Abstracts
Cochlear implants represent a significant breakthrough in the treatment of hearing loss. Evidence indicates bilateral hearing brings significant benefits to patients, particularly when binaural hearing is offered. OBJECTIVE: To describe the first case of implantation of a Digisonic SP® Binaural Neurelec device in Brazil (the third implant placed in the Americas, after Mexico and Colombia) and the chosen surgical approach. METHOD: Description of a surgical approach. RESULTS: The procedure was successfully completed. DISCUSSION: The squelch effect, binaural summation, location of the sound source, and the shadow effect of the head are listed among the reasons to explain the superiority of binaural rehabilitation. Cost of treatment must be considered in the development of public health policies. CONCLUSION: The cost of cochlear implants has been one of the main impediments to bilateral rehabilitation. The Digisonic SP® Binaural Neurelec device addresses this issue and exposes patients to less risk through a minimally invasive implantation procedure.
cochlear implantation; deafness; hearing loss, bilateral; hearing loss, sensorineural; rehabilitation of hearing impaired
O implante coclear é um grande avanço no tratamento da surdez. Há grandes evidências que a audição bilateral traz diversas vantagens ao ser humano e muito mais quando se trata de audição binaural. OBJETIVO: Este artigo tem por objetivo descrever o primeiro caso operado no Brasil, sendo o terceiro país das Américas (México e Colômbia) a realizar, com implante binaural Neurelec Digisonic SP® demonstrando a técnica cirúrgica. MÉTODO: Descrição da técnica cirúrgica. RESULTADOS: Ver técnica cirúrgica. Procedimento ocorreu sem intercorrências. DISCUSSÃO: O efeito "squelch", a somação binaural, a localização da fonte sonora e o efeito sombra da cabeça são umas das principais razões que justificam a superioridade da reabilitação binaural. O custo do tratamento deve ser levado em conta em políticas de saúde pública. CONCLUSÃO: Custo do implante coclear é um dos grandes limitadores da bilateralidade na reabilitação desse grupo de pacientes, porém, com essa tecnologia, é possível solucionar esse problema, expondo o paciente a poucos riscos, com o uso de uma técnica cirúrgica pouco invasiva.
implante coclear; perda auditiva bilateral; perda auditiva neurossensorial; reabilitação de deficientes auditivos; surdez
ORIGINAL ARTICLE
Digisonic SP® Binaural cochlear implant: the coronal tunneled approach
Guilherme Machado de CarvalhoI; Alexandre Caixeta GuimarãesII; Ivan Senis Cardoso MacedoIII; Lúcia Cristina Beltrame OnukiIV; Fabiana DanieliV; Henrique Furlan PaunaII; Fernando Laffitte FernandesVI; Jorge Rizzato PaschoalVII; Walter Adriano BianchiniVIII; Arthur Menino CastilhoIX
IMSc in Medicine (Nova University in Lisbon) (ENT, Otologist, Course of Otorhinolaryngology, Head, and Neck, UNICAMP)
IIMD (ENT Resident, Course of Otorhinolaryngology, Head, and Neck, UNICAMP)
IIIMD (ENT, Otologist, Course of Otorhinolaryngology, Head, and Neck, UNICAMP)
IVSpeech and Hearing Therapist, Course of Otorhinolaryngology, Head, and Neck, UNICAMP. (Speech and Hearing Therapist, Specialist in Cochlear Implants)
VMSc in Bioengineering, Speech and Hearing Therapist (Speech and Hearing Therapist, Specialist in Cochlear Implants, MSc in Bioengineering, EESC/USP)
VIMD (ENT Resident, Course of Otorhinolaryngology, Head, and Neck, UNICAMP)
VII Professor (MD, ENT, Course of Otorhinolaryngology, Head, and Neck, UNICAMP)
VIIIMSc (ENT, Otologist, Course of Otorhinolaryngology, Head, and Neck, UNICAMP)
IXPhD (ENT, Otologist, Course of Otorhinolaryngology, Head, and Neck, UNICAMP)
Send correspondence to Send correspondence to: Guilherme Machado de Carvalho Disciplina de Otorrinolaringologia Faculdade de Ciências Médicas - UNICAMP Cidade Universitária "Zeferino Vaz". Caixa Postal: 6111 Campinas - São Paulo. Brasil. CEP: 13081-970
ABSTRACT
Cochlear implants represent a significant breakthrough in the treatment of hearing loss. Evidence indicates bilateral hearing brings significant benefits to patients, particularly when binaural hearing is offered.
OBJECTIVE: To describe the first case of implantation of a Digisonic SP® Binaural Neurelec device in Brazil (the third implant placed in the Americas, after Mexico and Colombia) and the chosen surgical approach.
METHOD: Description of a surgical approach.
RESULTS: The procedure was successfully completed.
DISCUSSION: The squelch effect, binaural summation, location of the sound source, and the shadow effect of the head are listed among the reasons to explain the superiority of binaural rehabilitation. Cost of treatment must be considered in the development of public health policies.
CONCLUSION: The cost of cochlear implants has been one of the main impediments to bilateral rehabilitation. The Digisonic SP® Binaural Neurelec device addresses this issue and exposes patients to less risk through a minimally invasive implantation procedure.
Keywords: cochlear implantation; deafness; hearing loss, bilateral; hearing loss, sensorineural; rehabilitation of hearing impaired.
INTRODUCTION
Recent studies have considered cochlear implants (CI) for the treatment of profound deafness in adults and children. The early restoration of auditory input allowed by the placement of cochlear implants has allowed patients to improve their communication skills in varying degrees1.
According to the World Health Organization (WHO), in 2025 there will be approximately 1.2 billion people in the world aged 60 and above2. The Royal National Institute for Deaf People (RNID) estimates that over 300 million people experience hearing loss today, and that this number will grow to 900 million by 20502, thus significantly increasing the need for rehabilitation of subjects with hearing loss.
Cochlear implants represent a significant innovation in the fields of surgery3 and technology. Numerous studies have stated that the benefits of implanting cochlear devices outweigh the risks, in addition to improving the quality-of-life of implanted patients3.
Unilateral cochlear implants allow patients to recognize speech in silent conditions, but CI users frequently report difficulty recognizing speech in the presence of background noise and locating sound sources. Patients are increasingly interested in having binaural cochlear implants4, as they would be able to overcome the obstacles mentioned above.
The goal of this paper was to describe the surgical technique and the first case of a bilateral Digisonic SP® Neurelec cochlear implant case done in Brazil through a subcutaneous tunnel in a coronal access, with the help of an orotracheal tube and showing the details involved in this procedure. Today, UNICAMP already has a number of cases operated, all without any complications, and we also state that some Brazilian institutions have already performed this procedure.
Today, (2013), according to Neurelec itself, such procedure had been carried out only in some countries like France, the United Kingdom, Germany, Spain, Italy, Romania, Middle East, India, Mexico, Colombia, and now, Brazil.
METHOD
Patients had to meet the following criteria to be included in the study:
Age above 16 years (growth of the skullcap);
Post-lingual patients with developed speech;
Good lip reading skills;
At least two years of experience with hearing aids;
Series of historical pure-tone audiometry tests (severe/profound sensorineural hearing loss evidence of stable audiological indicators for at least two years);
Free-field audiometry with and without hearing aids (with little gain);
Speech recognition test (performance under 60% with 65 dB on free field);
Absent brainstem auditory evoked potential (BAEP) and otoacoustic emissions (OAE);
CT scans of the ears, mastoid, and skull;
MRI scans of the ears, mastoid, and skull with assessment and reconstruction of the inner ear canal;
Psychological evaluation.
Selected patients were informed of the tests, surgery, cochlear devices, postoperative expectations, expected complications and signed an informed consent term.
Ethical aspects
The study was approved by the institution's Ethics Committee (004/2013).
RESULTS
This section includes a description of the patient and implantation approach.
Surgical approach
The patient was positioned in dorsal decubitus, administered general anesthesia, and intubated. Preparation was performed as follows:
1. Antisepsis of the face, retroauricular area, hair and scalp with 2% chlorhexidine; fixation of facial nerve electrodes, and administration of one gram of intravenous cefazolin;
2. Bilateral retroauricular hair removal, isolation and draping of the retroauricular area and face with MicroporeTM;
3. Preparation and containment of the patient's hair with elastic bands; marking of the coronal area;
4. Application of topical anesthesia (2% xylocaine with norepinephrine; 4 mg of lidocaine/kg) in the retroauricular region and on the coronal suture;
5. Additional antisepsis with 0.5% chlorhexidine of the retroauricular area and scalp;
6. Placement of sterile draping exposing the coronal suture, retroauricular areas, and part of the face;
7. Straight retroauricular incision of approximately four centimeters; dissection in planes and production of a cross-shaped flap of periosteal muscle;
8. Removal of small fragments of fascia and temporal muscle for later obliteration of the cochleostomy;
9. Mastoidectomy, exposing the lateral semicircular canal, the short branch of the incus, the posterior wall of the outer ear canal, the tegmen tympani, and the lateral sinus; a small amount of bone powder was collected;
10. Thinning of the posterior wall of the outer ear canal; posterior tympanotomy sparing the incus buttress;
11. One-millimeter cochleostomy in the anterosuperior region in relation to the round window after the identification of the round window niche;
12. Steps 7 to 11 were repeated on the contralateral side;
13. Coronal incision of three centimeters (on the head vertex) and dissection in planes;
14. Construction of a subperiosteal tunnel to connect the coronal and retroauricular incisions with the aid of lifters, retractors and conventional forceps (bilaterally);
15. Placement of a 5 mm orotracheal tube through the tunnel described above (bilaterally) (Figure 1);
16. Careful examination of hemostasis status;
17. Fixation of the internal component of the binaural Neurelec Digisonic SP® implant with two titanium screws on the squamous portion of the temporal bone (Figure 2);
18. Insertion of a lead through the cochleostomy with the aid of a microscope, placement of the ground electrode in the region of the zygomatic arch and positioning of the contralateral lead from within the ipsilateral orotracheal tube;
19. Orotracheal tube was pulled ipsilaterally to the implant internal component through the coronal incision along with the previously positioned contralateral lead (Figure 3);
20. Positioning of the contralateral lead now in the contralateral orotracheal tube;
21. Orotracheal tube was pulled contralaterally to the implant through the contralateral retroauricular incision;
22. Insertion of the lead through the cochleostomy with the aid of a microscope; placement of a ground electrode in the region of the zygomatic arch (contralateral side);
23. Positioning of a muscle graft around the electrode in a way to seal the cochleostomy; placement of bone powder to obliterate the posterior tympanotomy (bilaterally);
24. Sutures applied with VicrylTM 3.0 to close the planes of the muscle periosteum flaps; closure of the coronal incision and subcutaneous stitches with nylon 4.0 on the plane of the skin (bilaterally);
25. Patient was cleaned and external compressive bandages were placed;
26. Electrode impedances and brainstem auditory evoked potentials (BAEPs) were measured;
27. Transorbital view x-ray images were taken to confirm the position of the intracochlear lead (Figure 4).
Note: The patient's head must be moved with utter care. This surgical approach was not developed by the authors of this paper; it is an adaptation from previously described procedures5,6.
Surgery is depicted in Figures 5 to 7.


Impedance and BAEP measurement
Impedances and BAEPs were measured for the electrodes inserted in both cochleas through a bidirectional telemetry system. Diagnostic interface Digistim SP and software Digistim for Windows SP®, version 1.9.15 were used with such purpose. Measurements were carried out during and after surgery with the patient still under general anesthesia in order to check the status of the receiver-stimulator and the electrode beams, device overall function, and effectiveness of the stimuli delivered upon the peripheral auditory neural fibers in both sides (Figures 8 and 9).
Facial Nerve Monitoring
The facial nerve was monitored bilaterally throughout the entire procedure through two electrodes placed one on each side of the face on the frontal and zygomatic areas, in addition to ground leads (placed on the chest) and STIM + (positive pole on the sternoclavicular area). A NIM- PulseTM (Nerve Integrity Monitor, Meditronic XomedTM) monitor was used.
Microscope
A CARL ZEISS GMGH S88 MicroscopeTM was used. The microscope was equipped with a camera and a digital video recording system to capture images of the implantation procedures.
Device
Cochlear implant Neurelec Digisonic SP® Binaural, developed by French company Neurelec S.A. in 2006 was used in this study.
The device is made up of one receiver-stimulator connected to two electrode beams designed to stimulate the remaining neural fibers of both cochleas in a simultaneous, synchronous fashion (Figure 10). The receiver-stimulator is physically similar to the conventional monaural Digisonic SP® implant, and allows for quick, minimally invasive implantation. Each beam has 12 leads connected to a ground electrode, adding up to 24 active stimulation channels and speeds of up to 24,000 pulses per second. A contralateral microphone is connected to a Digi® SP or Saphyr® SP conventional speech processor, to separately analyze the input signals from each ear and send them synchronously to the leads positioned in each cochlea, thus producing binaural hearing (Figure 11). A Widex CROS (Widex Corp, Denmark) microphone was used.
Case
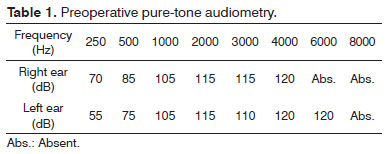
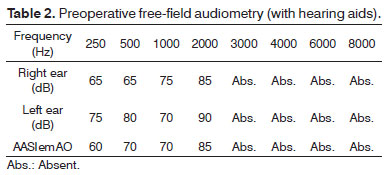
The patient was a 35-year-old woman with history of progressive hearing loss; she had been affected by severe sensorineural hearing loss for ten years. The patient had been using hearing aids in both ears for 16 years, recently with little effect.
Due to the progressive nature of her condition, she developed oral communication and acquired good lip reading skills. The patient had a family history of deafness (father, paternal uncles and aunts, siblings, grandparents).
The patient was included in the Cochlear Implantation Program of the Otology and Implantable Devices Group of the University Hospital in January of 2012.
Clinical examination, lab workup, and imaging (CT and MRI) tests failed to reveal the etiology of her condition, as all test were normal.
Her audiological assessment is described below (Tables 1 and 2).
Brainstem auditory evoked potentials, transient and product distortion otoacoustic emissions were absent for both ears.
Her scores in the Ling Six-Sound test were 0% for sound perception (each ear separately and both ears together); and 0% for name and sentence recognition (each ear separately and both ears together).
DISCUSSION
Still today, various public health care centers recommend the implantation of unilateral - instead of bilateral - cochlear devices to patients with severe to profound sensorineural hearing loss. The reasons are many, and include cost, sparing one ear for future technologies, the additional risk of a second procedure, and the lack of evidences documenting the benefits of bilateral cochlear implants7.
However, bilateral cochlear implants have been considered as significantly better than unilateral cochlear devices at improving speech recognition in noise8.
Studies also indicate that bilateral implants (two implants, one on each ear) introduce stereophonic hearing, which results in better speech recognition in noise and silence, in addition to improving sound localization9.
Improved sound localization in bilateral cochlear device users relies on the shadow effect of the head, on the squelch effect, and on binaural summation10.
The shadow effect of the head stems from the obstacle the head offers to the arrival of sound to the stimulated ear and the improvement on the signal to noise ratio. Binaural summation is the outcome of central auditory processing and represents the ability the central auditory nervous system to integrate and use the information coming from both ears. The squelch effect represents the ability of the auditory system to utilize the information sent by both ears when speech and noise are separated spatially4.
Although the literature on psychoacoustics has for long discussed the benefits of binaural hearing, only recently have studies shown improved speech intelligibility in bilateral implant users when compared to patients implanted with unilateral devices.
In ideal conditions, the benefits of bilateral implants may be far greater than reported. For example, the benefit is considerably greater in speech intelligibility in noise than in summation and squelch, and robust gains have been seen in reverberation when the source of interference is near the subject11.
Despite the clear functional benefits yielded by bilateral devices, bilateral implantation is still not popular among adult patients. The cost of a second device and the expenses associated with two surgeries decrease the likelihood of this procedure being offered by health care centers, and particularly public health services such as the Brazilian SUS.
A study on the cost-effectiveness of the cochlear implant procedure for health care services revealed that the clinical benefits provided by bilateral implants in adults were small when the expenditure is considered12.
The Digisonic SP® Binaural cochlear implant developed by Neurelec S.A. is an affordable option to bilateral implants, as only one device is used to stimulate both cochleas. This device is priced at a premium of 30% in relation to conventional unilateral implants, and offers benefits equivalent to bilateral cochlear implantation12.
The study also indicated a significant squelch effect in Digisonic SP® Binaural device users, with values above the levels observed in users of conventional bilateral implants. This aspect was described by the authors as the outcome of the right/left temporal correspondence allowed by the synchronous stimulation provided by the binaural implant13.
The Digisonic SP® Binaural device processes the sound stimuli arriving at both ears in a separate, simultaneous fashion, as also seen in bilateral cochlear implants. However, differently from bilateral devices, the binaural implant offers synchronous electric stimulation between the cochleas. In other words, the device provides stimulation in different frequency bands alternating between cochleas for each sequence of pulses, promoting correspondence between them for each sound stimulus.
Complications in cochlear device implantation occur somewhat frequently and have been a reason for concern in health care centers during the implementation of new surgical approaches. According to the European Statement on Cochlear Implant Failures and Explantations, failure can be divided into six categories: 1 - failure by impact; 2 - sealing failure; 3 - electronic failure; 4 - problems with the electrode set; 5 - others (specify); 6 - no specific reason14.
A study conducted on 550 consecutive cochlear device implantation procedures found 92 (6%) complications. Major complications accounted for 8.9% of the procedures, while minor issues were seen in 7.8% of the cases15.
Major complications included problems inserting electrodes, misplaced electrodes, damaged electrodes, compressed electrodes, insertion failure, dislocation, flap dehiscence or infection, cholesteatoma, otomastoiditis, facial palsy with sequela, CSF leak, meningitis, and incapacitating otological symptoms. The following minor complications were described: transient peripheral facial palsy, posterior meatal wall injuries, annulus and tympanic membrane injuries, perilymphatic fistula, bleeding, corda tympani nerve injuries, and hematoma15.
CONCLUSION
Bilateral cochlear implants bring several benefits to patients with severe and profound hearing loss. The Digisonic SP® Binaural device is a cost-effective alternative to bilateral implants. The surgical approach described was performed without complications, and the procedure was proven to be easy and safe.
ACKNOWLEDGEMENTS
We would like to thank the Program for the chance of carrying out projects such as this. Our gratitude also goes to the entire team involved in the rehabilitation of patients with hearing loss (employees, nurses, speech and hearing therapists, psychologists, resident physicians) and everyone else. Special thanks go to Mercedes F. Santos for her invaluable support in creating the drawings, along with the FCM AV team.
REFERENCES
1. Fortunato-Tavares T, Befi-Lopes D, Bento RF, Andrade CRF. Children with cochlear implants: communication skills and quality of life. Braz J Otorhinolaryngol. 2011;78(1):15-25.
2. Sprinzl GM, Riechelmann H. Current trends in treating hearing loss in elderly people: a review of the technology and treatment options - a mini-review. Gerontology. 2010;56:351-8. http://dx.doi. org/10.1159/000275062 PMid:20090297
3. Turchetti G, Bellelli S, Palla I, Forli F. Systematic review of the scientific literature on the economic evaluation of cochlear implants in paediatric patients. Acta Otorhinolaryngol Ital. 2011;31(5):311-8. PMid:22287822 PMCid:3262412
4. Brown KD, Balkany TJ. Benefits of bilateral cochlear implantation: a review. Curr Opin Otolaryngol Head Neck Surg. 2007;15(5):315-8. http://dx.doi.org/10.1097/MOO.0b013e3282ef3d3e PMid:17823546
5. Guevara N, Sterkers O, Bébéar JP, Meller R, Magnan J, Mosnier I, et al. Multicenter evaluation of the digisonic SP cochlear implant fixation system with titanium screws in 156 patients. Ann Otol Rhinol Laryngol. 2010;119(8):501-5. PMid:20860274
6. Truy E, Ionescu E, Ceruse P, Gallego S. The binaural digisonic cochlear implant: surgical technique. Otol Neurotol. 2002;23(5):704-9. http://dx.doi.org/10.1097/00129492-200209000-00017 PMid:12218623
7. Litovsky R, Parkinson A, Arcaroli J, Sammeth C. Simultaneous bilateral cochlear implantation in adults: a multicenter clinical study. Ear Hear. 2006;27(6):714-31. http://dx.doi.org/10.1097/01.aud.0000246816.50820.42 PMid:17086081 PMCid:2651401
8. Yoon YS, Li Y, Kang HY, Fu QJ. The relationship between binaural benefit and difference in unilateral speech recognition performance for bilateral cochlear implant users. Int J Audiol. 2011;50(8):554-65. http://dx.doi.org/10.3109/14992027.2011.580785 PMid:21696329 PMCid:3160169
9. Freyman RL, Balakrishnan U, Helfer KS. Spatial release from informational masking in speech recognition. J Acoust Soc Am. 2001;109(5 Pt 1):2112-22. http://dx.doi.org/10.1121/1.1354984 PMid:11386563
10. Hyppolito MA, Bento RF. Directions of the bilateral cochlear implant in Brazil. Braz J Otorhinolaryngol. 2012;78(1):2-3. PMid:22392231
11. Culling JF, Jelfs S, Talbert A, Grange JA, Backhouse SS. The benefit of bilateral versus unilateral cochlear implantation to speech intelligibility in noise. Ear Hear. 2012;33(6):673-82. http://dx.doi.org/10.1097/AUD.0b013e3182587356 PMid:22717687
12. Summerfield AQ, Barton GR. Getting acceptable value for money from bilateral cochlear implantation. Cochlear Implants Int. 2003;4 Suppl 1:66-7. http://dx.doi.org/10.1002/cii.112 PMid:18792183
13. Verhaert N, Lazard DS, Gnansia D, Bébéar JP, Romanet P, Meyer B, et al. Speech performance and sound localization abilities in Neurelec Digisonic® SP binaural cochlear implant users. Audiol Neurootol. 2012;17(4):256-66. http://dx.doi.org/10.1159/000338472 PMid:22584289
14. Achiques MT, Morant A, Muñoz N, Marco J, Llópez I, Latorre E, et al. Cochlear implant complications and failures. Acta Otorrinolaringol Esp. 2010;61(6):412-7. http://dx.doi.org/10.1016/j.otorri.2010.07.005 PMid:20947060
15. Brito R, Monteiro TA, Leal AF, Tsuji RK, Pinna MH, Bento RF. Surgical complications in 550 consecutive cochlear implantation. Braz J Otorhinolaryngol. 2012;78(3):80-5. http://dx.doi.org/10.1590/S180886942012000300014 PMid:22714851
Paper submitted to the BJORL-SGP (Publishing Management System - Brazilian Journal of Otorhinolaryngology) on October 22, 2012; and accepted on March 1, 2013.
Otology, Audiology and Implantable Ear Prostheses - Ear, Nose, Throat and Head & Neck Surgery Department. UNICAMP.
- 1. Fortunato-Tavares T, Befi-Lopes D, Bento RF, Andrade CRF. Children with cochlear implants: communication skills and quality of life. Braz J Otorhinolaryngol. 2011;78(1):15-25.
- 2. Sprinzl GM, Riechelmann H. Current trends in treating hearing loss in elderly people: a review of the technology and treatment options - a mini-review. Gerontology. 2010;56:351-8. http://dx.doi. org/10.1159/000275062 PMid:20090297
- 3. Turchetti G, Bellelli S, Palla I, Forli F. Systematic review of the scientific literature on the economic evaluation of cochlear implants in paediatric patients. Acta Otorhinolaryngol Ital. 2011;31(5):311-8. PMid:22287822 PMCid:3262412
- 4. Brown KD, Balkany TJ. Benefits of bilateral cochlear implantation: a review. Curr Opin Otolaryngol Head Neck Surg. 2007;15(5):315-8. http://dx.doi.org/10.1097/MOO.0b013e3282ef3d3e PMid:17823546
- 6. Truy E, Ionescu E, Ceruse P, Gallego S. The binaural digisonic cochlear implant: surgical technique. Otol Neurotol. 2002;23(5):704-9. http://dx.doi.org/10.1097/00129492-200209000-00017 PMid:12218623
- 7. Litovsky R, Parkinson A, Arcaroli J, Sammeth C. Simultaneous bilateral cochlear implantation in adults: a multicenter clinical study. Ear Hear. 2006;27(6):714-31. http://dx.doi.org/10.1097/01.aud.0000246816.50820.42 PMid:17086081 PMCid:2651401
- 8. Yoon YS, Li Y, Kang HY, Fu QJ. The relationship between binaural benefit and difference in unilateral speech recognition performance for bilateral cochlear implant users. Int J Audiol. 2011;50(8):554-65. http://dx.doi.org/10.3109/14992027.2011.580785 PMid:21696329 PMCid:3160169
- 9. Freyman RL, Balakrishnan U, Helfer KS. Spatial release from informational masking in speech recognition. J Acoust Soc Am. 2001;109(5 Pt 1):2112-22. http://dx.doi.org/10.1121/1.1354984 PMid:11386563
- 10. Hyppolito MA, Bento RF. Directions of the bilateral cochlear implant in Brazil. Braz J Otorhinolaryngol. 2012;78(1):2-3. PMid:22392231
- 11. Culling JF, Jelfs S, Talbert A, Grange JA, Backhouse SS. The benefit of bilateral versus unilateral cochlear implantation to speech intelligibility in noise. Ear Hear. 2012;33(6):673-82. http://dx.doi.org/10.1097/AUD.0b013e3182587356 PMid:22717687
- 12. Summerfield AQ, Barton GR. Getting acceptable value for money from bilateral cochlear implantation. Cochlear Implants Int. 2003;4 Suppl 1:66-7. http://dx.doi.org/10.1002/cii.112 PMid:18792183
- 14. Achiques MT, Morant A, Muñoz N, Marco J, Llópez I, Latorre E, et al. Cochlear implant complications and failures. Acta Otorrinolaringol Esp. 2010;61(6):412-7. http://dx.doi.org/10.1016/j.otorri.2010.07.005 PMid:20947060
- 15. Brito R, Monteiro TA, Leal AF, Tsuji RK, Pinna MH, Bento RF. Surgical complications in 550 consecutive cochlear implantation. Braz J Otorhinolaryngol. 2012;78(3):80-5. http://dx.doi.org/10.1590/S180886942012000300014 PMid:22714851
Send correspondence to:
Publication Dates
-
Publication in this collection
29 May 2013 -
Date of issue
June 2013
History
-
Received
22 Oct 2012 -
Accepted
01 Mar 2013