardiac failure, which require treatment in an intensive care unit (ICU) with invasive support (44. Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, et al. Clinical Course and Outcomes of Critically Ill Patients With SARS-CoV-2 Pneumonia in Wuhan, China: A Single-Centered, Retrospective, Observational Study. Lancet Respir Med. 2020;8(5):475-81. https://doi.org/10.1016/S2213-2600(20)30079-5.
https://doi.org/10.1016/S2213-2600(20)30...
). Approximately 14% of patients develop a severe form of COVID-19, requiring hospitalization, and 5% require admission to an ICU (55. Grasselli G, Presenti A, Cecconi M. Critical Care Utilization for the COVID-19 Outbreak in Lombardy, Italy: Early Experience and Forecast During an Emergency Response. JAMA. 2020. https://doi.org/10.1001/jama.2020.4031
https://doi.org/10.1001/jama.2020.4031...
).
Physiotherapists are recognized in several countries as professionals working in primary and tertiary care (66. Jerre G, Beraldo MA, Silva Tde J, Gastaldi A, Kondo C, Leme F, et al. [Physiotherapy on the Mechanically Ventilated Patients]. J Bras Pneumol. 2007;33(Suppl 2):S142-50. https://doi.org/10.1590/S1806-37132007000800010.
https://doi.org/10.1590/S1806-3713200700...
7. Stiller K. Physiotherapy in intensive care: an updated systematic review. Chest. 2013;144(3):825-47. https://doi.org/10.1378/chest.12-2930.
https://doi.org/10.1378/chest.12-2930...
-88. Spruit MA. Pulmonary rehabilitation. Eur Respir Rev. 2014;23(131):55-63. https://doi.org/10.1183/09059180.00008013.
https://doi.org/10.1183/09059180.0000801...
) who play a fundamental role in multi-professional teams providing ventilatory support during the acute illness phase and rehabilitation interventions thereafter to promote functionality (99. Ambrosino N, Makhabah DN. Comprehensive physiotherapy management in ARDS. Minerva Anestesiol. 2013;79(5):554-63.,1010. Goãi-Viguria R, Yoldi-Arzoz E, Casajús-Sola L, Aquerreta-Larraya T, Fernández-Sangil P, Guzmán-Unamuno E, et al. Respiratory Physiotherapy in Intensive Care Unit: Bibliographic Review. Enferm Intensiva. 2018;29(4):168-81. https://doi.org/10.1016/j.enfi.2018.03.003.
https://doi.org/10.1016/j.enfi.2018.03.0...
).
This paper describes the different actions and practices adopted by the Rehabilitation Service of Hospital Sírio-Libanês (São Paulo, Brazil) to face the challenges in treating and containing the spread of COVID-19. Issues pertaining to clinical practice in the adult hospital setting were identified on the basis of the experience and opinions of front-line experts as well as a review of the relevant literature.
To provide the maximum level of care and ensure staff protection, recommendations were developed regarding protective equipment, conventional chest physiotherapy, exercise and early mobilization, oxygen therapy, nebulizer treatment, non-invasive ventilation and high-flow nasal oxygen, endotracheal intubation, protective mechanical ventilation, management of mechanical ventilation in severe and refractory cases of hypoxemia, prone positioning, cuff pressure, tube and nasotracheal suction, humidifier use for ventilated patients, methods of weaning ventilated patients, and equipment and hand hygiene.
PERSONAL PROTECTIVE EQUIPMENT (PPE)
Several procedures performed by physiotherapists may generate aerosols and droplets, which are sources of lung and respiratory pathogens. These procedures include non-invasive ventilation, high-flow oxygenation, endotracheal intubation, airway tracheostomy and endotracheal tube suction, cardiopulmonary resuscitation, high-frequency oscillatory ventilation, chest physiotherapy, prone patient positioning, disconnection of the ventilator, administration of nebulized treatment, and sputum induction (1111. Lim WS, Anderson SR, Read RC. SARS Guidelines Committee of the British Thoracic Society; British Infection Society; Health Protection Agency. Hospital management of adults with severe acute respiratory syndrome (SARS) if SARS re-emerges—updated 10 February 2004. J Infect. 2004;49(1):1-7. https://doi.org/10.1016/j.jinf.2004.04.001.
https://doi.org/10.1016/j.jinf.2004.04.0...
12. Livingston E, Desai A, Berkwits M. Sourcing Personal Protective Equipment During the COVID-19 Pandemic. JAMA. 2020. https://doi.org/10.1001/jama.2020.5317
https://doi.org/10.1001/jama.2020.5317...
13. Carlson AL, Budd AP, Perl TM. Control of Influenza in Healthcare Settings: Early Lessons From the 2009 Pandemic. Curr Opin Infect Dis. 2010;23(4):293-9. https://doi.org/10.1097/QCO.0b013e32833bb804.
https://doi.org/10.1097/QCO.0b013e32833b...
-1414. Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol Generating Procedures and Risk of Transmission of Acute Respiratory Infections to Healthcare Workers: A Systematic Review. PLoS One. 2012;7(4):e35797. https://doi.org/10.1371/journal.pone.0035797
https://doi.org/10.1371/journal.pone.003...
). Furthermore, severe acute respiratory syndrome coronavirus 2 can remain in the air for hours and on surfaces of various materials for days upon aerosolization, with risks of possible human infection (1515. van Doremalen N, Bushmaker T, Morris DH, Holbrook MG, Gamble A, Williamson BN, et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N Engl J Med. 2020;382(16):1564-7. https://doi.org/10.1056/NEJMc2004973.
https://doi.org/10.1056/NEJMc2004973...
). However, when aerosol-generating procedures cannot be avoided, they should be performed in a negative-pressure room. In the absence of negative-pressure rooms, the procedures must be performed in a room with closed doors and open windows; with minimum number of qualified professionals to perform the procedures; with appropriate PPE; and avoiding the presence other people (1616. Cheung JC, Ho LT, Cheng JV, Cham EYK, Lam KN. Staff safety during emergency airway management for COVID-19 in Hong Kong. Lancet Respir Med. 2020;8(4):e19. https://doi.org/10.1016/S2213-2600(20)30084-9
https://doi.org/10.1016/S2213-2600(20)30...
,1717. World Health Organization. Rational use of personal protective equipment (PPE) for coronavirus disease (COVID-19): interim guidance, 19 March 2020. Available from: https://apps.who.int/iris/handle/10665/331498. [Accessed March 20th, 2020].
https://apps.who.int/iris/handle/10665/3...
). Therefore, physiotherapists must adopt protective measures to avoid aerosol exposure and for contact isolation by using adequate PPE, namely, surgical caps, safety goggles, face shields, N95 masks or equivalent, gowns, and gloves (1717. World Health Organization. Rational use of personal protective equipment (PPE) for coronavirus disease (COVID-19): interim guidance, 19 March 2020. Available from: https://apps.who.int/iris/handle/10665/331498. [Accessed March 20th, 2020].
https://apps.who.int/iris/handle/10665/3...
18. Milton DK, Fabian MP, Cowling BJ, Grantham ML, McDevitt JJ. Influenza Virus Aerosols in Human Exhaled Breath: Particle Size, Culturability, and Effect of Surgical Masks. PLoS Pathog. 2013;9(3):e1003205. https://doi.org/10.1371/journal.ppat.1003205
https://doi.org/10.1371/journal.ppat.100...
-1919. Ferioli M, Cisternino C, Leo V, Pisani L, Palange P, Nava S. Protecting healthcare workers from SARS-CoV-2 infection: practical indications. Eur Respir Rev. 2020;29(155):200068. https://doi.org/10.1183/16000617.0068-2020
https://doi.org/10.1183/16000617.0068-20...
).
CONVENTIONAL CHEST PHYSIOTHERAPY
Currently, no evidence exists indicating that conventional chest physiotherapy changes the course of COVID-19 in the acute phase of the disease in patients with hypoxemic respiratory failure and dry cough. However, some patients with productive cough may benefit from bronchial hygiene maneuvers and techniques that stimulate coughing (2020. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical Features of Patients Infected With 2019 Novel Coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-506. https://doi.org/10.1016/S0140-6736(20)30183-5.
https://doi.org/10.1016/S0140-6736(20)30...
,2121. Cabillic M, Gouilly P, Reychler G. [Manual Airway Clearance Techniques in Adults and Adolescents: What Level of Evidence?]. Rev Mal Respir. 2018;35(5):495-520. https://doi.org/10.1016/j.rmr.2015.12.004.
https://doi.org/10.1016/j.rmr.2015.12.00...
). Patients with a mild form of the disease should be instructed to perform breathing exercises independently. Patients with moderate and severe conditions should be constantly monitored for pulmonary disease (2222. Chinese Association of Rehabilitation Medicine; Respiratory Rehabilitation Committee of Chinese Association of Rehabilitation Medicine; Cardiopulmonary Rehabilitation Group of Chinese Society of Physical Medicine and Rehabilitation. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43(4):308-14. https://doi.org/10.3760/cma.j.cn112147-20200228-00206.
https://doi.org/10.3760/cma.j.cn112147-2...
). In these cases, physiotherapists should contact the patient only for respiratory and pulmonary assessments, especially during orotracheal intubation and oxygen supplementation and for patients who are candidates for non-invasive ventilation or high-flow oxygen administration (2222. Chinese Association of Rehabilitation Medicine; Respiratory Rehabilitation Committee of Chinese Association of Rehabilitation Medicine; Cardiopulmonary Rehabilitation Group of Chinese Society of Physical Medicine and Rehabilitation. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43(4):308-14. https://doi.org/10.3760/cma.j.cn112147-20200228-00206.
https://doi.org/10.3760/cma.j.cn112147-2...
,2323. Alhazzani W, Møller MH, Arabi YM, Loeb M, Gong MN, Fan E, et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Crit Care Med. 2020;48(6):e440-e469. https://doi.org/10.1097/CCM.0000000000004363
https://doi.org/10.1097/CCM.000000000000...
). The professional exposure time should be the minimum necessary for evaluation and assistance (2222. Chinese Association of Rehabilitation Medicine; Respiratory Rehabilitation Committee of Chinese Association of Rehabilitation Medicine; Cardiopulmonary Rehabilitation Group of Chinese Society of Physical Medicine and Rehabilitation. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43(4):308-14. https://doi.org/10.3760/cma.j.cn112147-20200228-00206.
https://doi.org/10.3760/cma.j.cn112147-2...
,2424. Cheng HY, Jian SW, Liu DP, Ng TC, Huang WT, Lin HH, et al. Contact Tracing Assessment of COVID-19 Transmission Dynamics in Taiwan and Risk at Different Exposure Periods Before and After Symptom Onset. JAMA Intern Med. 2020. https://doi.org/10.1001/jamainternmed.2020.2020
https://doi.org/10.1001/jamainternmed.20...
).
EXERCISE AND EARLY MOBILIZATION
Patients usually present with a debilitated physical condition because of the disease, which reduces their exercise capacity, especially when they present with fever, dyspnea, myalgia, and fatigue (2020. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical Features of Patients Infected With 2019 Novel Coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-506. https://doi.org/10.1016/S0140-6736(20)30183-5.
https://doi.org/10.1016/S0140-6736(20)30...
); the debilitated physical condition can also be a result of prolonged mechanical ventilation and immobilization. Hospitalized patients, even those with moderate disease severity, can spend weeks in hospital isolation, with a significant decrease in their activity levels, and are thus prone to a reduction in their muscle strength and cardiorespiratory capacity (2525. Hartley P, Costello P, Fenner R, Gibbins N, Quinn É, Kuhn I, et al. Change in skeletal muscle associated with unplanned hospital admissions in adult patients: A systematic review and meta-analysis. PLoS One. 2019;14(1):e0210186. https://doi.org/10.1371/journal.pone.0210186
https://doi.org/10.1371/journal.pone.021...
). Therefore, patients in the acute phase with mild disease should be encouraged to perform light-intensity exercises to maintain minimal functional capacity. The exercises can be tailored for maintenance of a Borg rating of <3 (on a 10-point scale) (2222. Chinese Association of Rehabilitation Medicine; Respiratory Rehabilitation Committee of Chinese Association of Rehabilitation Medicine; Cardiopulmonary Rehabilitation Group of Chinese Society of Physical Medicine and Rehabilitation. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43(4):308-14. https://doi.org/10.3760/cma.j.cn112147-20200228-00206.
https://doi.org/10.3760/cma.j.cn112147-2...
). Although there are no studies specific to patients with COVID-19, classically critical patients who underwent early mobilization showed a reduction in delirium and duration of mechanical ventilation (2626. Schweickert WD, Pohlman MC, Pohlman AS, Nigos C, Pawlik AJ, Esbrook CL, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet. 2009;373(9678):1874-82. https://doi.org/10.1016/S0140-6736(09)60658-9.
https://doi.org/10.1016/S0140-6736(09)60...
); thus, early mobilization should be started as soon as possible, as long as the patient presents suitable clinical conditions (2727. Aquim EE, Bernardo WM, Buzzini RF, Azeredo NSG, Cunha LSD, Damasceno MCP, et al. Brazilian Guidelines for Early Mobilization in Intensive Care Unit. Rev Bras Ter Intensiva. 2019;31(4):434-43. https://doi.org/10.5935/0103-507X.20190084.
https://doi.org/10.5935/0103-507X.201900...
). This mobilization can include neuromuscular stimulation, therapeutic exercises, and early verticalization (2828. Hodgson CL, Berney S, Harrold M, Saxena M, Bellomo R. Clinical review: early patient mobilization in the ICU. Crit Care. 2013;17(1):207. https://doi.org/10.1186/cc11820
https://doi.org/10.1186/cc11820...
29. Hashem MD, Nelliot A, Needham DM. Early Mobilization and Rehabilitation in the ICU: Moving Back to the Future. Respir Care. 2016;61(7):971-9. https://doi.org/10.4187/respcare.04741.
https://doi.org/10.4187/respcare.04741...
30. Jang MH, Shin MJ, Shin YB. Pulmonary and Physical Rehabilitation in Critically Ill Patients. Acute Crit Care. 2019;34(1):1-13. https://doi.org/10.4266/acc.2019.00444.
https://doi.org/10.4266/acc.2019.00444...
-3131. Murakami FM, Yamaguti WP, Onoue MA, Mendes JM, Pedrosa RS, Maida AL, et al. Functional evolution of critically ill patients undergoing an early rehabilitation protocol. Rev Bras Ter Intensiva. 2015;27(2):161-9. https://doi.org/10.5935/0103-507X.20150028.
https://doi.org/10.5935/0103-507X.201500...
).
OXYGEN THERAPY
The prevalence of hypoxic respiratory failure in adults with COVID-19 is 19%; thus, oxygen therapy represents a major treatment intervention for patients with severe pulmonary dysfunction (22. World Health Organization. Clinical management of severe acute respiratory infection when COVID-19 is suspected. 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected. [Accessed March 24th, 2020].
https://www.who.int/publications-detail/...
,3232. Wu Z, McGoogan JM. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA. 2020. https://doi.org/10.1001/jama.2020.2648
https://doi.org/10.1001/jama.2020.2648...
). Adults with COVID-19 should be started on supplemental oxygen if the peripheral oxygen saturation (SpO2) is <93% and maintained oxygen saturation is no higher than 96% (2323. Alhazzani W, Møller MH, Arabi YM, Loeb M, Gong MN, Fan E, et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Crit Care Med. 2020;48(6):e440-e469. https://doi.org/10.1097/CCM.0000000000004363
https://doi.org/10.1097/CCM.000000000000...
). Mechanical ventilation may be necessary in cases of respiratory failure refractory to oxygen therapy (22. World Health Organization. Clinical management of severe acute respiratory infection when COVID-19 is suspected. 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected. [Accessed March 24th, 2020].
https://www.who.int/publications-detail/...
,2323. Alhazzani W, Møller MH, Arabi YM, Loeb M, Gong MN, Fan E, et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Crit Care Med. 2020;48(6):e440-e469. https://doi.org/10.1097/CCM.0000000000004363
https://doi.org/10.1097/CCM.000000000000...
).
The interfaces used for oxygen supplementation can generate aerosols. Therefore, health care workers should take adequate precautions and wear proper PPE when providing respiratory support to patients with COVID-19 complicated by respiratory failure (1919. Ferioli M, Cisternino C, Leo V, Pisani L, Palange P, Nava S. Protecting healthcare workers from SARS-CoV-2 infection: practical indications. Eur Respir Rev. 2020;29(155):200068. https://doi.org/10.1183/16000617.0068-2020
https://doi.org/10.1183/16000617.0068-20...
,3333. Hui DS, Chow BK, Chu L, Ng SS, Lai ST, Gin T, et al. Exhaled Air Dispersion and Removal Is Influenced by Isolation Room Size and Ventilation Settings During Oxygen Delivery via Nasal Cannula. Respirology. 2011;16(6):1005-13. https://doi.org/10.1111/j.1440-1843.2011.01995.x.
https://doi.org/10.1111/j.1440-1843.2011...
). Oxygen humidification should not be used (3434. Wen Z, Wang W, Zhang H, Wu C, Ding J, Shen M. Is Humidified Better Than Non-Humidified Low-Flow Oxygen Therapy? A Systematic Review and Meta-Analysis. J Adv Nurs. 2017;73(11):2522-33. https://doi.org/10.1111/jan.13323.
https://doi.org/10.1111/jan.13323...
). The prescription of moisturizers such as self-applied nasal sodium chloride gel may be suggested for complications such as dryness of the upper airways or epistaxis. The oxygen supply device should be changed if these complications persist.
Figure 1 shows our institutional proposal for oxygen therapy and early transfer to the ICU for patients with respiratory distress and hypoxemia on the basis of the Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19).
Proposal for oxygen therapy and early transfer to intensive care units for patients with respiratory distress and hypoxemia based on Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). SaO2: arterial oxygen saturation; ICU: intensive care unit; PPE: Personal protective equipment; NIV: non-invasive ventilation; HFNO: high-flow nasal oxygen.
NEBULIZER TREATMENT
All forms of nebulization (including inhalation) are potential aerosol generators and should be avoided (22. World Health Organization. Clinical management of severe acute respiratory infection when COVID-19 is suspected. 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected. [Accessed March 24th, 2020].
https://www.who.int/publications-detail/...
,3535. Simonds AK, Hanak A, Chatwin M, Morrell M, Hall A, Parker KH, et al. Evaluation of droplet dispersion during non-invasive ventilation, oxygen therapy, nebuliser treatment and chest physiotherapy in clinical practice: implications for management of pandemic influenza and other airborne infections. Health Technol Assess. 2010;14(46):131-72. https://doi.org/10.3310/hta14460-02.
https://doi.org/10.3310/hta14460-02...
). Bronchodilators should be administered with metering units (puff or spray) in an air chamber/spacer (22. World Health Organization. Clinical management of severe acute respiratory infection when COVID-19 is suspected. 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected. [Accessed March 24th, 2020].
https://www.who.int/publications-detail/...
).
NON-INVASIVE VENTILATION AND HIGH-FLOW NASAL OXYGEN
For the treatment of acute hypoxemic respiratory failure, the use of high-flow nasal oxygen is suggested over conventional oxygen therapy and non-invasive positive pressure ventilation (3636. Frat JP, Thille AW, Mercat A, Girault C, Ragot S, Perbet S, et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med. 2015;372(23):2185-96. https://doi.org/10.1056/NEJMoa1503326.
https://doi.org/10.1056/NEJMoa1503326...
37. Ni YN, Luo J, Yu H, Liu D, Liang BM, Liang ZA. The Effect of High-Flow Nasal Cannula in Reducing the Mortality and the Rate of Endotracheal Intubation When Used Before Mechanical Ventilation Compared With Conventional Oxygen Therapy and Noninvasive Positive Pressure Ventilation. A Systematic Review and Meta-Analysis. Am J Emerg Med. 2018;36(2):226-33. https://doi.org/10.1016/j.ajem.2017.07.083.
https://doi.org/10.1016/j.ajem.2017.07.0...
-3838. Ou X, Hua Y, Liu J, Gong C, Zhao W. Effect of high-flow nasal cannula oxygen therapy in adults with acute hypoxemic respiratory failure: a meta-analysis of randomized controlled trials. CMAJ. 2017;189(7):E260-E267. https://doi.org/10.1503/cmaj.160570
https://doi.org/10.1503/cmaj.160570...
). If high-flow nasal oxygen is not available, a trial of non-invasive ventilation is suggested (3939. Poston JT, Patel BK, Davis AM. Management of Critically Ill Adults With COVID-19. JAMA. 2020. https://doi.org/10.1001/jama.2020.4914
https://doi.org/10.1001/jama.2020.4914...
). An experiment in a human model showed that non-invasive ventilation or high-flow nasal oxygen, when well applied with an optimal fit, resulted in minimal aerosolization of exhaled air (4040. Hui DS, Chow BK, Lo T, Tsang OTY, Ko FW, Ng SS, et al. Exhaled air dispersion during high-flow nasal cannula therapy versus CPAP via different masks. Eur Respir J. 2019;53(4):1802339. https://doi.org/10.1183/13993003.02339-2018
https://doi.org/10.1183/13993003.02339-2...
). However, the specific models of masks and interfaces tested in the study are not universally used in all hospitals. Therefore, to avoid potential harm, we recommend using adequate precautions and PPE and discourage the use of this procedure if an airborne infection isolation room is unavailable (22. World Health Organization. Clinical management of severe acute respiratory infection when COVID-19 is suspected. 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected. [Accessed March 24th, 2020].
https://www.who.int/publications-detail/...
,1616. Cheung JC, Ho LT, Cheng JV, Cham EYK, Lam KN. Staff safety during emergency airway management for COVID-19 in Hong Kong. Lancet Respir Med. 2020;8(4):e19. https://doi.org/10.1016/S2213-2600(20)30084-9
https://doi.org/10.1016/S2213-2600(20)30...
). Monitoring for worsening respiratory status and subsequent early intubation is recommended (3939. Poston JT, Patel BK, Davis AM. Management of Critically Ill Adults With COVID-19. JAMA. 2020. https://doi.org/10.1001/jama.2020.4914
https://doi.org/10.1001/jama.2020.4914...
).
Patient candidates for non-invasive ventilation admitted to the ICU in negative-pressure rooms must be ventilated with positive end-expiratory pressure (PEEP) ≥8 cmH2O, support pressure for a tidal volume (TV) ≤8 mL/kg of the predicted weight, and fraction of inspired oxygen (FiO2) to maintain SaO2 >92%. Facial or full-face masks must be used during application of the ventilator. Devices with double branches for ventilation are indicated in these cases, with a heat moisture exchange filter (HMEF) between the face mask and the device and another high-efficiency particulate arrestance (HEPA) filter on the exhalation outlet of the ventilator. For high-flow oxygen, a flow rate of 40 to 50 L/min should be maintained, and FiO2 to maintain SaO2 >92% should be started.
The criteria for orotracheal intubation and invasive mechanical ventilation are FiO2 >60% in non-invasive ventilation or TV ≥9 mL/kg or inability to tolerate <2 hours without non-invasive ventilation or presence of other organic dysfunctions. For high-flow oxygen, the criteria for orotracheal intubation are FiO2 >60% or signs of respiratory distress, or other organic dysfunctions. It is important to reassess the patient after 30 to 60 minutes; if there is no improvement or if there is worsening of ventilatory parameters, endotracheal intubation and invasive mechanical ventilation should be considered (Figure 2) (22. World Health Organization. Clinical management of severe acute respiratory infection when COVID-19 is suspected. 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected. [Accessed March 24th, 2020].
https://www.who.int/publications-detail/...
,2323. Alhazzani W, Møller MH, Arabi YM, Loeb M, Gong MN, Fan E, et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Crit Care Med. 2020;48(6):e440-e469. https://doi.org/10.1097/CCM.0000000000004363
https://doi.org/10.1097/CCM.000000000000...
,3636. Frat JP, Thille AW, Mercat A, Girault C, Ragot S, Perbet S, et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med. 2015;372(23):2185-96. https://doi.org/10.1056/NEJMoa1503326.
https://doi.org/10.1056/NEJMoa1503326...
37. Ni YN, Luo J, Yu H, Liu D, Liang BM, Liang ZA. The Effect of High-Flow Nasal Cannula in Reducing the Mortality and the Rate of Endotracheal Intubation When Used Before Mechanical Ventilation Compared With Conventional Oxygen Therapy and Noninvasive Positive Pressure Ventilation. A Systematic Review and Meta-Analysis. Am J Emerg Med. 2018;36(2):226-33. https://doi.org/10.1016/j.ajem.2017.07.083.
https://doi.org/10.1016/j.ajem.2017.07.0...
-3838. Ou X, Hua Y, Liu J, Gong C, Zhao W. Effect of high-flow nasal cannula oxygen therapy in adults with acute hypoxemic respiratory failure: a meta-analysis of randomized controlled trials. CMAJ. 2017;189(7):E260-E267. https://doi.org/10.1503/cmaj.160570
https://doi.org/10.1503/cmaj.160570...
).
Proposal for non-invasive ventilation and high-flow nasal oxygen for patients with COVID-19. NIV: non-invasive ventilation; EPAP: expiratory positive airway pressure; IPAP: inspiratory positive airway pressure; TV: tidal volume; FiO2: fraction of inspired oxygen; HFNO: high-flow nasal oxygen; SaO2: arterial oxygen saturation.
ENDOTRACHEAL INTUBATION
When aerosol-generating procedures are required, they are recommended to be performed in a negative-pressure room and with the use of appropriate PPE (1616. Cheung JC, Ho LT, Cheng JV, Cham EYK, Lam KN. Staff safety during emergency airway management for COVID-19 in Hong Kong. Lancet Respir Med. 2020;8(4):e19. https://doi.org/10.1016/S2213-2600(20)30084-9
https://doi.org/10.1016/S2213-2600(20)30...
). Only the professionals needed to perform orotracheal intubation should remain in the room.
Patients with COVID‐19 are at risk of a rapid decrease in arterial oxygen levels; therefore, effective pre-oxygenation is mandatory. Patients must be administered a sufficient oxygen flow to maintain SpO2 >93%, and intubation should be performed with a rapid sequence of induction and intubation. Pre-oxygenation with a non-rebreather mask with the lowest possible airflow to maintain effective oxygenation (SpO2 >93%) (4141. Orser BA. Recommendations for Endotracheal Intubation of COVID-19 Patients. Anesth Analg. 2020;130(5):1109-10. https://doi.org/10.1213/ANE.0000000000004803.
https://doi.org/10.1213/ANE.000000000000...
) is required. It is also important to avoid assisted ventilation with the Bag-Valve-Mask device or the use of a supraglottic device because of the potential for aerosolization and contamination of health workers. However, if necessary, we suggest adding a filter between the simple respirator and the Bag-Valve-Mask or artificial airway during use (Figure 3) to reduce the spread of the virus in the patient's airway to the indoor air (1919. Ferioli M, Cisternino C, Leo V, Pisani L, Palange P, Nava S. Protecting healthcare workers from SARS-CoV-2 infection: practical indications. Eur Respir Rev. 2020;29(155):200068. https://doi.org/10.1183/16000617.0068-2020
https://doi.org/10.1183/16000617.0068-20...
).
Bag-Valve-Mask device: (A) face mask, (B) heat moisture exchange filter, and (C) Bag-Valve-Mask.
After orotracheal intubation, checking the proper positioning of the orotracheal tube and inflating the cuff are recommended. The patient can then be connected to the ventilator associated with the HMEF and with a HEPA filter in the expiratory valve of the mechanical ventilator. These filters can filter bacteria and viruses and reduce room contamination (22. World Health Organization. Clinical management of severe acute respiratory infection when COVID-19 is suspected. 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected. [Accessed March 24th, 2020].
https://www.who.int/publications-detail/...
,4141. Orser BA. Recommendations for Endotracheal Intubation of COVID-19 Patients. Anesth Analg. 2020;130(5):1109-10. https://doi.org/10.1213/ANE.0000000000004803.
https://doi.org/10.1213/ANE.000000000000...
42. Sorbello M, El-Boghdadly K, Di Giacinto I, Cataldo R, Esposito C, Falcetta S, et al. The Italian coronavirus disease 2019 outbreak: recommendations from clinical practice. Anaesthesia. 2020;75(6):724-32. https://doi.org/10.1111/anae.15049.
https://doi.org/10.1111/anae.15049...
-4343. Respiratory Care Committee of Chinese Thoracic Society. [Expert consensus on preventing nosocomial transmission during respiratory care for critically ill patients infected by 2019 novel coronavirus pneumonia]. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43(4):288-96. https://doi.org/10.3760/cma.j.cn112147-20200304-00239.
https://doi.org/10.3760/cma.j.cn112147-2...
). Airway interventions must be carried out by experienced individuals. After each procedure, appropriate hand hygiene is required (4141. Orser BA. Recommendations for Endotracheal Intubation of COVID-19 Patients. Anesth Analg. 2020;130(5):1109-10. https://doi.org/10.1213/ANE.0000000000004803.
https://doi.org/10.1213/ANE.000000000000...
).
PROTECTIVE MECHANICAL VENTILATION
Invasive mechanical mode volume-controlled ventilation (in the presence of neuromuscular block or the absence of inspiratory effort) or pressure-controlled ventilation (in the absence of neuromuscular block and mild respiratory effort and asynchrony) should be performed with lower TVs (4 to 6 mL/kg predicted body weight) and lower inspiratory pressures, reaching a plateau pressure (Pplat) of <28-30 cmH2O (4444. Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2017;195(9):1253-63. https://doi.org/10.1164/rccm.201703-0548ST.
https://doi.org/10.1164/rccm.201703-0548...
). The PEEP must be as high as possible to maintain the driving pressure (Pplat − PEEP) as low as possible (<15 cmH2O) and SpO2 88-95% (4444. Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2017;195(9):1253-63. https://doi.org/10.1164/rccm.201703-0548ST.
https://doi.org/10.1164/rccm.201703-0548...
,4545. NHLBI ARDS Network Tools [website]. Available from: http://www.ardsnet.org/tools.shtml [Accessed March 18th, 2020]
http://www.ardsnet.org/tools.shtml...
). Moreover, disconnection from the invasive mechanical ventilator must be avoided to prevent loss of PEEP and consequent atelectasis.
MANAGEMENT OF MECHANICAL VENTILATION IN SEVERE AND REFRACTORY CASES OF HYPOXEMIA
For patients with PaO2/FiO2 <150 and an inability to maintain protective ventilation or with the presence of asynchrony or severe hypercapnia (pH <7.25), we suggest sedation and continuous neuromuscular block to reduce respiratory drive and maintain protective ventilation. The multidisciplinary team can discuss the following: 1. prone positioning; 2. alveolar recruitment maneuvers and PEEP adjustment for better pulmonary compliance; 3. recruitment in the prone position for patients who responded to the supine recruitment maneuver; 4. nitric oxide administration in cases with a clinical history of “cor pulmonale” or as a recruitment maneuver for hypoxemia; and 5. extracorporeal membrane oxygenation (ECMO) (22. World Health Organization. Clinical management of severe acute respiratory infection when COVID-19 is suspected. 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected. [Accessed March 24th, 2020].
https://www.who.int/publications-detail/...
,4444. Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2017;195(9):1253-63. https://doi.org/10.1164/rccm.201703-0548ST.
https://doi.org/10.1164/rccm.201703-0548...
,4646. Gerlach H, Keh D, Semmerow A, Busch T, Lewandowski K, Pappert DM, et al. Dose-response characteristics during long-term inhalation of nitric oxide in patients with severe acute respiratory distress syndrome: a prospective, randomized, controlled study. Am J Respir Crit Care Med. 2003;167(7):1008-15. https://doi.org/10.1164/rccm.2108121.
https://doi.org/10.1164/rccm.2108121...
,4747. Pham T, Combes A, Rozé H, Chevret S, Mercat A, Roch A, et al. Extracorporeal membrane oxygenation for pandemic influenza A(H1N1)-induced acute respiratory distress syndrome: a cohort study and propensity-matched analysis. Am J Respir Crit Care Med. 2013;187(3):276-85. https://doi.org/10.1164/rccm.201205-0815OC.
https://doi.org/10.1164/rccm.201205-0815...
).
PRONE POSITION
Prone ventilation for 12 to 16 hours a day is recommended in adult patients with severe ARDS (PaO2/FiO2 <150), (22. World Health Organization. Clinical management of severe acute respiratory infection when COVID-19 is suspected. 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected. [Accessed March 24th, 2020].
https://www.who.int/publications-detail/...
,4444. Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2017;195(9):1253-63. https://doi.org/10.1164/rccm.201703-0548ST.
https://doi.org/10.1164/rccm.201703-0548...
). It is strongly recommended for adult patients with severe ARDS but requires sufficient human resources and knowledge to be performed safely. Protocols and videos are available in the study by Guérin et al., 2013. A satisfactory response is defined as a patient achieving an increase of 10 mmHg in PaO2 or an increase of 20 mmHg in the PaO2/FiO2 ratio. Prone positioning should be repeated when a PaO2/FiO2 ratio <150 mmHg is observed after 6 hours in the supine position. PaO2/FiO2 reductions of 20% in the supine position should be considered criteria for interrupting the prone position after two consecutive attempts at pronation or hemodynamic instability (4848. Guérin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368(23):2159-68. https://doi.org/10.1056/NEJMoa1214103.
https://doi.org/10.1056/NEJMoa1214103...
,4949. Oliveira VM, Piekala DM, Deponti GN, Batista DCR, Minossi SD, Chisté M, et al. Safe prone checklist: construction and implementation of a tool for performing the prone maneuver. Rev Bras Ter Intensiva. 2017;29(2):131-41. https://doi.org/10.5935/0103-507X.20170023.
https://doi.org/10.5935/0103-507X.201700...
).
CUFF PRESSURE
Invasive mechanical ventilation is a risk factor for aerosols (5050. Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7(4):e35797. https://doi.org/10.1371/journal.pone.0035797
https://doi.org/10.1371/journal.pone.003...
). Therefore, it is important to maintain a cuff pressure between 20 and 30 cmH2O or 25 and 35 mmHg, with sufficient pressure to prevent leakage and aerosol spread (5151. Sultan P, Carvalho B, Rose BO, Cregg R. Endotracheal tube cuff pressure monitoring: a review of the evidence. J Perioper Pract. 2011;21(11):379-86. https://doi.org/10.1177/175045891102101103.
https://doi.org/10.1177/1750458911021011...
). We suggest cuff measurement either at every shift or at least daily (5151. Sultan P, Carvalho B, Rose BO, Cregg R. Endotracheal tube cuff pressure monitoring: a review of the evidence. J Perioper Pract. 2011;21(11):379-86. https://doi.org/10.1177/175045891102101103.
https://doi.org/10.1177/1750458911021011...
).
TUBE AND NASOTRACHEAL SUCTION
Suction of the artificial airway because of ventilator disconnection must be avoided so that there is no loss of pressure in the respiratory system, atelectasis, or spread of aerosols in the room. The use of a closed suction system in all cases of intubation and invasive mechanical ventilation is recommended (22. World Health Organization. Clinical management of severe acute respiratory infection when COVID-19 is suspected. 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected. [Accessed March 24th, 2020].
https://www.who.int/publications-detail/...
,5050. Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7(4):e35797. https://doi.org/10.1371/journal.pone.0035797
https://doi.org/10.1371/journal.pone.003...
). In situations requiring open suction, we suggest the use of the “stand by” mode of the mechanical ventilator to minimize the spread of aerosols. Nasotracheal suction should be performed with careful evaluation by the physiotherapist because of the generation of aerosols. To perform these procedures, the use of proper PPE is recommended. Whenever possible, this procedure should be performed in a negative-pressure room.
HUMIDIFIERS FOR VENTILATED PATIENTS
Heat and moisture exchangers or heated humidifiers are more effective in preventing complications such as airway blockages and pneumonia in adults who receive invasive mechanical ventilation (5252. Gillies D, Todd DA, Foster JP, Batuwitage BT. Heat and moisture exchangers versus heated humidifiers for mechanically ventilated adults and children. Cochrane Database Syst Rev. 2017;9(9):CD004711. https://doi.org/10.1002/14651858.CD004711.pub3
https://doi.org/10.1002/14651858.CD00471...
). Therefore, patients with COVID-19 should use devices that humidify and filter their inhaled and exhaled air, respectively. Thus, HMEF is more suitable for the humidification of exchanged air as it also has filtering capacity for viruses and bacteria, thus reducing air contamination. Additional protection can be provided by placing a HEPA filter on the exhalation valve of the mechanical ventilator. The use of heated humidifiers is discouraged in these patients (4343. Respiratory Care Committee of Chinese Thoracic Society. [Expert consensus on preventing nosocomial transmission during respiratory care for critically ill patients infected by 2019 novel coronavirus pneumonia]. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43(4):288-96. https://doi.org/10.3760/cma.j.cn112147-20200304-00239.
https://doi.org/10.3760/cma.j.cn112147-2...
).
WEANING FROM MECHANICAL VENTILATION AND EXTUBATION
All patients must be evaluated daily regarding the eligibility criteria for the spontaneous breathing test, considering adequate oxygenation: PaO2/FiO2>200 with PEEP ≤5-7 cmH2O, hemodynamic stability with low and stabilized doses or without vasopressor drug infusion, an adequate level of consciousness (easily awake or wakened), and adequate cough and secretion management with the presence of a cough reflex during closed aspiration (5353. Boles JM, Bion J, Connors A, Herridge M, Marsh B, Melot C, et al. Weaning from mechanical ventilation. Eur Respir J. 2007;29(5):1033-56. https://doi.org/10.1183/09031936.00010206.
https://doi.org/10.1183/09031936.0001020...
,5454. Tobin MJ. Remembrance of weaning past: the seminal papers. Intensive Care Med. 2006;32(10):1485-93. https://doi.org/10.1007/s00134-006-0338-8.
https://doi.org/10.1007/s00134-006-0338-...
).
To wean patients with COVID-19 from mechanical invasive ventilation, we recommend the use of the pressure support ventilation (PSV) mode for spontaneous breathing tests. The use of the T-tube method should be avoided as it can increase aerosolization (4343. Respiratory Care Committee of Chinese Thoracic Society. [Expert consensus on preventing nosocomial transmission during respiratory care for critically ill patients infected by 2019 novel coronavirus pneumonia]. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43(4):288-96. https://doi.org/10.3760/cma.j.cn112147-20200304-00239.
https://doi.org/10.3760/cma.j.cn112147-2...
). Table 1 shows the parameters suggested for the spontaneous breathing test in PSV (A), success criteria (B), and failure criteria (C) (5555. Vallverdú I, Calaf N, Subirana M, Net A, Benito S, Mancebo J. Clinical characteristics, respiratory functional parameters, and outcome of a two-hour T-piece trial in patients weaning from mechanical ventilation. Am J Respir Crit Care Med. 1998;158(6):1855-62. https://doi.org/10.1164/ajrccm.158.6.9712135.
https://doi.org/10.1164/ajrccm.158.6.971...
56. Heunks LM, van der Hoeven JG. Clinical review: the ABC of weaning failure--a structured approach. Crit Care. 2010;14(6):245. https://doi.org/10.1186/cc9296
https://doi.org/10.1186/cc9296...
57. Thille AW, Richard JC, Brochard L. The decision to extubate in the intensive care unit. Am J Respir Crit Care Med. 2013;187(12):1294-302. https://doi.org/10.1164/rccm.201208-1523CI.
https://doi.org/10.1164/rccm.201208-1523...
58. Perren A, Brochard L. Managing the apparent and hidden difficulties of weaning from mechanical ventilation. Intensive Care Med. 2013;39(11):1885-95. https://doi.org/10.1007/s00134-013-3014-9.
https://doi.org/10.1007/s00134-013-3014-...
59. Schmidt GA, Girard TD, Kress JP, Morris PE, Ouellette DR, Alhazzani W, et al. Liberation From Mechanical Ventilation in Critically Ill Adults: Executive Summary of an Official American College of Chest Physicians/American Thoracic Society Clinical Practice Guideline. Chest. 2017;151(1):160-5. https://doi.org/10.1016/j.chest.2016.10.037.
https://doi.org/10.1016/j.chest.2016.10....
-6060. Sklar MC, Burns K, Rittayamai N, Lanys A, Rauseo M, Chen L, et al. Effort to Breathe with Various Spontaneous Breathing Trial Techniques. A Physiologic Meta-analysis. Am J Respir Crit Care Med. 2017;195(11):1477-85. https://doi.org/10.1164/rccm.201607-1338OC.
https://doi.org/10.1164/rccm.201607-1338...
). The cuff leak test should not be performed routinely before extubation because of the risk of aerosolization. However, its use should be considered for the clinical suspicion of upper airway edema or the presence of risk factors for post-extubation stridor (6161. Schnell D, Planquette B, Berger A, Merceron S, Mayaux J, Strasbach L, et al. Cuff Leak Test for the Diagnosis of Post-Extubation Stridor: A Multicenter Evaluation Study. J Intensive Care Med. 2019;34(5):391-6. https://doi.org/10.1177/0885066617700095.
https://doi.org/10.1177/0885066617700095...
).
Patients who pass the spontaneous breathing test should preferably be extubated in a negative-pressure room or in respiratory isolation. Physiotherapists and other health professionals present in the environment during extubation must follow PPE aerosol isolation precautions. During the procedure, extra care must be taken during extubation, including keeping the HMEF and closed endotracheal suction (e. g. Trach-Care®) connected to the endotracheal tube when deflating the cuff. The endotracheal tube should be removed as gently as possible to avoid vigorous manipulation and coughing. If it is necessary to stimulate the patient's cough, the patient should be instructed to adopt cough etiquette. The tube must be discarded in the infectious waste collector. In the ICU, the availability of a professional with experience in intubation is always recommended during the extubation of patients diagnosed with COVID-19, in case rapid reintubation is necessary. The rate of reintubation of these patients should be as low as possible; therefore, we recommend that the decision regarding the patient's extubation be rigorously discussed within the multidisciplinary team (6262. Fernandez MM, González-Castro A, Magret M, Bouza MT, Ibaãez M, García C, et al. Reconnection to mechanical ventilation for 1 h after a successful spontaneous breathing trial reduces reintubation in critically ill patients: a multicenter randomized controlled trial. Intensive Care Med. 2017;43(11):1660-7. https://doi.org/10.1007/s00134-017-4911-0.
https://doi.org/10.1007/s00134-017-4911-...
,6363. Cook TM, El-Boghdadly K, McGuire B, McNarry AF, Patel A, Higgs A. Consensus guidelines for managing the airway in patients with COVID-19: Guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists. Anaesthesia. 2020;75(6):785-99. https://doi.org/10.1111/anae.15054.
https://doi.org/10.1111/anae.15054...
).
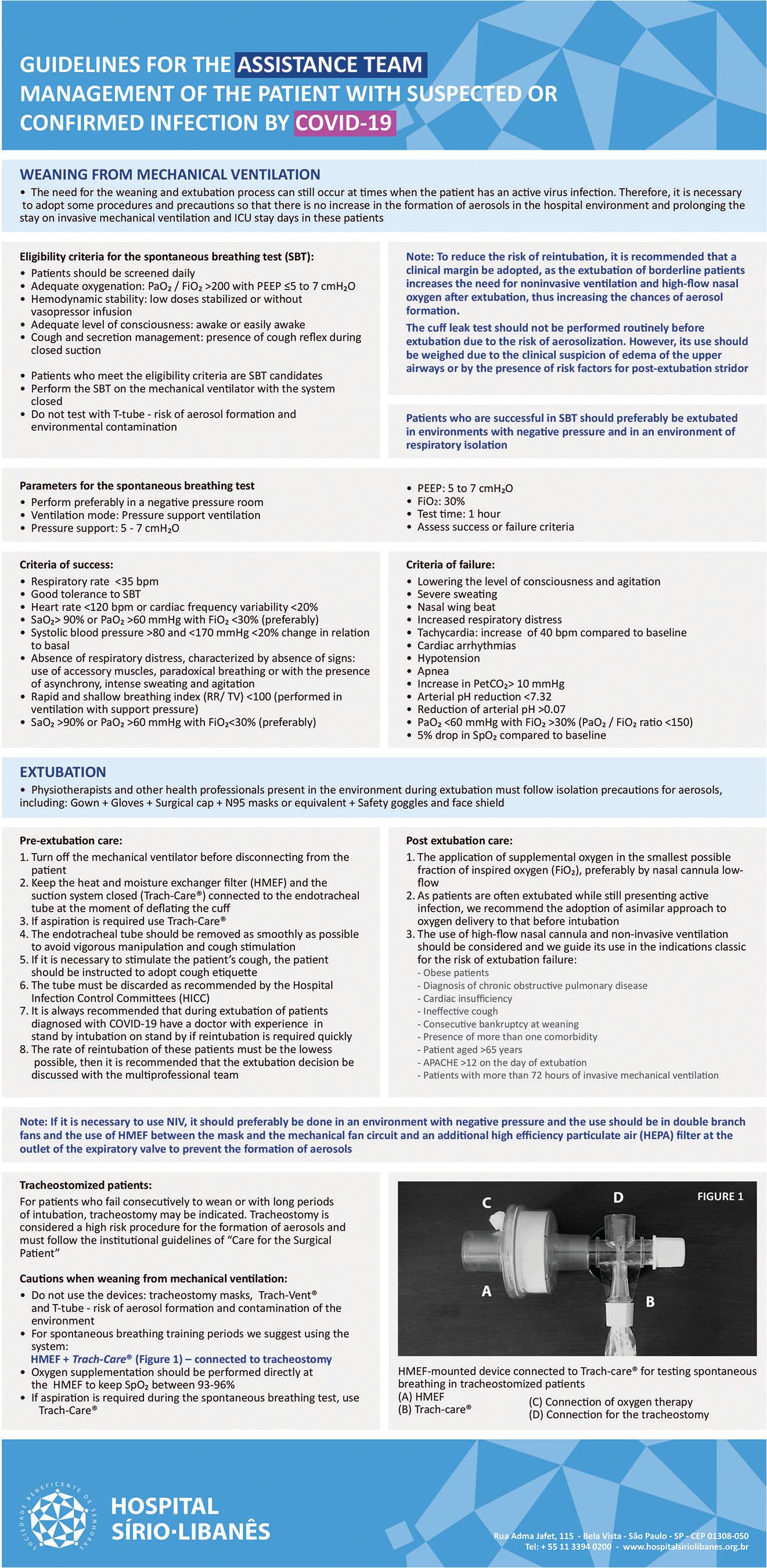
Tracheostomy may be indicated for patients who consecutively fail to wean or with long periods of intubation. Tracheostomy is considered a high-risk procedure for the formation of aerosols. Weaning patients using tracheostomy masks (e.g., Trach-Vent® and T-tube) is not recommended for patients with COVID-19. Rather, for spontaneous breathing training periods, the use of HMEF connected to Trach-Care® (Figure 4), with oxygen supplementation directly in the HMEF to maintain SpO2 between 93 and 96%, is recommended. If aspiration is required during the spontaneous breathing test, the closed suction system must be used. We emphasize that the use of HMEF to wean tracheostomized patients requires constant assessment of clinical signs of discomfort or instability. Spontaneous breathing time should be progressive as patients improve breathing performance and resistance (6464. Givi B, Schiff BA, Chinn SB, Clayburgh D, Iyer NG, Jalisi S, et al. Safety Recommendations for Evaluation and Surgery of the Head and Neck During the COVID-19 Pandemic. JAMA Otolaryngol Head Neck Surg. 2020. https://doi.org/10.1001/jamaoto.2020.0780
https://doi.org/10.1001/jamaoto.2020.078...
).
Spontaneous breathing test device for tracheostomized patients: (A) heat moisture exchange filter (HMEF), (B) closed endotracheal suction (Trach-care), (C) site for connection of oxygen therapy in HMEF. (D) connection for the tracheostomy.
EQUIPMENT AND HAND HYGIENE
The cleaning of the equipment with 70% alcohol or chlorine-based substances is recommended immediately after use. Health workers should wash their hands frequently, especially after contact with infected people or their environment (22. World Health Organization. Clinical management of severe acute respiratory infection when COVID-19 is suspected. 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected. [Accessed March 24th, 2020].
https://www.who.int/publications-detail/...
).
CONCLUSION
COVID-19 is a new disease that presents challenges to inpatient care. These recommendations can serve as clinical practice guidelines for physiotherapists. Physiotherapy plays a fundamental role throughout patient hospitalization. However, the hospital physiotherapy team must be well-oriented regarding specific care to both reduce infection risk and provide the best patient care. The Appendix section presents cards from our institution, Hospital Sírio-Libanês, in English and Portuguese languages for the respiratory management of patients with suspected or confirmed COVID-19 infection.
APPENDIX
ACKNOWLEDGMENTS
The authors acknowledge the financial support of the Brazilian Scientific Agency Fundação de Amparo è Pesquisa do Estado de São Paulo (FAPESP, number 18/16832-9) and Hospital Sírio-Libanês.
REFERENCES
-
1Weston S, Frieman MB. COVID-19: Knowns, Unknowns, and Questions. mSphere. 2020;5(2):e00203-20. https://doi.org/10.1128/mSphere.00203-20
» https://doi.org/doi:10.1128/mSphere.00203-20 -
2World Health Organization. Clinical management of severe acute respiratory infection when COVID-19 is suspected. 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected [Accessed March 24th, 2020].
» https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected -
3Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020;382(18):1708-20. https://doi.org/10.1056/NEJMoa2002032
» https://doi.org/10.1056/NEJMoa2002032 -
4Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, et al. Clinical Course and Outcomes of Critically Ill Patients With SARS-CoV-2 Pneumonia in Wuhan, China: A Single-Centered, Retrospective, Observational Study. Lancet Respir Med. 2020;8(5):475-81. https://doi.org/10.1016/S2213-2600(20)30079-5
» https://doi.org/10.1016/S2213-2600(20)30079-5 -
5Grasselli G, Presenti A, Cecconi M. Critical Care Utilization for the COVID-19 Outbreak in Lombardy, Italy: Early Experience and Forecast During an Emergency Response. JAMA. 2020. https://doi.org/10.1001/jama.2020.4031
» https://doi.org/10.1001/jama.2020.4031 -
6Jerre G, Beraldo MA, Silva Tde J, Gastaldi A, Kondo C, Leme F, et al. [Physiotherapy on the Mechanically Ventilated Patients]. J Bras Pneumol. 2007;33(Suppl 2):S142-50. https://doi.org/10.1590/S1806-37132007000800010
» https://doi.org/10.1590/S1806-37132007000800010 -
7Stiller K. Physiotherapy in intensive care: an updated systematic review. Chest. 2013;144(3):825-47. https://doi.org/10.1378/chest.12-2930
» https://doi.org/10.1378/chest.12-2930 -
8Spruit MA. Pulmonary rehabilitation. Eur Respir Rev. 2014;23(131):55-63. https://doi.org/10.1183/09059180.00008013
» https://doi.org/10.1183/09059180.00008013 -
9Ambrosino N, Makhabah DN. Comprehensive physiotherapy management in ARDS. Minerva Anestesiol. 2013;79(5):554-63.
-
10Goãi-Viguria R, Yoldi-Arzoz E, Casajús-Sola L, Aquerreta-Larraya T, Fernández-Sangil P, Guzmán-Unamuno E, et al. Respiratory Physiotherapy in Intensive Care Unit: Bibliographic Review. Enferm Intensiva. 2018;29(4):168-81. https://doi.org/10.1016/j.enfi.2018.03.003
» https://doi.org/10.1016/j.enfi.2018.03.003 -
11Lim WS, Anderson SR, Read RC. SARS Guidelines Committee of the British Thoracic Society; British Infection Society; Health Protection Agency. Hospital management of adults with severe acute respiratory syndrome (SARS) if SARS re-emerges—updated 10 February 2004. J Infect. 2004;49(1):1-7. https://doi.org/10.1016/j.jinf.2004.04.001
» https://doi.org/10.1016/j.jinf.2004.04.001 -
12Livingston E, Desai A, Berkwits M. Sourcing Personal Protective Equipment During the COVID-19 Pandemic. JAMA. 2020. https://doi.org/10.1001/jama.2020.5317
» https://doi.org/10.1001/jama.2020.5317 -
13Carlson AL, Budd AP, Perl TM. Control of Influenza in Healthcare Settings: Early Lessons From the 2009 Pandemic. Curr Opin Infect Dis. 2010;23(4):293-9. https://doi.org/10.1097/QCO.0b013e32833bb804
» https://doi.org/10.1097/QCO.0b013e32833bb804 -
14Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol Generating Procedures and Risk of Transmission of Acute Respiratory Infections to Healthcare Workers: A Systematic Review. PLoS One. 2012;7(4):e35797. https://doi.org/10.1371/journal.pone.0035797
» https://doi.org/10.1371/journal.pone.0035797 -
15van Doremalen N, Bushmaker T, Morris DH, Holbrook MG, Gamble A, Williamson BN, et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N Engl J Med. 2020;382(16):1564-7. https://doi.org/10.1056/NEJMc2004973
» https://doi.org/10.1056/NEJMc2004973 -
16Cheung JC, Ho LT, Cheng JV, Cham EYK, Lam KN. Staff safety during emergency airway management for COVID-19 in Hong Kong. Lancet Respir Med. 2020;8(4):e19. https://doi.org/10.1016/S2213-2600(20)30084-9
» https://doi.org/10.1016/S2213-2600(20)30084-9 -
17World Health Organization. Rational use of personal protective equipment (PPE) for coronavirus disease (COVID-19): interim guidance, 19 March 2020. Available from: https://apps.who.int/iris/handle/10665/331498 [Accessed March 20th, 2020].
» https://apps.who.int/iris/handle/10665/331498 -
18Milton DK, Fabian MP, Cowling BJ, Grantham ML, McDevitt JJ. Influenza Virus Aerosols in Human Exhaled Breath: Particle Size, Culturability, and Effect of Surgical Masks. PLoS Pathog. 2013;9(3):e1003205. https://doi.org/10.1371/journal.ppat.1003205
» https://doi.org/10.1371/journal.ppat.1003205 -
19Ferioli M, Cisternino C, Leo V, Pisani L, Palange P, Nava S. Protecting healthcare workers from SARS-CoV-2 infection: practical indications. Eur Respir Rev. 2020;29(155):200068. https://doi.org/10.1183/16000617.0068-2020
» https://doi.org/10.1183/16000617.0068-2020 -
20Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical Features of Patients Infected With 2019 Novel Coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-506. https://doi.org/10.1016/S0140-6736(20)30183-5
» https://doi.org/10.1016/S0140-6736(20)30183-5 -
21Cabillic M, Gouilly P, Reychler G. [Manual Airway Clearance Techniques in Adults and Adolescents: What Level of Evidence?]. Rev Mal Respir. 2018;35(5):495-520. https://doi.org/10.1016/j.rmr.2015.12.004
» https://doi.org/10.1016/j.rmr.2015.12.004 -
22Chinese Association of Rehabilitation Medicine; Respiratory Rehabilitation Committee of Chinese Association of Rehabilitation Medicine; Cardiopulmonary Rehabilitation Group of Chinese Society of Physical Medicine and Rehabilitation. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43(4):308-14. https://doi.org/10.3760/cma.j.cn112147-20200228-00206
» https://doi.org/10.3760/cma.j.cn112147-20200228-00206 -
23Alhazzani W, Møller MH, Arabi YM, Loeb M, Gong MN, Fan E, et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Crit Care Med. 2020;48(6):e440-e469. https://doi.org/10.1097/CCM.0000000000004363
» https://doi.org/10.1097/CCM.0000000000004363 -
24Cheng HY, Jian SW, Liu DP, Ng TC, Huang WT, Lin HH, et al. Contact Tracing Assessment of COVID-19 Transmission Dynamics in Taiwan and Risk at Different Exposure Periods Before and After Symptom Onset. JAMA Intern Med. 2020. https://doi.org/10.1001/jamainternmed.2020.2020
» https://doi.org/10.1001/jamainternmed.2020.2020 -
25Hartley P, Costello P, Fenner R, Gibbins N, Quinn É, Kuhn I, et al. Change in skeletal muscle associated with unplanned hospital admissions in adult patients: A systematic review and meta-analysis. PLoS One. 2019;14(1):e0210186. https://doi.org/10.1371/journal.pone.0210186
» https://doi.org/10.1371/journal.pone.0210186 -
26Schweickert WD, Pohlman MC, Pohlman AS, Nigos C, Pawlik AJ, Esbrook CL, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet. 2009;373(9678):1874-82. https://doi.org/10.1016/S0140-6736(09)60658-9
» https://doi.org/10.1016/S0140-6736(09)60658-9 -
27Aquim EE, Bernardo WM, Buzzini RF, Azeredo NSG, Cunha LSD, Damasceno MCP, et al. Brazilian Guidelines for Early Mobilization in Intensive Care Unit. Rev Bras Ter Intensiva. 2019;31(4):434-43. https://doi.org/10.5935/0103-507X.20190084
» https://doi.org/10.5935/0103-507X.20190084 -
28Hodgson CL, Berney S, Harrold M, Saxena M, Bellomo R. Clinical review: early patient mobilization in the ICU. Crit Care. 2013;17(1):207. https://doi.org/10.1186/cc11820
» https://doi.org/10.1186/cc11820 -
29Hashem MD, Nelliot A, Needham DM. Early Mobilization and Rehabilitation in the ICU: Moving Back to the Future. Respir Care. 2016;61(7):971-9. https://doi.org/10.4187/respcare.04741
» https://doi.org/10.4187/respcare.04741 -
30Jang MH, Shin MJ, Shin YB. Pulmonary and Physical Rehabilitation in Critically Ill Patients. Acute Crit Care. 2019;34(1):1-13. https://doi.org/10.4266/acc.2019.00444
» https://doi.org/10.4266/acc.2019.00444 -
31Murakami FM, Yamaguti WP, Onoue MA, Mendes JM, Pedrosa RS, Maida AL, et al. Functional evolution of critically ill patients undergoing an early rehabilitation protocol. Rev Bras Ter Intensiva. 2015;27(2):161-9. https://doi.org/10.5935/0103-507X.20150028
» https://doi.org/10.5935/0103-507X.20150028 -
32Wu Z, McGoogan JM. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA. 2020. https://doi.org/10.1001/jama.2020.2648
» https://doi.org/10.1001/jama.2020.2648 -
33Hui DS, Chow BK, Chu L, Ng SS, Lai ST, Gin T, et al. Exhaled Air Dispersion and Removal Is Influenced by Isolation Room Size and Ventilation Settings During Oxygen Delivery via Nasal Cannula. Respirology. 2011;16(6):1005-13. https://doi.org/10.1111/j.1440-1843.2011.01995.x
» https://doi.org/10.1111/j.1440-1843.2011.01995.x -
34Wen Z, Wang W, Zhang H, Wu C, Ding J, Shen M. Is Humidified Better Than Non-Humidified Low-Flow Oxygen Therapy? A Systematic Review and Meta-Analysis. J Adv Nurs. 2017;73(11):2522-33. https://doi.org/10.1111/jan.13323
» https://doi.org/10.1111/jan.13323 -
35Simonds AK, Hanak A, Chatwin M, Morrell M, Hall A, Parker KH, et al. Evaluation of droplet dispersion during non-invasive ventilation, oxygen therapy, nebuliser treatment and chest physiotherapy in clinical practice: implications for management of pandemic influenza and other airborne infections. Health Technol Assess. 2010;14(46):131-72. https://doi.org/10.3310/hta14460-02
» https://doi.org/10.3310/hta14460-02 -
36Frat JP, Thille AW, Mercat A, Girault C, Ragot S, Perbet S, et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med. 2015;372(23):2185-96. https://doi.org/10.1056/NEJMoa1503326
» https://doi.org/10.1056/NEJMoa1503326 -
37Ni YN, Luo J, Yu H, Liu D, Liang BM, Liang ZA. The Effect of High-Flow Nasal Cannula in Reducing the Mortality and the Rate of Endotracheal Intubation When Used Before Mechanical Ventilation Compared With Conventional Oxygen Therapy and Noninvasive Positive Pressure Ventilation. A Systematic Review and Meta-Analysis. Am J Emerg Med. 2018;36(2):226-33. https://doi.org/10.1016/j.ajem.2017.07.083
» https://doi.org/10.1016/j.ajem.2017.07.083 -
38Ou X, Hua Y, Liu J, Gong C, Zhao W. Effect of high-flow nasal cannula oxygen therapy in adults with acute hypoxemic respiratory failure: a meta-analysis of randomized controlled trials. CMAJ. 2017;189(7):E260-E267. https://doi.org/10.1503/cmaj.160570
» https://doi.org/10.1503/cmaj.160570 -
39Poston JT, Patel BK, Davis AM. Management of Critically Ill Adults With COVID-19. JAMA. 2020. https://doi.org/10.1001/jama.2020.4914
» https://doi.org/10.1001/jama.2020.4914 -
40Hui DS, Chow BK, Lo T, Tsang OTY, Ko FW, Ng SS, et al. Exhaled air dispersion during high-flow nasal cannula therapy versus CPAP via different masks. Eur Respir J. 2019;53(4):1802339. https://doi.org/10.1183/13993003.02339-2018
» https://doi.org/10.1183/13993003.02339-2018 -
41Orser BA. Recommendations for Endotracheal Intubation of COVID-19 Patients. Anesth Analg. 2020;130(5):1109-10. https://doi.org/10.1213/ANE.0000000000004803
» https://doi.org/10.1213/ANE.0000000000004803 -
42Sorbello M, El-Boghdadly K, Di Giacinto I, Cataldo R, Esposito C, Falcetta S, et al. The Italian coronavirus disease 2019 outbreak: recommendations from clinical practice. Anaesthesia. 2020;75(6):724-32. https://doi.org/10.1111/anae.15049
» https://doi.org/10.1111/anae.15049 -
43Respiratory Care Committee of Chinese Thoracic Society. [Expert consensus on preventing nosocomial transmission during respiratory care for critically ill patients infected by 2019 novel coronavirus pneumonia]. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43(4):288-96. https://doi.org/10.3760/cma.j.cn112147-20200304-00239
» https://doi.org/10.3760/cma.j.cn112147-20200304-00239 -
44Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2017;195(9):1253-63. https://doi.org/10.1164/rccm.201703-0548ST
» https://doi.org/10.1164/rccm.201703-0548ST -
45NHLBI ARDS Network Tools [website]. Available from: http://www.ardsnet.org/tools.shtml [Accessed March 18th, 2020]
» http://www.ardsnet.org/tools.shtml -
46Gerlach H, Keh D, Semmerow A, Busch T, Lewandowski K, Pappert DM, et al. Dose-response characteristics during long-term inhalation of nitric oxide in patients with severe acute respiratory distress syndrome: a prospective, randomized, controlled study. Am J Respir Crit Care Med. 2003;167(7):1008-15. https://doi.org/10.1164/rccm.2108121
» https://doi.org/10.1164/rccm.2108121 -
47Pham T, Combes A, Rozé H, Chevret S, Mercat A, Roch A, et al. Extracorporeal membrane oxygenation for pandemic influenza A(H1N1)-induced acute respiratory distress syndrome: a cohort study and propensity-matched analysis. Am J Respir Crit Care Med. 2013;187(3):276-85. https://doi.org/10.1164/rccm.201205-0815OC
» https://doi.org/10.1164/rccm.201205-0815OC -
48Guérin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368(23):2159-68. https://doi.org/10.1056/NEJMoa1214103
» https://doi.org/10.1056/NEJMoa1214103 -
49Oliveira VM, Piekala DM, Deponti GN, Batista DCR, Minossi SD, Chisté M, et al. Safe prone checklist: construction and implementation of a tool for performing the prone maneuver. Rev Bras Ter Intensiva. 2017;29(2):131-41. https://doi.org/10.5935/0103-507X.20170023
» https://doi.org/10.5935/0103-507X.20170023 -
50Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7(4):e35797. https://doi.org/10.1371/journal.pone.0035797
» https://doi.org/10.1371/journal.pone.0035797 -
51Sultan P, Carvalho B, Rose BO, Cregg R. Endotracheal tube cuff pressure monitoring: a review of the evidence. J Perioper Pract. 2011;21(11):379-86. https://doi.org/10.1177/175045891102101103
» https://doi.org/10.1177/175045891102101103 -
52Gillies D, Todd DA, Foster JP, Batuwitage BT. Heat and moisture exchangers versus heated humidifiers for mechanically ventilated adults and children. Cochrane Database Syst Rev. 2017;9(9):CD004711. https://doi.org/10.1002/14651858.CD004711.pub3
» https://doi.org/10.1002/14651858.CD004711.pub3 -
53Boles JM, Bion J, Connors A, Herridge M, Marsh B, Melot C, et al. Weaning from mechanical ventilation. Eur Respir J. 2007;29(5):1033-56. https://doi.org/10.1183/09031936.00010206
» https://doi.org/10.1183/09031936.00010206 -
54Tobin MJ. Remembrance of weaning past: the seminal papers. Intensive Care Med. 2006;32(10):1485-93. https://doi.org/10.1007/s00134-006-0338-8
» https://doi.org/10.1007/s00134-006-0338-8 -
55Vallverdú I, Calaf N, Subirana M, Net A, Benito S, Mancebo J. Clinical characteristics, respiratory functional parameters, and outcome of a two-hour T-piece trial in patients weaning from mechanical ventilation. Am J Respir Crit Care Med. 1998;158(6):1855-62. https://doi.org/10.1164/ajrccm.158.6.9712135
» https://doi.org/10.1164/ajrccm.158.6.9712135 -
56Heunks LM, van der Hoeven JG. Clinical review: the ABC of weaning failure--a structured approach. Crit Care. 2010;14(6):245. https://doi.org/10.1186/cc9296
» https://doi.org/10.1186/cc9296 -
57Thille AW, Richard JC, Brochard L. The decision to extubate in the intensive care unit. Am J Respir Crit Care Med. 2013;187(12):1294-302. https://doi.org/10.1164/rccm.201208-1523CI
» https://doi.org/10.1164/rccm.201208-1523CI -
58Perren A, Brochard L. Managing the apparent and hidden difficulties of weaning from mechanical ventilation. Intensive Care Med. 2013;39(11):1885-95. https://doi.org/10.1007/s00134-013-3014-9
» https://doi.org/10.1007/s00134-013-3014-9 -
59Schmidt GA, Girard TD, Kress JP, Morris PE, Ouellette DR, Alhazzani W, et al. Liberation From Mechanical Ventilation in Critically Ill Adults: Executive Summary of an Official American College of Chest Physicians/American Thoracic Society Clinical Practice Guideline. Chest. 2017;151(1):160-5. https://doi.org/10.1016/j.chest.2016.10.037
» https://doi.org/10.1016/j.chest.2016.10.037 -
60Sklar MC, Burns K, Rittayamai N, Lanys A, Rauseo M, Chen L, et al. Effort to Breathe with Various Spontaneous Breathing Trial Techniques. A Physiologic Meta-analysis. Am J Respir Crit Care Med. 2017;195(11):1477-85. https://doi.org/10.1164/rccm.201607-1338OC
» https://doi.org/10.1164/rccm.201607-1338OC -
61Schnell D, Planquette B, Berger A, Merceron S, Mayaux J, Strasbach L, et al. Cuff Leak Test for the Diagnosis of Post-Extubation Stridor: A Multicenter Evaluation Study. J Intensive Care Med. 2019;34(5):391-6. https://doi.org/10.1177/0885066617700095
» https://doi.org/10.1177/0885066617700095 -
62Fernandez MM, González-Castro A, Magret M, Bouza MT, Ibaãez M, García C, et al. Reconnection to mechanical ventilation for 1 h after a successful spontaneous breathing trial reduces reintubation in critically ill patients: a multicenter randomized controlled trial. Intensive Care Med. 2017;43(11):1660-7. https://doi.org/10.1007/s00134-017-4911-0
» https://doi.org/10.1007/s00134-017-4911-0 -
63Cook TM, El-Boghdadly K, McGuire B, McNarry AF, Patel A, Higgs A. Consensus guidelines for managing the airway in patients with COVID-19: Guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists. Anaesthesia. 2020;75(6):785-99. https://doi.org/10.1111/anae.15054
» https://doi.org/10.1111/anae.15054 -
64Givi B, Schiff BA, Chinn SB, Clayburgh D, Iyer NG, Jalisi S, et al. Safety Recommendations for Evaluation and Surgery of the Head and Neck During the COVID-19 Pandemic. JAMA Otolaryngol Head Neck Surg. 2020. https://doi.org/10.1001/jamaoto.2020.0780
» https://doi.org/10.1001/jamaoto.2020.0780
Publication Dates
-
Publication in this collection
22 June 2020 -
Date of issue
2020
History
-
Received
11 May 2020 -
Accepted
15 May 2020