LETTER TO THE EDITOR
INTRODUCTION
Endometriosis is the presence of functioning endometrial tissue outside the uterine cavity2,3,6,7,8,10,12,13. It is hormone dependent disease that affects women in reproductive age1,3,4,6,7,9,10. The most common sites are the intra-pelvic such as ovaries, uterin tubes, fornix, uterus, sacral ligament, pelvic peritoneum2,6,7,8,12,13. It can also occurs in distant organs like the lungs, pleura, liver, gastrointestinal tract, central nervous system, skin, striated muscle4,6,8. In the digestive tract the most affected sites in descending order are the rectum, sigmoid colon, ileocecal appendix, terminal ileum and cecum1,4,6,7,10,11,12,13. The diagnosis of endometriosis can be difficult because of its nonspecific symptoms. When located in the large intestine the distinction with malignancies, inflammatory and stenosis should always be suspected6,8,9,10,11,13.
The treatment of intestinal endometriosis may be surgical or hormonal, depending on age, the desire to maintain fertility, the severity and complications of the disease4,6,7,11.
CASE REPORT
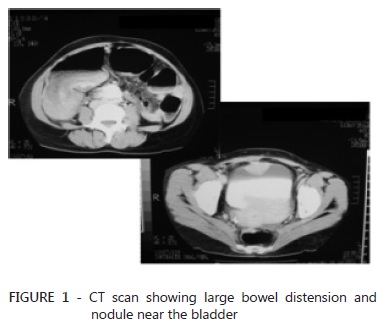
Woman of 40 years, white, reported that two months ago presented abdominal distension with a stop elimination of gas and feces. Two days ago had diffuse abdominal cramping associated with no elimination of gas and feces, loss appetite and vomiting. Reported use of oral contraceptives for eight consecutive years, suspended with the pregnancy. In the last period, nine days before the onset of symptoms noticed change in consistency of stools that were pasty. Physical examination revealed distended abdomen with pale, painful to deep palpation especially in lower abdomen, without signs of peritoneal irritation and abdominal auscultation increased peristalsis. Rectal examination showed the absence of stools, rectal bleeding and tumors. Was initially treated with fasting, nasogastric and bladder tube, fluid replacement, analgesics and observation of vital signs. Radiology showed pneumoperitoneum no colonic distension, air-fluid levels and absence of gas in the rectum. Abdominal and pelvic CT scan showed an expansive lesion in the sigmoid with obstruction of the intestinal segment, gaseous distension of the cecum, without distention of the ileal loops. Also had a nodular lesion involving the anterior wall of the bladder measuring four centimeters (Figure 1). The uterus was enlarged with nodular lesions suggestive of leiomyoma and cystic formation.
Median laparotomy was done and found dilatation of the entire large intestine and a stenotic lesion in the sigmoid colon, with a serous bleeding. The small bowel was not dilated. A four inches nodular lesion in the bladder was noticed with myomatous uterus and left ovarian cyst. Due to the macroscopic findings suggested endometriosis a Hartmann sigmoidectomy was performed. At the opening of the specimen, a full mucosa without the presence of ulceration, thickened wall and stenotic lesion were found (Figure 2).
The patient had no complications and was discharged in 3º day postoperatively. The histopathology of endometriosis was revealed with no signs of malignancy. Subsequently she underwent a total hysterectomy and reconstitution of the bowel with surgical staples.
DISCUSSION
Endometriosis is a disease that affects around 3% to 20% of women of childbearing age1,2,3,4,5,6,7,8,9,10,11,12,13. The mean age of patients diagnosed with endometriosis ranges from 25 to 30 years of age; is also found among adolescents with chronic pelvic pain and dyspareunia. Infertility occurs in 30% of cases7,11.
Depending on the location of the ectopic tissue, endometriosis may present itself in two forms: internal endometriosis or uterine, where the ectopic focus is on the uterine muscle, also known as adenomyosis3,6,7.
The diagnosis can be suspected from the four cardinal points: infertility, dysmenorrhea and menstrual and sexual problems3,6,7,8,13. Intestinal involvement in endometriosis occurs in 3% to 37%. The rectum and sigmoid are responsible for 73% of cases and the rectovaginal septum by 13% followed, in descending order, the ileocecal appendix, terminal ileum and cecum 1,4,6,7,10,11,12,13.
Intestinal endometriosis usually is asymptomatic. When symptomatic, the symptoms are abdominal or pelvic pain, rectal pain, diarrhea, constipation, tenesmus, rectal bleeding and symptoms of intestinal obstruction. The symptoms are generally more exuberant1,3,5,6,7,8,10,11,12,13 during the menstrual period.
The bowel disease is characterized by macroscopically limited to serosal implants. However these implants, in some cases can reach the intestinal mucosa. Repeated bleeding in endometriomas cause intense inflammatory reaction with secondary fibrosis and may lead to adhesions of the pelvic organs or even involved colorectal segment. These changes may result in intestinal obstruction associated with abdominal pain and changes in bowel habits6,10,11,13.
The acute intestinal obstruction secondary to endometriosis is a rare complication3,9. The diagnosis of intestinal form is hard to do, especially in the preoperative period, and should always be suspected in women of childbearing age who have intestinal disorders, especially when the presence of gynecologicl signs or symptoms3,5,7,8,9,12,13. In this case the patient had a clinical aspect of intestinal obstruction7,10. She had no metrorrhagia, dispaurenia or dysmenorrhea. The only aspects in the history of the patient, which could raise the hypothesis would be endometriosis, the cesarean delivery, the change in stool consistency during the menstrual period, and the fact that she didn´t became pregnant using birth control and condoms withdrawal3,6,8,11.
A pelvic ultrasound is considered essential to study the ovarian lesions6,7,11. The barium enema may help6,11,13. Colonoscopy and/or sigmoidoscopy should be performed in an attempt to visualize the characteristic macroscopic lesion and biopsy to remove fragments, but there are limitations as the majority of patients have intact mucosa3,6,7,10,11.
Several authors state that laparoscopy is the "gold standard" for the diagnosis of endometriosis, allowing to detect and assess the extent of disease3,6,7,13. Recently, laparoscopic surgery has advanced stages and proving to be feasible and effective6,12,13.
The treatment of intestinal endometriosis may be surgical or hormonal, depending on age, the desire to maintain fertility, the severity and complications of the disease4,6,7. The ovariectomy and hormone treatment are shown in oligosymptomatic patients with less extensive colorectal endometriomas6,7. The patient was evaluated by a gynecology clinic, and underwent bilateral oophorectomy and hysterectomy for myomatous uterus present at the time of reconstitution of the intestinal transit.
REFERENCES
- 1. Abrão MS, Machado MAC, Campos FG, Gama AH, Pinotti HW. Endometriose de Reto: Relato de Caso. Rev Hosp Clín Fac Med S. Paulo 1994;49(4):173-176.
- 2. Camurça MF. Endometriose Perianal e Íleo Cecal: Registro de Casos. Ceará Médico 1981;3(3):43-45.
- 3. D'Acampora AJ, Felício F, Santos JM, Froner LG, Santos CM, Grudtner JH. Obstrução Intestinal por Endometriose do Sigmóide: Apresentação de Caso. Arq Cat Med 1985;14(4): 257-261.
- 4. De Anchorena, M; Heidenreich, A; Gori, J; Hülskamp, P; Maletti, G. Bowel Endometriosis. Prensa méd.argent 1999;86(8):746-754.
- 5. Fagundes DJ, Plapler H. Estenose de Retossigmóide e Endometriose: Apresentação de Caso. Rev Col Bras Cir 1993;22(3):151-153.
- 6. Garcia A, Spadoni Neto B, Garcia VCS, Arruda P, Garcia DL. Endometriose Colônica Simulando Câncer Colorretal: Relato de Dois Casos. Rev Bras Coloproct 2006;26(3):316-320.
- 7. Guerra GMLSR, Monteiro EP, Souza HFS, Fonseca MFM, Horta SHC, Formiga GJS. Endometriose de Reto: Relato de Caso. Rev Bras Coloproct 2004;24(4):354-357.
- 8. Hilgert HC, Sudbrack C, Zimmermann AC, Cruz JV. Endometriose de Reto: Relato de Caso e Revisão de Literatura. R. Pesquisa Médica, Porto Alegre 1989;23(1):32-35.
- 9. de Paula JF, Batista CAM, Leite GF, Osugue JY, Faria JGR, Pedrosa LCAS, Umeoka G, Sathler CGH. Endometriose de Retossigmóide Como Causa de Obstrução Intestinal. Revista da Faculdade de Medicina de Valença 1998;1:40-44.
- 10. Popoutchi P, Lemos CRR, Silva JCR, Nogueira AA, Feres O, da Rocha JJR. Postmenopausal Intestinal Obstructive Endometriosis: Case Report and Review of the Literature. São Paulo Med J 2008;126(3).
- 11. Ribeiro HSAA, Ribeiro PAAG, Rodrigues FC, Donadio N, Auge APF, Aoki T . Valor do enema de bário com duplo contraste o diagnóstico da endometriose do reto e sigmóide. Rev Bras Ginecol Obstet. 2008;30(8):400-405.
- 12. Seid VE, Imperiale AR, Araújo SE Campos. Videolaparoscopia no Diagnóstico e Tratamento da Obstrução Intestinal. Rev Bras Coloproct 2007;27(2):228-234.
- 13. Souza JVS, Carmel APW, Silvany AM. Tratamento Cirúrgico da Endometriose Intestinal: Seção Livre. Rev Bras Coloproct 1996;16(4):232-234.
Endometriosis as a cause of intestinal obstruction
Publication Dates
-
Publication in this collection
24 Jan 2012 -
Date of issue
Dec 2011