Abstract
Objective: To verify the influence of physical performance on elderly mortality, functionality and life satisfaction. Materials and methods: A follow-up was performed on 900 Brazilian non-hospitalized elderly in the period 2008-2016, in which 154 deaths from natural causes were included in the survival analysis. Results: the worst grip strength (RR = 1.60; CI 95% = 1.15-2.23, p = 0.005) and gait speed (RR = 1.82; CI 95% = 1.30-2.55, p < 0.001) performances were associated with increased mortality risk. Age was a confounding factor for strength (RR = 1.06; CI 95% = 1.03-1.09, p < 0.001) and rheumatoid arthritis was a confounding factor for speed (RR = 2.02; CI 95% = 1.36-3.01, p < 0.001). The elderly with good physical performance realized more instrumental and advanced activities of daily living, and good gait performance had a significant effect on life satisfaction (F = 6.87, p = 0.009). Conclusions: good physical performance seems to be fundamental for longevity and for accomplishing daily tasks. Furthermore, good mobility can affect life satisfaction-related mechanisms.
Key words
Mortality; Functionality; Life satisfaction
Resumo
O objetivo deste artigo é verificar a influência do desempenho físico na mortalidade, funcionalidade e satisfação com a vida de idosos. Foi realizado o seguimento de 900 idosos brasileiros não hospitalizados entre os anos de 2008 e 2016, no qual foram incluídos na análise de sobrevivência 154 óbitos por causas naturais. Os piores desempenhos de força de preensão manual (R.R. = 1,60; IC 95% = 1,15-2,23; p = 0,005) e de velocidade usual de marcha (R.R. = 1,82; IC 95% = 1,30-2,55; p < 0,001) associaram-se com o aumento do risco de mortalidade. A idade foi um fator de confusão para a força (R.R. = 1,06; IC 95% = 1,03-1,09; p < 0,001) e a artrite reumatoide foi um fator de confusão para a velocidade (R.R. = 2,02; IC 95% = 1,36-3,01; p < 0,001). Os idosos com bom desempenho físico faziam mais atividades instrumentais e avançadas da vida diária, e o bom desempenho de marcha apresentou efeito significativo na satisfação com a vida (F = 6,87; p = 0,009). O bom desempenho físico parece ser fundamental para a longevidade e para a realização de tarefas do cotidiano. Além disso, a boa mobilidade pode afetar mecanismos relacionados à satisfação com a vida.
Palavras-chave
Mortalidade; Funcionalidade; Satisfação com a vida
Introduction
In elderly patients, estimates of physical performance are essential parameters for health assessment. The most commonly used physical performance variables are handgrip strength and gait speed. The first consists of an indicator of isometric muscular strength, which is related to mobility, daily physical activity level and sarcopenia11 Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001; 56(3):M146-156.,22 Cruz-Jentoft AJ, Landi F, Topinkova E, Michel JP. Understanding sarcopenia as a geriatric syndrome. Current Opinion in Clinical Nutrition & Metabolic Care 2010; 13(1):1-7.. Gait speed, in turn, is associated with the strength of lower limbs33 Buchner DM, Larson EB, Wagner EH, Koepsell TD, De Lateur BJ. Evidence for a non-linear relationship between leg strength and gait speed. Age and ageing 1996; 25(5):386-391. and physical disability44 Guralnik JM, Ferrucci L, Pieper CF, Leveille SG, Markides KS, Ostir GV, Wallace RB. Lower extremity function and subsequent disability: consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J Gerontol A Biol Sci Med Sci 2000; 55(4):M221-M231.. That is, they are measures that allow to infer other physical capacities and require low economic expenditure, and become valuable tools in clinical and scientific practices.
These physical performance variables can also be used to predict future events. Studies have shown that poor handgrip strength55 Wu Y, Wang W, Liu T, Zhang D. Association of Grip Strength With Risk of All-Cause Mortality, Cardiovascular Diseases, and Cancer in Community-Dwelling Populations: A Meta-analysis of Prospective Cohort Studies. J Am Med Dir Assoc 2017; 18(6):551-e517,66 Metter EJ, Talbot LA, Schrager M, Conwit R. Skeletal muscle strength as a predictor of all-cause mortality in healthy men. J Gerontol A Biol Sci Med Sci 2002; 57(10):B359-B365. and mobility77 Pamoukdjian F, Lévy V, Sebbane G, Boubaya M, Landre T, Bloch-Queyrat C, Paillaud E, Zelek L: Slow gait speed is an independent predictor of early death in older cancer outpatients: Results from a prospective cohort study. The journal of nutrition, health & aging 2017; 21(2):202-206.
8 Hardy SE, Perera S, Roumani YF, Chandler JM, Studenski SA. Improvement in usual gait speed predicts better survival in older adults. J Am Geriatr Soc 2007; 55(11):1727-1734.
9 Olaya B, Moneta MV, Démenech-Abella J, Miret M, Bayes I, Ayuso-Mateos JL, Haro JM. Mobility difficulties, physical activity and all-cause mortality risk in a nationally-representative sample of older adults. J Gerontol A Biol Sci Med Sci 2017.
10 Studenski S, Perera S, Patel K, Rosano C, Faulkner K, Inzitari M, Brach J, Chandler J, Cawthon P, Connor EB. Gait speed and survival in older adults. Jama 2011; 305(1):50-58.-1111 Taekema DG, Gussekloo J, Westendorp RGJ, de Craen AJM, Maier AB. Predicting survival in oldest old people. Am J Med 2012; 125(12):1188-1194. are associated with an increased risk of mortality. Despite this, few studies have investigated the influence of these two variables simultaneously and in non-hospitalized elderly1212 Nofuji Y, Shinkai S, Taniguchi Y, Amano H, Nishi M, Murayama H, Fujiwara Y, Suzuki T. Associations of walking speed, grip strength, and standing balance with total and cause-specific mortality in a general population of Japanese elders. J Am Med Dir Assoc 2016; 17(2):184-e181..
Considering that low handgrip strength levels are associated with an increased risk of motor limitation1313 Sallinen J, Stenholm S, Rantanen T, Heliövaara M, Sainio P, Koskinen S. Hand-grip strength cut points to screen older persons at risk for mobility limitation. J Am Geriatr Soc 2010; 58(9):1721-1726. and that the frailty process affects the organic systems simultaneously1414 Lang P-O, Michel J-P, Zekry D. Frailty syndrome: a transitional state in a dynamic process. Gerontology 2009; 55(5):539-549., then perhaps the use of these variables in association ensures greater predictive reliability.
Also, guidelines on healthy aging surpassed the longevity paradigm, emphasizing the importance of maintaining functionality and autonomy in old age1515 Organização Mundial da Saúde (OMS). Relatório Mundial de Envelhecimento e Saúde. Geneva: WHO; 2015.. Thus, we should not only reflect on the quantity of life but also consider how those additional years are being lived. Therefore, this study aimed to verify the influence of physical performance on mortality, functionality and life satisfaction of the elderly.
Materials and methods
Cohort study
This is a cohort study in which a sample of 900 elderly individuals was monitored to investigate the influence of physical performance on the risk of mortality. The sample was established from the database of the Study on Brazilian Elderly Frailty (FIBRA), from which we selected the information of the participants of the city of Campinas-SP.
FIBRA was developed for the screening of frailty conditions of elderly residents in urban areas. Initiated in 2008, participants were 65 years of age or older and had no memory, attention, spatial orientation, speech, hearing, vision or mobility disorders, sequelae of stroke or advanced neurodegenerative disease. For more information, please read FIBRA1616 Neri AL, Yassuda MS, Araújo LF, Eulálio MC, Cabral BE, Siqueira MEC, Santos GA, Moura JGA. Metodologia e perfil sociodemográfico, cognitivo e de fragilidade de idosos comunitários de sete cidades brasileiras: Estudo FIBRA. Cad Saude Publica 2013; 29(4):778-792. study’s full methodology.
Mortality data
The date of death was identified through the Mortality Information System of the Municipality of Campinas-SP. The cause of death was obtained through the International Code of Diseases (ICD-10). December 31, 2016 was adopted as the deadline for the follow-up of the sample. Total follow-up time was 8.4 years, and the elderly who died from unnatural causes or who did not die during the follow-up period were censored. Among the unnatural causes of death were traffic accidents and accidents with firearms. Survival time was calculated by the difference between the date of entry in the study and date of death (or the cut-off date). The Research Ethics Committee of the State University of Campinas approved the study.
Physical performance
It consisted of handgrip strength and usual gait speed. The former was evaluated three consecutive times through a hydraulic dynamometer set in the dominant hand of the elderly. Performances were categorized dichotomically according to the median, with cutoff points adjusted for gender (weak: ≤ 34 kg men, ≤ 20.6 kg women). Gait speed corresponded to the travel time, at a usual pace, of 4.6 meters, three consecutive times. The simple mean travel time was used to calculate the mean speed (Vm = Δs / Δt). According to the median, we used the gender-adjusted dichotomous classification (slow: ≤ 1.00 m/s men; ≤0.91 m/s women).
Confounding variables
Confounding variables were defined by theoretical criteria and were grouped in: age, psychological aspects, body composition and chronic diseases.
Psychological aspects
The Mini-Mental State Examination (MMSE)1717 Folstein MF, Folstein SE, McHugh PR. "Mini-mental state": a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975; 12(3):189-198. was applied to screen cognitive function. The definition of cutoff points followed the recommendations of the Brazilian Academy of Neurology, which is based on Brucki et al.1818 Brucki SMD, Nitrini R, Caramelli P, Bertolucci PHF, Okamoto IH: Sugestões para o uso do mini-exame do estado mental no Brasil. Arq Neuropsiquiatr 2003; 61(3B):777-781. and on a standard deviation. The definition of cut-off points is important because, according to Neri et al.1616 Neri AL, Yassuda MS, Araújo LF, Eulálio MC, Cabral BE, Siqueira MEC, Santos GA, Moura JGA. Metodologia e perfil sociodemográfico, cognitivo e de fragilidade de idosos comunitários de sete cidades brasileiras: Estudo FIBRA. Cad Saude Publica 2013; 29(4):778-792., cognitive impairment could compromise the validity of self-reported responses. Therefore, cut-off points adjusted for schooling time were adopted: illiterate=17; 1-4 years=22; 5-8 years=24; ≥ 9 years=26.
Participants scoring above the cut-off point in the MMSE responded to the Abridged Geriatric Depression Scale (GDS-15). GDS-15 was categorized as follows: <6 = no depressive symptoms; ≥ 6 = with depressive symptoms1919 Batistoni SST, Neri AL, Cupertino APFB. Validade da escala de depressão do Center for Epidemiological Studies entre idosos brasileiros. Rev Saude Publica 2007; 41(4):598-605..
Body composition
It consisted of the classification of overweight by the Body Mass Index (BMI)2020 Moretto MC, Tadoni MI, Neri AL, Guariento ME. Associations among self-reported diabetes, nutritional status, and socio-demographic variables in community-dwelling older adults. Revista de Nutrição 2014; 27(6):653-664. and risk by the Waist to Hip Ratio (WHR)2121 Bray GA, Gray DS. Obesity. Part I-Pathogenesis. Western Journal of Medicine 1988; 149(4):429.. BMI: < 23 low weight; ≥ 23 and < 28 normal weight; ≥ 28 and < 30 overweight; ≥ 30 obesity. The risk score for the WHR was adjusted for gender: Men: < 0.91 low; 0.91-0.98 moderate; > 0.98 high. Women: < 0.76 low; 0.76-0.83 moderate; > 0.83: high.
Chronic diseases
A questionnaire was applied that asked the elderly or family member (if the score was below the MMSE cutoff point) whether the doctor had diagnosed heart disease, hypertension, diabetes, cancer, lung disease, arthritis and osteoporosis2222 Alves LC, Leimann BCQ, Vasconcelos MEL, Carvalho MS, Vasconcelos AGG, Fonseca TCO. A influência das doenças crônicas na capacidade funcional dos idosos do Município de São Paulo, Brasil. Cad Saude Publica 2007; 23(8):1924-1930..
Activities of daily living and life satisfaction
The elderly who scored above the cut-off point in the MMSE were asked about the activities of daily living (ADLs) and their life satisfaction level.
The Basic Activities of Daily Living (BADLs) consisted of items related to self-care, in which the elderly were classified as “independent” or “dependent”2323 Lino VTS, Pereira SRM, Bastos Camacho LA, Ribeiro Filho ST, Buksman S. Adaptação transcultural da Escala de Independência em Atividades da Vida Diária (Escala de Katz). Cad Saude Publica 2008; 24(1):103-112.. One point was assigned for each “independent” task and zero for each task that the elderly could not perform alone. The maximum score was 6 points.
The Instrumental Activities of Daily Living (IADLs) consisted of 7 items about household tasks, in which the elderly was classified as “independent”, “partially independent” or “dependent”2424 Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Nursing Research 1970; 19(3):278.. Three points were assigned to each “independent” item, two points for “partially dependent” tasks and one point for “dependent” items. The maximum score was 21 points.
The Advanced Activities of Daily Living (AADLs) corresponded to 16 items on activities more complicated than BADLs and IADLs, in which the elderly were classified as “do”, “do not do” or “never did”2525 Reuben DB, Laliberte L, Hiris J, Mor V. A hierarchical exercise scale to measure function at the advanced activities of daily living (AADL) level. J Am Geriatr Soc 1990; 38(8):855-861.. For the score of this tool, we considered the activities that the elderly do and stopped doing, and we disregarded the activities never performed. Then, we calculated the percentage value representing the proportion of activities that the elderly still performed at the baseline, using the following formula:
The score ranged from 0 to 100, with functionality directly proportional to the score.
Life satisfaction consisted of 8 items evaluating aspects, such as overall satisfaction, comparison with others same age, ability to handle everyday chores, social relationships, environment, access to health services and transportation, which were classified as “very satisfied”, “more or less satisfied” or “not very satisfied”2626 Neri AL. Bienestar subjetivo en la vida adulta y en la vejez: hacia una psicología positiva; en América Latina. Revista Latinoamericana de Psicología 2002; 1(1):55-74.. Three points were awarded for each item “very satisfied”, two for “more or less satisfied” and one for items that the elderly person was “not very satisfied”. The maximum achievable score was 24 points.
Statistical analysis
Descriptive statistics were used to characterize the database. Proportions were compared through the chi-square test. The Mann-Whitney test was run for the variables with abnormal distribution. Kaplan-Meier curves were performed to verify the rate of mortality according to the strength and speed categories. The Log-Rank test compared survival functions. The association of handgrip strength and usual gait speed with mortality was verified using the Cox regression. Relative Risk (RR) indexes for mortality were initially calculated without any adjustment (Model 1). The following models were adjusted for age (Model 2), psychological aspects (Model 3), body composition (Model 4) and chronic diseases (Model 5).
A Multivariate General Linear Model was performed to verify the influence of physical performance on ADLs and life satisfaction. Variables with abnormal or heterogeneous distribution were transformed into Z-scores. The size of the effect was estimated by Eta Squared (η22 Cruz-Jentoft AJ, Landi F, Topinkova E, Michel JP. Understanding sarcopenia as a geriatric syndrome. Current Opinion in Clinical Nutrition & Metabolic Care 2010; 13(1):1-7.). All statistical analyses were done in the Statistical Package for the Social Sciences, version 24, and statistical significance was set at p < 0.05.
Results
Physical performance and mortality
One hundred sixty deaths (17.8%) were recorded during follow-up, of which 154 (17.1%) were due to natural causes. Considering only deaths from natural causes, mean survival was 4.4 years (± 1.9), with 4.6 years (± 1.8) for men and 4.3 years (± 1.9) for women. On average, the elderly died aged 79.7 years (± 7.2), with 78.7 years (± 7.2) for men and 80.4 years (± 7.2) for women. Figure 1 shows the comparison of handgrip strength (A) and usual gait speed (B) between survivors and deceased from natural causes, by gender. The Mann-Whitney test showed that survivors were stronger (men: p = 0.013, women: p < 0.001) and faster (men: p = 0.003; women: p < 0.001) at baseline against individuals who died during the follow-up period.
Comparison of handgrip strength (A) and usual gait speed (B) levels among surviving and deceased elderly according to sex.
* Statistically significant difference (p < 0.05) obtained with Mann-Whitney’s Test.
About the deceased, at baseline, 90 (58.4%) participants had low levels of handgrip, while mobility disability was found in 92 (59.7%) elderly.
Table 1 shows the characteristics of elderly survivors and those who died from natural causes. About the deceased, 2 (1.3%) preferred not to respond on the marital status. Thirty-eight (24.7%) had low weight, 65 (42.2%) normal weight and 23 (14.9%) were overweight. Regarding WHR, 59 (38.3%) elderly were classified as low risk, and 42 (27.3%) had a moderate risk. Overall, 689 (76.5%) elderly individuals were not diagnosed with cognitive impairment. Among them, 673 (97.7%) answered the GDS-15, of which 541 (80.4%) did not evidence depressive symptoms.
Characteristics in the baseline of the elderly of Campinas-SP according to the mortality status.
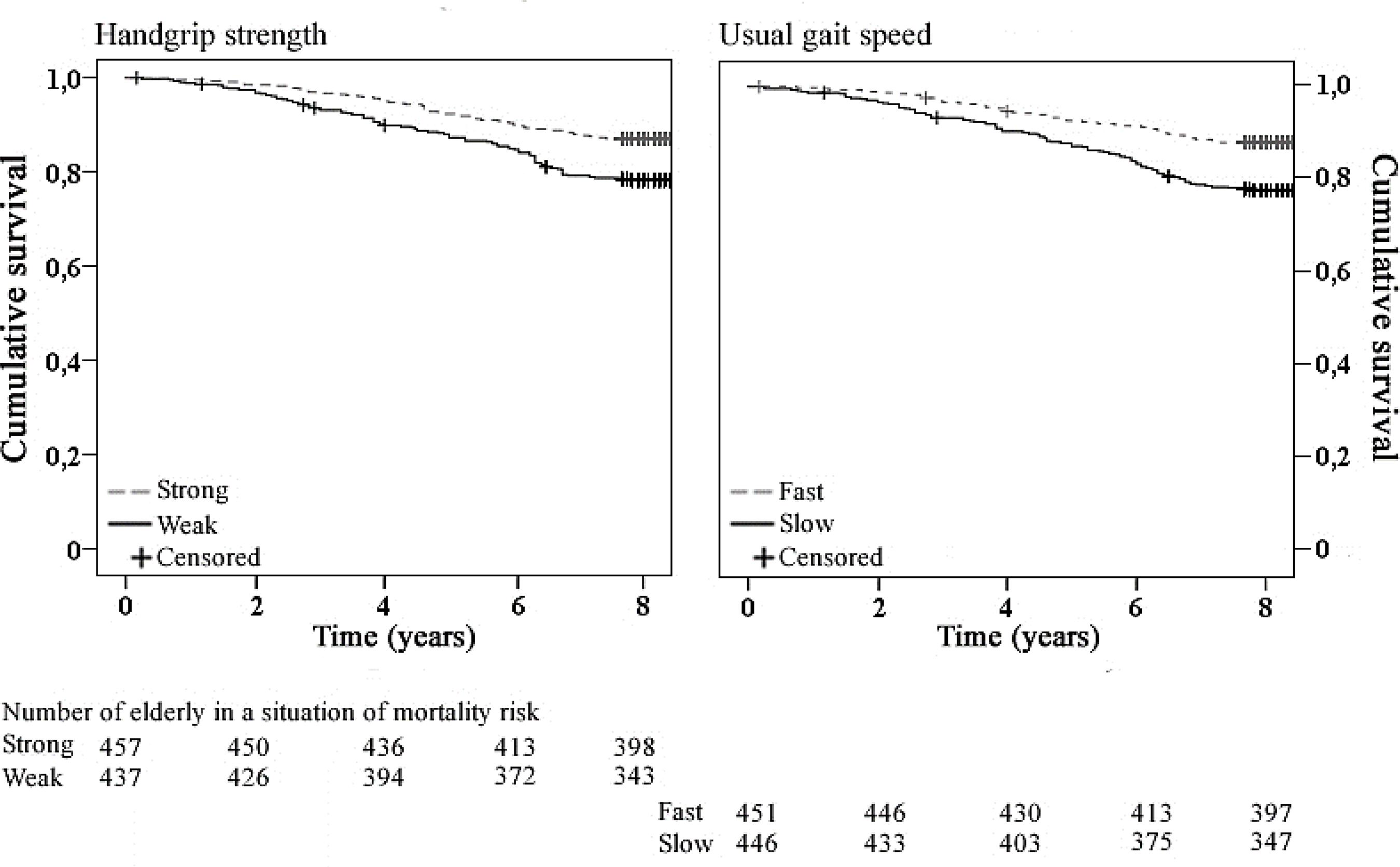
Figure 2 shows the Kaplan-Meier survival curves and the number of elderly at risk of mortality according to the follow-up time. When comparing survival functions, there was a statistically significant difference between the functions of handgrip strength (Log Rank: X2 = 12.18, p < 0.001) and gait speed (Log Rank: X2 = 16.64, p < 0.001), showing that the mortality speed was enhanced for individuals with both strength and mobility impairments.
Kaplan-Meier survival curves according to the levels of handgrip strength and usual gait speed of the elderly in Campinas-SP.
As shown in Table 2, the risk of mortality was 1.6 times higher for elderly with handgrip strength deficit. The effect was maintained in the adjustments of Models 3, 4 and 5, but age (Model 2) was a statistically significant confounding factor (RR = 1.06; 95% CI = 1.03-1.09, p < 0.001). Elderly patients with slow gait had 1.82 times higher mortality risk in relation to the elderly without mobility impairment. The effect was maintained in the adjustments of Models 2, 3 and 4, but the presence of rheumatoid arthritis (Model 5) was a statistically significant confounding factor (RR = 2.02; 95% CI = 1.36-3.01; p < 0.001).
Mortality risk estimated by Cox proportional hazards regression according to levels of handgrip strength and usual gait speed of elderly in Campinas-SP.
Physical performance, ADLs and life satisfaction
The population without cognitive impairment and that performed the physical tests totaled 655 elderly. Among them, 306 (46.7%) were classified as weak, while gait disability was observed in 283 (43.2%) elderly. The results for the multivariate model are shown in Table 3. There was a statistically significant effect of handgrip strength on IADLs (F = 4.72, η2 = 0.01) and AADLs (F = 7.03; η2 = 0.01). The gait speed showed a statistically significant effect on life satisfaction (F = 6.87; η2 = 0.01), IADLs (F = 19.85; η2 = 0.04) and AADLs (F = 6.02; η2 = 0.01). According to the means, the stronger elderly did more IADLs and AADLs, while faster elders were more satisfied with life, and made more IADLs and AADLs.
Influence of handgrip strength and the usual gait speed on life satisfaction and activities of daily living of the elderly in Campinas-SP.
Discussion
We verified the influence of two important components of physical fitness on the risk of mortality, functionality and life satisfaction of the elderly. The results suggest that elderly with good levels of handgrip strength and usual gait speed are more likely to live longer. Also, good physical performance seems to be fundamental for functionality in the face of daily demands and a good perception of life.
The findings about the influence of physical performance on mortality corroborate other studies77 Pamoukdjian F, Lévy V, Sebbane G, Boubaya M, Landre T, Bloch-Queyrat C, Paillaud E, Zelek L: Slow gait speed is an independent predictor of early death in older cancer outpatients: Results from a prospective cohort study. The journal of nutrition, health & aging 2017; 21(2):202-206.,88 Hardy SE, Perera S, Roumani YF, Chandler JM, Studenski SA. Improvement in usual gait speed predicts better survival in older adults. J Am Geriatr Soc 2007; 55(11):1727-1734.,2727 Al Snih S, Markides KS, Ray L, Ostir GV, Goodwin JS. Handgrip strength and mortality in older Mexican Americans. J Am Geriatr Soc 2002, 50(7):1250-1256.,2828 Rantanen T, Volpato S, Ferrucci L, Heikkinen E, Fried LP, Guralnik JM. Handgrip strength and cause-specific and total mortality in older disabled women: exploring the mechanism. J Am Geriatr Soc 2003, 51(5):636-641.. We found that low levels of handgrip strength were associated with increased risk of mortality in models adjusted for psychological aspects, body composition and chronic diseases. However, age was a statistically significant confounding factor, because a natural physical decline2929 Morley JE, Vellas B, van Kan GA, Anker SD, Bauer JM, Bernabei R, Cesari M, Chumlea WC, Doehner W, Evans J. Frailty consensus: a call to action. J Am Med Dir Assoc 2013; 14(6):392-397. occurs with age, affecting mainly strength3030 Goodpaster BH, Park SW, Harris TB, Kritchevsky SB, Nevitt M, Schwartz AV, Simonsick EM, Tylavsky FA, Visser M, Newman AB. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol A Biol Sci Med Sci 2006; 61(10):1059-1064. and muscle mass3131 Casas-Herrero A, Izquierdo M. Physical exercise as an efficient intervention in frail elderly persons. An Sist Sanit Navar 2012; 35(1):69-85..
Slow gait was associated with an increased risk of mortality in the models adjusted for age, psychological aspects and body composition. In contrast, self-reported rheumatoid arthritis was a statistically significant confounding factor. Rheumatoid arthritis is an inflammatory, limiting disease that may progress to irreversible conditions of deformity3232 Platto MJ, O'Connell PG, Hicks JE, Gerber LH. The relationship of pain and deformity of the rheumatoid foot to gait and an index of functional ambulation. J Rheumatol 1991; 18(1):38-43.. Weiss et al.3333 Weiss RJ, Wretenberg P, Stark A, Palmblad K, Larsson P, Gröndal L, Broström E. Gait pattern in rheumatoid arthritis. Gait & posture 2008; 28(2):229-234. showed that patients with rheumatoid arthritis had a substantial gait speed reduction. As justification, the disease impairs the mobility of several joints such as hip, knee and ankle, compromising gait’s biomechanics.
Two hypotheses are considered as possible physical performance actions mechanisms in the mortality risk: one situational and one inflammatory. The situational hypothesis begins with the assumption that low physical performance would signal a frailty process. Thus, it has already been shown that low levels of strength and gait are part of the frailty phenotype11 Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001; 56(3):M146-156.. Frail individuals may evidence sarcopenia, neuroendocrine and immunological dysregulation, which deplete energy reserves and organic resistance in response to stressors3434 Duarte YAO. Indicadores de fragilidade em pessoas idosas visando o estabelecimento de medidas preventivas. Boletim do instituto de saúde 2009; 47:49-52.. All these factors would make individuals more susceptible to diseases and infections, culminating in increased mortality risk.
The inflammatory hypothesis is based on the assumption that poor physical performance may make the elderly feel more fatigued when performing daily tasks, increasing the odds of immobility and sarcopenia3535 Casas-Herrero A, Izquierdo M. Ejercicio físico como intervención eficaz en el anciano frágil. An Sist Sanit Navar 2012; 35(1):69-85.. Physical inactivity may lead to a chronic inflammatory state, signaled by pro-inflammatory cytokines such as Interleukin 6 (IL-6), Tumor Necrosis Factor Alpha (TNF-α) and C-reactive protein (CRP)3636 Michaud M, Balardy L, Moulis G, Gaudin C, Peyrot C, Vellas B, Cesari M, Nourhashemi F. Proinflammatory cytokines, aging, and age-related diseases. J Am Med Dir Assoc 2013; 14(12):877-882.. These cytokines decrease protein synthesis, feedback the sarcopenia process, and increase the risk of chronic diseases3636 Michaud M, Balardy L, Moulis G, Gaudin C, Peyrot C, Vellas B, Cesari M, Nourhashemi F. Proinflammatory cytokines, aging, and age-related diseases. J Am Med Dir Assoc 2013; 14(12):877-882., which together would increase the mortality risk.
Another observed result is that good physical performance seems to benefit daily activities, especially more complex tasks. This is a predictable result, since day-to-day activities demand physical abilities such as strength, speed, flexibility, etc. The complexity of tasks, such as in the IADLs and AADLs increases with greater physical demand. Thus, maintenance of physical capacities is fundamental for the elderly to continue performing their usual tasks. This statement is in line with the World Health Organization (WHO) report on Aging and Health1515 Organização Mundial da Saúde (OMS). Relatório Mundial de Envelhecimento e Saúde. Geneva: WHO; 2015., which emphasizes healthy aging as one in which the elderly retain their functionality and maintain their independence and autonomy vis-à-vis daily demands.
There was no statistically significant effect of physical performance on the BADLs, which may be sample bias, since participants recruited for this study had a robust profile1616 Neri AL, Yassuda MS, Araújo LF, Eulálio MC, Cabral BE, Siqueira MEC, Santos GA, Moura JGA. Metodologia e perfil sociodemográfico, cognitivo e de fragilidade de idosos comunitários de sete cidades brasileiras: Estudo FIBRA. Cad Saude Publica 2013; 29(4):778-792., without physical and cognitive impairments. Thus, the detection of possible shortcomings was achieved only by increasing the complexity of daily tasks, such as in the IADLs and AADLs.
We also identified that the elderly without gait impairment were more satisfied with life. Although this result was statistically significant, we should use some caution in its analysis. After all, from the practical point of view, a negligible difference in the comparison of the groups and a low size of effect was observed. However, from the theoretical point of view, gait speed may influence regulation mechanisms, which can contribute to a better perception of life.
Life self-assessment is influenced by individual regulation in the face of the noxious effects of aging3737 Lerner RM, Weiner MB, Arbeit MR, Chase PA, Agans JP, Schmid KL, Warren AEA. Resilience across the life span. Annual review of gerontology and geriatrics 2012; 32(1):275-299.. Factors such as social roles, purpose in life3838 Schaefer SM, Boylan JM, Van Reekum CM, Lapate RC, Norris CJ, Ryff CD, Davidson RJ. Purpose in life predicts better emotional recovery from negative stimuli. PloS One 2013; 8(11):e80329., interrelationships3939 Ryff CD. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. Journal of personality and social psychology 1989; 57(6):1069. and even the comparison with worse-off elderly4040 Puts MTE, Shekary N, Widdershoven G, Heldens J, Lips P, Deeg DJH. What does quality of life mean to older frail and non-frail community-dwelling adults in the Netherlands? Qual Life Res 2007; 16(2):263-277. are some of the regulatory mechanisms. Also, it has been shown that individuals with restricted mobility tend to have low social involvement4141 Ekström H, Dahlin-Ivanoff S, Elmståhl S. Effects of walking speed and results of timed get-up-and-go tests on quality of life and social participation in elderly individuals with a history of osteoporosis-related fractures. Journal of Aging and Health 2011; 23(8):1379-1399.. That is, good mobility allows the elderly to remain active agents in their homes and communities, stimulating important aspects, such as a sense of purpose, self-esteem and self-confidence. Thus, we believe that people without mobility impairments tend to live more actively, and are more exposed to social, emotional and environmental interactions, which may reflect a better perception of life.
Taking into account that mortality and functionality were influenced by physical performance, then, we inevitably stress the importance of having an active life in old age, mainly through the practice of physical exercises, because, in addition to improving functionality4242 Yamada M, Arai H, Uemura K, Mori S, Nagai K, Tanaka B, Terasaki Y, Iguchi M, Aoyama T. Effect of resistance training on physical performance and fear of falling in elderly with different levels of physical well-being. Age and ageing 2011; 40(5):637-641., physical exercise acts on biological2929 Morley JE, Vellas B, van Kan GA, Anker SD, Bauer JM, Bernabei R, Cesari M, Chumlea WC, Doehner W, Evans J. Frailty consensus: a call to action. J Am Med Dir Assoc 2013; 14(6):392-397. and psychosocial aspects4343 McAuley E, Jerome GJ, Marquez DX, Elavsky S, Blissmer B. Exercise self-efficacy in older adults: social, affective, and behavioral influences. Annals of Behavioral Medicine 2003; 25(1):1-7., reducing mortality risks and enhancing the regulatory mechanisms mentioned above.
This study differs from other investigations by adopting measures of physical performance in association, applied in a sample of non-ambulatory elderly. The results shown here reinforce the importance of adopting physical performance variables in clinical and scientific practices, since they are reliable in the prediction of future events, such as death, in addition to being associated with subjective variables. This study enables reflections based solely on the time of existence, admitting physical performance as the key to an extensive and intense life.
As limitations of this study, the results should not be generalized for outpatient elderly, since, as previously mentioned, the profile of the population investigated was of robust and proactive elderly1616 Neri AL, Yassuda MS, Araújo LF, Eulálio MC, Cabral BE, Siqueira MEC, Santos GA, Moura JGA. Metodologia e perfil sociodemográfico, cognitivo e de fragilidade de idosos comunitários de sete cidades brasileiras: Estudo FIBRA. Cad Saude Publica 2013; 29(4):778-792.. Also, the cutoff points adopted for the classification of physical performance were different from other studies, which is due to a particular characteristic of the sample. An example is gait speed’s cutoff point. Descriptive results showed that males were generally faster than females. Had we used the same cutoff point adopted in other studies (0.8 m/s)4444 Alley DE, Shardell MD, Peters KW, McLean RR, Dam T-TL, Kenny AM, Fragala MS, Harris TB, Kiel DP, Guralnik JM. Grip strength cutpoints for the identification of clinically relevant weakness. J Gerontol A Biol Sci Med Sci 2014; 69(5):559-566.,4545 Studenski SA, Peters KW, Alley DE, Cawthon PM, McLean RR, Harris TB, Ferrucci L, Guralnik JM, Fragala MS, Kenny AM. The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. J Gerontol A Biol Sci Med Sci 2014; 69(5):547-558., we would have had an imbalanced proportion of individuals with and without mobility impairment (the same goes for strength). On the other hand, knowing that the general population includes men and women with varying levels of mobility, we chose to equalize the variables according to gender, minimizing sample-related biases. Finally, information on chronic diseases was obtained by self-report, which may have overestimated the prevalence of diseases.
Future studies may adopt repeated measures to investigate the magnitude of physical declines over the follow-up period, which may later be associated with mortality risk. Another suggestion relates to the evaluation of functionality. Here we infer it from the self-report of daily activities. An alternative would be the adoption of specific physical tests for the assessment of abilities such as balance, coordination and double task.
Conclusions
We showed that older adults with good physical performance live longer and better. Thus, good physical performance was associated with reduced risk of mortality and better functionality in daily tasks. The associated use of handgrip strength and the usual gait speed proved to be an effective strategy because of its good predictive capacity for death. Finally, we showed that mobility could act in protection mechanisms associated with life satisfaction.
Referências
-
1Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001; 56(3):M146-156.
-
2Cruz-Jentoft AJ, Landi F, Topinkova E, Michel JP. Understanding sarcopenia as a geriatric syndrome. Current Opinion in Clinical Nutrition & Metabolic Care 2010; 13(1):1-7.
-
3Buchner DM, Larson EB, Wagner EH, Koepsell TD, De Lateur BJ. Evidence for a non-linear relationship between leg strength and gait speed. Age and ageing 1996; 25(5):386-391.
-
4Guralnik JM, Ferrucci L, Pieper CF, Leveille SG, Markides KS, Ostir GV, Wallace RB. Lower extremity function and subsequent disability: consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J Gerontol A Biol Sci Med Sci 2000; 55(4):M221-M231.
-
5Wu Y, Wang W, Liu T, Zhang D. Association of Grip Strength With Risk of All-Cause Mortality, Cardiovascular Diseases, and Cancer in Community-Dwelling Populations: A Meta-analysis of Prospective Cohort Studies. J Am Med Dir Assoc 2017; 18(6):551-e517
-
6Metter EJ, Talbot LA, Schrager M, Conwit R. Skeletal muscle strength as a predictor of all-cause mortality in healthy men. J Gerontol A Biol Sci Med Sci 2002; 57(10):B359-B365.
-
7Pamoukdjian F, Lévy V, Sebbane G, Boubaya M, Landre T, Bloch-Queyrat C, Paillaud E, Zelek L: Slow gait speed is an independent predictor of early death in older cancer outpatients: Results from a prospective cohort study. The journal of nutrition, health & aging 2017; 21(2):202-206.
-
8Hardy SE, Perera S, Roumani YF, Chandler JM, Studenski SA. Improvement in usual gait speed predicts better survival in older adults. J Am Geriatr Soc 2007; 55(11):1727-1734.
-
9Olaya B, Moneta MV, Démenech-Abella J, Miret M, Bayes I, Ayuso-Mateos JL, Haro JM. Mobility difficulties, physical activity and all-cause mortality risk in a nationally-representative sample of older adults. J Gerontol A Biol Sci Med Sci 2017.
-
10Studenski S, Perera S, Patel K, Rosano C, Faulkner K, Inzitari M, Brach J, Chandler J, Cawthon P, Connor EB. Gait speed and survival in older adults. Jama 2011; 305(1):50-58.
-
11Taekema DG, Gussekloo J, Westendorp RGJ, de Craen AJM, Maier AB. Predicting survival in oldest old people. Am J Med 2012; 125(12):1188-1194.
-
12Nofuji Y, Shinkai S, Taniguchi Y, Amano H, Nishi M, Murayama H, Fujiwara Y, Suzuki T. Associations of walking speed, grip strength, and standing balance with total and cause-specific mortality in a general population of Japanese elders. J Am Med Dir Assoc 2016; 17(2):184-e181.
-
13Sallinen J, Stenholm S, Rantanen T, Heliövaara M, Sainio P, Koskinen S. Hand-grip strength cut points to screen older persons at risk for mobility limitation. J Am Geriatr Soc 2010; 58(9):1721-1726.
-
14Lang P-O, Michel J-P, Zekry D. Frailty syndrome: a transitional state in a dynamic process. Gerontology 2009; 55(5):539-549.
-
15Organização Mundial da Saúde (OMS). Relatório Mundial de Envelhecimento e Saúde Geneva: WHO; 2015.
-
16Neri AL, Yassuda MS, Araújo LF, Eulálio MC, Cabral BE, Siqueira MEC, Santos GA, Moura JGA. Metodologia e perfil sociodemográfico, cognitivo e de fragilidade de idosos comunitários de sete cidades brasileiras: Estudo FIBRA. Cad Saude Publica 2013; 29(4):778-792.
-
17Folstein MF, Folstein SE, McHugh PR. "Mini-mental state": a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975; 12(3):189-198.
-
18Brucki SMD, Nitrini R, Caramelli P, Bertolucci PHF, Okamoto IH: Sugestões para o uso do mini-exame do estado mental no Brasil. Arq Neuropsiquiatr 2003; 61(3B):777-781.
-
19Batistoni SST, Neri AL, Cupertino APFB. Validade da escala de depressão do Center for Epidemiological Studies entre idosos brasileiros. Rev Saude Publica 2007; 41(4):598-605.
-
20Moretto MC, Tadoni MI, Neri AL, Guariento ME. Associations among self-reported diabetes, nutritional status, and socio-demographic variables in community-dwelling older adults. Revista de Nutrição 2014; 27(6):653-664.
-
21Bray GA, Gray DS. Obesity. Part I-Pathogenesis. Western Journal of Medicine 1988; 149(4):429.
-
22Alves LC, Leimann BCQ, Vasconcelos MEL, Carvalho MS, Vasconcelos AGG, Fonseca TCO. A influência das doenças crônicas na capacidade funcional dos idosos do Município de São Paulo, Brasil. Cad Saude Publica 2007; 23(8):1924-1930.
-
23Lino VTS, Pereira SRM, Bastos Camacho LA, Ribeiro Filho ST, Buksman S. Adaptação transcultural da Escala de Independência em Atividades da Vida Diária (Escala de Katz). Cad Saude Publica 2008; 24(1):103-112.
-
24Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Nursing Research 1970; 19(3):278.
-
25Reuben DB, Laliberte L, Hiris J, Mor V. A hierarchical exercise scale to measure function at the advanced activities of daily living (AADL) level. J Am Geriatr Soc 1990; 38(8):855-861.
-
26Neri AL. Bienestar subjetivo en la vida adulta y en la vejez: hacia una psicología positiva; en América Latina. Revista Latinoamericana de Psicología 2002; 1(1):55-74.
-
27Al Snih S, Markides KS, Ray L, Ostir GV, Goodwin JS. Handgrip strength and mortality in older Mexican Americans. J Am Geriatr Soc 2002, 50(7):1250-1256.
-
28Rantanen T, Volpato S, Ferrucci L, Heikkinen E, Fried LP, Guralnik JM. Handgrip strength and cause-specific and total mortality in older disabled women: exploring the mechanism. J Am Geriatr Soc 2003, 51(5):636-641.
-
29Morley JE, Vellas B, van Kan GA, Anker SD, Bauer JM, Bernabei R, Cesari M, Chumlea WC, Doehner W, Evans J. Frailty consensus: a call to action. J Am Med Dir Assoc 2013; 14(6):392-397.
-
30Goodpaster BH, Park SW, Harris TB, Kritchevsky SB, Nevitt M, Schwartz AV, Simonsick EM, Tylavsky FA, Visser M, Newman AB. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol A Biol Sci Med Sci 2006; 61(10):1059-1064.
-
31Casas-Herrero A, Izquierdo M. Physical exercise as an efficient intervention in frail elderly persons. An Sist Sanit Navar 2012; 35(1):69-85.
-
32Platto MJ, O'Connell PG, Hicks JE, Gerber LH. The relationship of pain and deformity of the rheumatoid foot to gait and an index of functional ambulation. J Rheumatol 1991; 18(1):38-43.
-
33Weiss RJ, Wretenberg P, Stark A, Palmblad K, Larsson P, Gröndal L, Broström E. Gait pattern in rheumatoid arthritis. Gait & posture 2008; 28(2):229-234.
-
34Duarte YAO. Indicadores de fragilidade em pessoas idosas visando o estabelecimento de medidas preventivas. Boletim do instituto de saúde 2009; 47:49-52.
-
35Casas-Herrero A, Izquierdo M. Ejercicio físico como intervención eficaz en el anciano frágil. An Sist Sanit Navar 2012; 35(1):69-85.
-
36Michaud M, Balardy L, Moulis G, Gaudin C, Peyrot C, Vellas B, Cesari M, Nourhashemi F. Proinflammatory cytokines, aging, and age-related diseases. J Am Med Dir Assoc 2013; 14(12):877-882.
-
37Lerner RM, Weiner MB, Arbeit MR, Chase PA, Agans JP, Schmid KL, Warren AEA. Resilience across the life span. Annual review of gerontology and geriatrics 2012; 32(1):275-299.
-
38Schaefer SM, Boylan JM, Van Reekum CM, Lapate RC, Norris CJ, Ryff CD, Davidson RJ. Purpose in life predicts better emotional recovery from negative stimuli. PloS One 2013; 8(11):e80329.
-
39Ryff CD. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. Journal of personality and social psychology 1989; 57(6):1069.
-
40Puts MTE, Shekary N, Widdershoven G, Heldens J, Lips P, Deeg DJH. What does quality of life mean to older frail and non-frail community-dwelling adults in the Netherlands? Qual Life Res 2007; 16(2):263-277.
-
41Ekström H, Dahlin-Ivanoff S, Elmståhl S. Effects of walking speed and results of timed get-up-and-go tests on quality of life and social participation in elderly individuals with a history of osteoporosis-related fractures. Journal of Aging and Health 2011; 23(8):1379-1399.
-
42Yamada M, Arai H, Uemura K, Mori S, Nagai K, Tanaka B, Terasaki Y, Iguchi M, Aoyama T. Effect of resistance training on physical performance and fear of falling in elderly with different levels of physical well-being. Age and ageing 2011; 40(5):637-641.
-
43McAuley E, Jerome GJ, Marquez DX, Elavsky S, Blissmer B. Exercise self-efficacy in older adults: social, affective, and behavioral influences. Annals of Behavioral Medicine 2003; 25(1):1-7.
-
44Alley DE, Shardell MD, Peters KW, McLean RR, Dam T-TL, Kenny AM, Fragala MS, Harris TB, Kiel DP, Guralnik JM. Grip strength cutpoints for the identification of clinically relevant weakness. J Gerontol A Biol Sci Med Sci 2014; 69(5):559-566.
-
45Studenski SA, Peters KW, Alley DE, Cawthon PM, McLean RR, Harris TB, Ferrucci L, Guralnik JM, Fragala MS, Kenny AM. The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. J Gerontol A Biol Sci Med Sci 2014; 69(5):547-558.
Publication Dates
-
Publication in this collection
28 Oct 2019 -
Date of issue
Nov 2019
History
-
Received
29 Nov 2017 -
Accepted
24 Apr 2018 -
Published
26 Apr 2018