
Abstract
Pretermbirth (PTB) is a major obstetric problem associated with high rates of neonatal morbidity and mortality. The prevalence of PTB has not changed in the last decade; thus, the establishment of a screening test and effective treatment are warranted. Transvaginal ultrasoundmeasurement of the cervical length (TUCL) has been proposed as an effective method to screen pregnant women at a higher risk of experiencing PTB.
Objective
To evaluate the applicability and usefulness of second-trimester TUCL to predict PTB in a cohort of Portuguese pregnant women.
Methods
Retrospective cross-sectional cohort study including all singleton pregnant women who performed their second-trimester ultrasound (between weeks 18 and 22þ6 days) from January 2013 to October 2017 at Centro Hospitalar Universitário São João.
Results
Our cohort included 4,481 women. The prevalence of spontaneous PTB was of 4.0%, with 0.7% occurring before the 34th week of gestation. The mean TUCL was of 33.8mm,and percentiles 3, 5 and 10 corresponded toTUCLs of 25.0mm, 27.0mmand 29.0mmrespectively. The multiple logistic regression analysis, including maternal age, previous PTB and cervical surgery showed a significant negative association between TUCL and PTB, with an odds ratio (OR) of 0.92 (95% confidence interval [95%CI]: 0.90-0.95; p<0.001). The use of a TUCL of 20mm is the best cut-off, when compared with the 25-mm cut-off, improving the prediction of risk.
Conclusion
The present study showed an inverse association between TUCL and PTB, and that the inclusion of other risk factors like maternal age, previous PTB and cervical surgery can improve the screening algorithm. Furthermore, it emphasizes that the TUCL cut-off that defines short cervix can differ according to the population.
Keywords:
preterm birth; preterm birth screening; transvaginal ultrasound cervical length; cervical length cut-off
Resumo
O parto pré-termo (PPT) é uma grande complicação obstétrica que se associa a elevadas taxas de morbimortalidade neonatal. A sua prevalência não tem alterado na última década, sendo esencial determinar uma forma de rastreio e tratamento eficaz. A medição ecográfica transvaginal do comprimento cervical tem sido proposta como um método eficaz de rastreio das grávidas com risco aumentado de PPT.
Objetivo
Avaliar a aplicabilidade e utilidade da medição ecográfica transvaginal do comprimento cervical na previsão de PPT numa amostra de grávidas portuguesas.
Método
Estudo de coorte retrospectivo incluindo todas as grávidas com gestação unifetal que realizaram ecografia do 2° trimestre (de 18 a 22semanasþ6 dias) no Centro Hospitalar Universitário de São João entre janeiro de 2013 e outubro de 2017.
Resultados
A nossa amostra incluiu 4.481 mulheres. A prevalência de PPT espontâneo foi de 4,0%, sendo que 0,7% ocorreu antes das 34 semanas de gestação. A média do comprimento cervical por ecografia transvaginal foi 33,8mm, e os percentis 3, 5 e 10 da amostra corresponderam a comprimentos cervicais de 25,0mm, 27,0mm e 29,0mm, respetivamente. A regressão logística múltipla, que incluiu a idade materna, PPT anterior e antecedentes de conização, demonstrou uma associação estatisticamente significativa entre o comprimento cervical e o risco de PPT, com um risco relativo de 0,92 (intervalo de confiança de 95% [IC95%]: 0.90-0.95; p<0.001). A utilização de um valor de referência de comprimento cervical de 20mm, quando comparado com o valor de referência de 25 mm, melhora a previsão do risco de PPT.
Conclusão
Este estudo demostra uma associação entre o comprimento cervical avaliado por ecografia tranasvaginal e o risco de PPT, e salienta que a inclusão de outros fatores de risco, como idade materna, PPT anterior e antecedentes de conização podem melhorar o algoritmo de rastreio. Realça ainda que o valor de comprimento cervical utilizado para definir “colo curto” varia de acordo com a população em estudo.
Palavras-chave:
parto pré-termo; rastreio parto pré-termo; comprimento cervical por ecografia transvaginal; valor de referência do comprimento cervical
Introduction
The World Health Organization (WHO) defines preterm birth (PTB) as a delivery that occurs before the 37th week of gestation. It can occur spontaneously or due to medical induction (iatrogenic). Poorly understood to date, spontaneous PTB is a heterogeneous syndrome with multiple underlying pathophysiologic events and causes,.
Approximately 11% of infants worldwide are born too soon, corresponding to 15 million premature newborns every year.11 Glover AV, Manuck TA. Screening for spontaneous preterm birth and resultant therapies to reduce neonatal morbidity and mortality: A review. Semin Fetal Neonatal Med. 2018;23(02): 126-132. Doi: 10.1016/j.siny.2017.11.007
https://doi.org/10.1016/j.siny.2017.11.0...
22 Purisch SE, Gyamfi-Bannerman C. Epidemiology of pretermbirth. Semin Perinatol. 2017;41(07):387-391. Doi: 10.1053/j.semperi. 2017.07.009
https://doi.org/10.1053/j.semperi...
33 Vogel JP, Chawanpaiboon S, Moller AB, Watananirun K, Bonet M, Lumbiganon P. The global epidemiology of preterm birth. Best Pract Res Clin Obstet Gynaecol. 2018;52:3-12. Doi: 10.1016/j. bpobgyn.2018.04.003 The prevalence ranges from 5% in European developed countries to 18% in certain African countries, but these international differences may reflect variations in definitions rather than a true epidemiological difference. For example, the method to determine the gestational age and different viability limits can influence this rate. In Portugal, the prevalence of singleton live preterm newborns is of 7.4%.44 Zeitlin J, Szamotulska K, Drewniak N, et al; Euro-Peristat Preterm Study Group. Preterm birth time trends in Europe: a study of 19 countries. BJOG. 2013;120(11):1356-1365. Doi: 10.1111/1471-0528.12281
https://doi.org/10.1111/1471-0528.12281...
Despite all advances in medicine, PTB is still an important health problem, and the leading cause of neonatal mortality. Prematurity is associated with multiple neonatal complications and long-term morbidity.55 Frey HA, Klebanoff MA. The epidemiology, etiology, and costs of preterm birth. Semin Fetal Neonatal Med. 2016;21(02):68-73. Doi: 10.1016/j.siny.2015.12.011
https://doi.org/10.1016/j.siny.2015.12.0...
66 Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of under-5 mortality in 2000-15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet. 2016;388(10063):3027-3035. Doi: 10.1016/S0140-6736(16)31593-8
https://doi.org/10.1016/S0140-6736(16)31...
Fetal development is a continuum, and the risk of perinatal complications is inversely related to the gestational age at delivery. For this reason, some experts recommend a subclassification of PTB into early PTB (< 34 weeks) and late PTB (between 34 weeks and 36 weeks + 6 days), as the negative impact is different in the two groups.77 Committee on Practice Bulletins-Obstetrics, The American College of Obstetricians and Gynecologists. Practice bulletin no. 130: prediction and prevention of preterm birth. Obstet Gynecol. 2012;120(04):964-973. Doi: 10.1097/AOG.0b013e3182723b1b
https://doi.org/10.1097/AOG.0b013e318272...
Infants born before the 32th week of gestation represent less than 2% of all premature births, but they contribute to 50% of the overall perinatal mortality.88 Dodd JM, Jones L, Flenady V, Cincotta R, Crowther CA. Prenatal administration of progesterone for preventing preterm birth in women considered to be at risk of pretermbirth. Cochrane Database Syst Rev. 2013;(07):CD004947. Doi: 10.1002/14651858.CD004947
https://doi.org/10.1002/14651858.CD00494...
Preterm birth is such a major economic and social burden that its reduction is one of the Millennium Development Goals established by the United Nations.99 Howson CP, Kinney MV, McDougall L, Lawn JEBorn Too Soon Preterm Birth Action Group. Born too soon: preterm birth matters. Reprod Health. 2013;10(Suppl 1):S1. Doi: 10.1186/1742-4755-10-S1-S1
https://doi.org/10.1186/1742-4755-10-S1-...
Unfortunately, despite all efforts, the rate of prematurity has not changed in the past 30 years, and, in 2016, the WHO included PTB as one of the top-10 priority research areas.1010 Yoshida S, Martines J, Lawn JE, et al; neonatal health research priority setting group. Setting research priorities to improve global newborn health and prevent stillbirths by 2025. J Glob Health. 2016;6(01):010508. Doi: 10.7189/jogh.06.010508
https://doi.org/10.7189/jogh.06.010508...
1111 Loureiro T, Cunha M, Montenegro N. [Sonographic measurement of cervical length and prediction of spontaneous preterm delivery: how useful is it?] Acta Med Port. 2006;19(05):395-404 Portuguese
During the last years, many risk scores have been proposed to predict PTB, but they all have a low sensitivity and poor positive predictive value (PPV).1212 Barde DMPS, Attal DMP. Transvaginal sonographic cervical length measurement as predictor of preterm delivery. Int J Med Sci Clin Invent. 2017;4(07):3129-3132. Doi: 10.18535/ijmsci/v4i7.17
https://doi.org/10.18535/ijmsci/v4i7.17...
1313 Krupa FG, Faltin D, Cecatti JG, Surita FGC, Souza JP. Predictors of preterm birth. Int J Gynaecol Obstet. 2006;94(01):5-11. Doi: 10.1016/j.ijgo.2006.03.022
https://doi.org/10.1016/j.ijgo.2006.03.0...
The history of previous spontaneous PTB, for example, is the most significant risk factor known, but only 10% to 15% of PTBs occur after a previous event.1414 Temming LA, Durst JK, Tuuli MG, et al. Universal cervical length screening: implementation and outcomes. Am J Obstet Gynecol. 2016;214(04):523.e1-523.e8. Doi: 10.1016/j.ajog.2016.02.002
https://doi.org/10.1016/j.ajog.2016.02.0...
1515 McIntosh J, Feltovich H, Berghella V, Manuck TSociety for Maternal-Fetal Medicine (SMFM). Electronic address: pubs@smfm.org. The role of routine cervical length screening in selected high- and low-risk women for preterm birth prevention. Am J Obstet Gynecol. 2016;215(03):B2-B7. Doi: 10.1016/j.ajog.2016.04.027
https://doi.org/10.1016/j.ajog.2016.04.0...
As the majority of spontaneous PTBs occur in low-risk pregnancies, Andersen et al.1616 Andersen HF, Nugent CE,Wanty SD, Hayashi RH. Prediction of risk for preterm delivery by ultrasonographic measurement of cervical length. Am J Obstet Gynecol. 1990;163(03):859-867. Doi: 10.1016/0002-9378(90)91084-p
https://doi.org/10.1016/0002-9378(90)910...
(1990) proposed the use of transvaginal ultrasound measurement of the cervical length (TUCL) as a predictor of PTB. Since then, the technique has been well standardized, and its reproducibility, confirmed.1717 Leung TN, Pang MW, Leung TY, Poon CF, Wong SM, Lau TK. Cervical length at 18-22 weeks of gestation for prediction of spontaneous preterm delivery in Hong Kong Chinese women. Ultrasound Obstet Gynecol. 2005;26(07):713-717. Doi: 10.1002/uog.2617
https://doi.org/10.1002/uog.2617...
1818 Burger M, Weber-Rössler T, Willmann M. Measurement of the pregnant cervix by transvaginal sonography: an interobserver study and new standards to improve the interobserver variability. Ultrasound Obstet Gynecol. 1997;9(03):188-193. Doi: 10.1046/j.1469-0705.1997.09030188.x
https://doi.org/10.1046/j.1469-0705.1997...
The risk of experiencing PTB is inversely correlated to the cervical length, but the ideal cut-off for clinical use is still controversial.1616 Andersen HF, Nugent CE,Wanty SD, Hayashi RH. Prediction of risk for preterm delivery by ultrasonographic measurement of cervical length. Am J Obstet Gynecol. 1990;163(03):859-867. Doi: 10.1016/0002-9378(90)91084-p
https://doi.org/10.1016/0002-9378(90)910...
1919 van Os MA, Kleinrouweler CE, Schuit E, et al. Influence of cut-off value on prevalence of short cervical length. Ultrasound Obstet Gynecol. 2017;49(03):330-336. Doi: 10.1002/uog.15967
https://doi.org/10.1002/uog.15967...
2020 Wulff CB, Rode L, Rosthøj S, Hoseth E, Petersen OB, Tabor A. Transvaginal sonographic cervical length in first and second trimesters in a low-risk population: a prospective study. Ultrasound Obstet Gynecol. 2018;51(05):604-613. Doi: 10.1002/uog.17556
https://doi.org/10.1002/uog.17556...
2121 Markham KB, Iams JD. Measuring the cervical length. Clin Obstet Gynecol. 2016;59(02):252-263. Doi: 10.1097/GRF.0000000000000204
https://doi.org/10.1097/GRF.000000000000...
2222 Verma S, Meena BS, Pooja P, Sehra RN. A study of cervical length measured ultrasonographically in prediction of pretermdelivery. J Obstet Gynaecol. 2017;3(04):38-432323 Orzechowski KM, Nicholas SS, Baxter JK, Weiner S, Berghella V. Implementation of a universal cervical length screening program for the prevention of preterm birth. Am J Perinatol. 2014;31(12): 1057-1062. Doi: 10.1055/s-0034-1371710
https://doi.org/10.1055/s-0034-1371710...
By definition, a cervical length below the 10th centile for gestational age is considered “short.” This value varies according to the gestational age, the populational distribution of TUCL, and the prevalence of PTB. In the initial trials, the 10th centile was of 25 mm; therefore, this cut-off has been widely used.1515 McIntosh J, Feltovich H, Berghella V, Manuck TSociety for Maternal-Fetal Medicine (SMFM). Electronic address: pubs@smfm.org. The role of routine cervical length screening in selected high- and low-risk women for preterm birth prevention. Am J Obstet Gynecol. 2016;215(03):B2-B7. Doi: 10.1016/j.ajog.2016.04.027
https://doi.org/10.1016/j.ajog.2016.04.0...
2424 Berghella V, Baxter JK, Hendrix NW. Cervical assessment by ultrasound for preventing preterm delivery. Obstet Gynecol. 2009;114 (05):1140-1141. Doi: 10.1097/AOG.0b013e3181bdca73
https://doi.org/10.1097/AOG.0b013e3181bd...
2525 Jain S, Kilgore M, Edwards RK, Owen J. Revisiting the costeffectiveness of universal cervical length screening: importance of progesterone efficacy. AmJ Obstet Gynecol. 2016;215(01):101. e1-101.e7. Doi: 10.1016/j.ajog.2016.01.165
https://doi.org/10.1016/j.ajog.2016.01.1...
2626 Barros-Silva J, Pedrosa AC, Matias A. Sonographic measurement of cervical length as a predictor of preterm delivery: a systematic review. J Perinat Med. 2014;42(03):281-293. Doi: 10.1515/jpm-2013-0115
https://doi.org/10.1515/jpm-2013-0115...
2727 Iams JD, Goldenberg RL, Meis PJ, et al; National Institute of Child Health and Human Development Maternal Fetal Medicine Unit Network. The length of the cervix and the risk of spontaneous premature delivery. N Engl J Med. 1996;334(09):567-572. Doi: 10.1056/NEJM199602293340904
https://doi.org/10.1056/NEJM199602293340...
Since then, many cut-offs (from 15 mm to 30 mm) have been proposed, but none is consensual.
The main objective of the present study was to evaluate the applicability and usefulness of second-trimester TUCL to predict PTB in Portuguese pregnant women. We analyzed the distribution of TUCL in our cohort and determined the prevalence of short cervix using different cut-offs. Furthermore, we developed models to estimate the best TUCL cut-off in our cohort and improve its usefulness.
Methods
The present was an observational, retrospective cross-sectional cohort study carried out at the Obstetrics and Gynecology Department of Centro Hospitalar Universitário São João (CHUSJ), Portugal, after approval by the hospital's ethics committee (CES 81-17).
We included all singleton pregnant women who underwent the second-trimester ultrasound (the 18th week to the 22nd week + 6 days, determined by the crown-rump length before the 14th week) from January 2013 to October 2017 in this hospital. Delivery in the same institution and the existence of delivery data were also inclusion criteria. We excluded all women that had induced PTBs for medical reasons (including premature rupture of membranes), cervical cerclage performed prior to screening, diagnosis of chorioamnionitis, and deliveries before the 24th week.
The ultrasound exams at CHSJ are performed by obstetricians with accreditation from the Fetal Medicine Foundation (FMF) for cervical assessment. However, because the universal screening of TUCL is not mandatory, all ultrasound images available through the Astraia software (Astraia Software, GmbH, Munich, Germany) were reviewed in order to identify patients with an ultrasound image that complied with standard the rules of the FMF, which recommends the use of a transvaginal probe with the identification of the sagittal view of the cervix, occupying 75% of the image. Identification of the internal os, external os and cervical canal is essential. The measurement is performed in a straight line between the external and internal os. Care should be taken to distinguish between the cervical canal and the lower uterine segment (Fig. 1).

Transvaginal ultrasound measurement of the cervical length (TUCL). (A) Normal cervix; (B) short cervix.
At our hospital, all pregnant women with TUCLs ≤ 25 mm are considered to have a short cervix, and vaginal progesterone or the Arabin (Dr. Arabin GmbH & Co., Witten, Germany) pessary is suggested.
Maternal characteristics, medical history, obstetric history and delivery data were obtained from the database of the Obstetrics and Gynecology Department through the Obscare software. This data was compiled using the Statistical Package for the Social Sciences (SPSS, IBM Corp., Armonk, NY, US) software, version 24, for the statistical analyses. The continuous variables were expressed as means ± standard deviations (SDs), and frequencies and percentages were used to describe the categorical variables.
The frequencies of PTB were calculated according to different groups of cervical length measurements. The diagnostic ability of different TUCL cut-offs was evaluated in terms of sensitivity, specificity, PPV, negative predictive value (NPV), and the area under the curve (AUC).
An exploratory univariate analysis of clinical and demographic global data was first performed to determine the variables that predicted PTB and those associated with TUCL. All of the hypothesis tests conducted were two-tailed, and they included the Student t-test, the Chi-squared (χ2) test, and the Fisher exact test, as appropriate. Then, we developed a multivariate logistic regression model aiming to predict PTB as the outcome, using the TUCL as the explanatory variable, and including the main effects of maternal age, previous PTB and cervical surgery. For all of these analyses, values of p < 0.05 were considered statistically significant.
To select an optimal TUCL cut-off, we used the maximum likelihood and a confidence interval based on a likelihood ratio test. The likelihoods were calculated for a series of our multivariate logistic regression model using all TUCL cuto-ffs between 8 mm and 50 mm. The 95% lower and upper confidence bounds were determined as parameter values that reduce the maximum likelihood by χ2(0.05,1)/2 = 1.92. Using this optimal TUCL cut-off, we then assessed the potential differential effects across subgroups of risk factors using a stratified analysis. The effect modification among strata was checked using a test of homogeneity. Adjusted estimates were calculated using the Cochran-Mantel-Haenszel method.
In Portugal, the most used cut-off is TUCL ≤ 25 mm. In order to compare our optimal cut-off with the 25-mm cut-off, we classified each woman into groups of predicted probabilities derived from corresponding multivariate models using each cut-off. We then cross-classified these groups and compared them to the observed proportions of events in each group.
Results
During the aforementioned period, 8,016 women underwent a routine second-trimester ultrasound and delivery at CHUSJ. In total, 3,476 women were excluded from this group for the following reasons: delivery before the 24th week (n = 5),; medically-induced PTB (n = 241); cervical cerclage prior to ultrasound (n = 19); diagnosis of chorioamnionitiss (n = 3); absence of cervical length measurement (n = 958); and images of the cervical length measurement that did not comply with FMF recommendations (n = 2,426). Within the latter group, the major reason for exclusion was a transabdominal measurement (n = 1,275), instead of the transvaginal approach preconized by the FMF. Some women presented more than one exclusion criteria.
Our final cohort consisted of 4,481 women with a mean age of 30.7 ± 5.5 years. Primigravidae represented 45.4% of the sample, and 56.2% had no previous delivery. Most of them had no medical (86.5%) or obstetric (96.7%) relevant background. Only 1.6% of these women had a previous spontaneous PTB, and 0.9% had history of cervical surgery, the 2 major known risk factors for PTB.
Spontaneous delivery occurred in 64.3% of the cases, and 76.4% of the women underwent vaginal delivery. The prevalence of spontaneous PTB prevalence of the original cohort (8,016 women) was of 6.9% (553), and, after applying the exclusion criteria (with the sample reduced to 4,481 women) the prevalence dropped to 4.0% (n = 179), mainly due to the exclusion of medically-induced PTB. In total, 96.0% (n = 149) of the cases of PTB occurred between the 34th and 37th weeks, and 0.7% (n = 30) occurred before 34th week of gestation. The maternal and clinical characteristics of our cohort are described in table 1.
The mean gestational age at the time of the ultrasound was 21 weeks + 3 days, with a distribution of 0.2% (8) at 18 weeks, 0.5% (22) at 19 weeks, 12.4% (555) at 20 weeks, 66.5% (2979) at 21 weeks, and 20.5% (917) at 22 weeks. The mean TUCL was of 33.8 mm ± 4.8 mm (range: 3.0 mm to 53.0 mm). Percentiles 3, 5 and 10 corresponded to TUCLs of 25.0 mm, 27.0 mm and 29.0 mm respectively. Table 2 presents the frequency of term and preterm births across different TUCL intervals. Among pregnant women with PTB, the TUCL was significantly lower (mean: 31.6 mm; 95%CI: 30.7–32.5 mm) compared to the measurements of those with term birth (mean: 33.9 mm; 95%CI: 33.8–34.0 mm; p < 0.001).
Even though the TUCL alone showed a high specificity to predict PTB, its diagnostic ability was limited by a very low sensitivity, with an AUC close to 0.5 for all different cut-offs studied, as depicted in table 3.
Sensitivity and specificity of the cervical length measurement to predict preterm birth and cumulative incidence of the different cut-offs
The univariate analysis (Tables 4 and 5) showed that maternal age ≥ 40 years, history of PTB, and cervical surgery were the main significant predictors of PTB. Additionally, history of PTB and previous cervical surgery were also associated with shorter TUCL, thus acting as confounders.
The multivariate logistic regression analysis, incorporating maternal age ≥ 40 years old, history of PTB, and previous cervical surgery, evaluated the impact of the TUCL as a predictor of PTB (Table 6).
Multivariate logistic regression analysis to evaluate the impact of transvaginal ultrasound measurement of the cervical length as a predictor of preterm birth
The estimated odds ratio (OR) for the effect of the TUCL on PTB, controlling for covariates, was of 0.92 (95%CI: 0.90–0.95; p < 0.001), which highlights the significant negative association between TUCL and PTB. The diagnostic ability of the multivariate model improved, showing an AUC of 0.65 (Fig. 2).
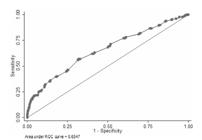
Graphic representations of sensitivity, specificity and area under the curve (AUC) of the multivariate model.
As expected, in the univariate analysis, the treatment with progesterone/pessary was associated with shorter TUCL, and thus, also with PTB, when considering the total study cohort. Within the group of women with a diagnosis of short cervix, 68% (n = 93) underwent treatment, and 13% (n = 18) declined it. There was, however, no significant difference between the frequency of PTB among women who accepted or declined progesterone or the pessary (14% versus 22.2% of PTB respectively; p = 0.472); therefore, the treatment was not included in our multivariate model.
To select the optimal TUCL cut-off, we ran several multivariate logistic regression models using different cut-offs (from 8 mm and 50 mm) associated with other variables like maternal age ≥ 40 years, history of PTB, and previous cervical surgery. Plotting the log likelihood from these models against the TUCL showed that a cut-off of 20 mm (95%CI: 19.5–22 mm) best discriminated 2 TUCL subgroups with differential odds for PTB (Fig. 3). Women with a short cervix, defined by TUCL ≤ 20 mm, had an OR of 12.2 (95%CI: 5.8–25.4; p < 0.001) compared with those with TUCL > 20 mm.

Plotting to determine the best TUCL cut-off based on multiple log likelihood of the logistic regression model (including maternal age ≥ 40 years, history of PTB, and previous cervical surgery), using cut-offs between 8 mm and 50 mm. The circle represents the cut-off that best discriminated the risk of experiencing PTB.
Considering maternal age ≥ 40 years, history of PTB and previous cervical surgery as the main risk factors for PTB, a stratified analysis was performed by separately evaluating women with at least 1 of these factors (n = 297) versus women who did not presented any of them (n = 4,184 [93.4%]) (Table 7). The significant association of a short cervix (TUCL ≤ 20 mm) with PTB was maintained in both groups, with an OR of 16.2 (95%CI: 2.7–97.1; p < 0.001) for women with risk factors, and an OR of 9.8 (95%CI: 4.1–23.7; p < 0.001) for women without them. There was no effect modification between the groups (p = 0.614, homogeneity test). Considering this stratification, the adjusted OR for women with short cervix (TUCL ≤ 20 mm) was of 11.4 (95%CI: 5.1–25.4; p < 0.001).
Distribution of the pregnant women according to group probability of preterm birth using transvaginal ultrasound measurement of the cervical length and presence/absence of risk factors (maternal age ≥ 40 years, previous PTB and cervical surgery). Cross-classification of the 25-mm cut-off group (most used cut-off) versus the 20-mm cut-off group (our best cut-off) and frequency of PTB in each subgroup
A simple comparison of the 20-mm and 25-mm cut-offs, based on AUCs of multivariate models, showed no statistical difference (20 mm: AUC = 0.59 [95%CI: 0.56–0.62] versus 25 mm: AUC = 0.60 [95%CI: 0.57–0.64]; p = 0.157). However, a better performance in the prediction of PTB of the 20-mm compared to the 25-mm cut-off was highlighted by comparing the distribution of women according to the prediction probabilities derived from the corresponding multivariate models. Globally, 15 (0.33%) women were reclassified to a different predicted-probability group when the multivariate model included the 20-mm instead of the 25-mm cut-off. As described in table 6, out of the 4 women upgraded to a higher probability (from 0.50-0.75 in the 25-mm model to > 0.75 in the 20-mm model), 75% (n = 3) experienced a PTB. On the other hand, out of the 8 women reclassified to a lower predicted probability (from 0.25-0.50 in the 25-mm model to < 0.25 in the 20-mm model), only 1 (12.5%) had PTB.
Discussion
Good practice of disease screening recommends that the condition be an important health problem and facilities for diagnosis and treatment be available, as already published in 1968 by the WHO.2828 Wilson JMG, Jungner G. Principles and practice of screening for disease. Geneva: World Health Organization; 1968
Preterm birth fulfills the first prerequisite, as it represents a major obstetric complication. Our cohort presents 4% (179) of spontaneous PTB, and this prevalence is similar to that of other studies regarding screening and treatment.2727 Iams JD, Goldenberg RL, Meis PJ, et al; National Institute of Child Health and Human Development Maternal Fetal Medicine Unit Network. The length of the cervix and the risk of spontaneous premature delivery. N Engl J Med. 1996;334(09):567-572. Doi: 10.1056/NEJM199602293340904
https://doi.org/10.1056/NEJM199602293340...
2929 Kuusela P, Jacobsson B, Söderlund M, et al. Transvaginal sonographic evaluation of cervical length in the second trimester of asymptomatic singleton pregnancies, and the risk of preterm delivery. Acta Obstet Gynecol Scand. 2015;94(06):598-607. Doi: 10.1111/aogs.12622
https://doi.org/10.1111/aogs.12622...
3030 Souka AP, Papastefanou I, Pilalis A, Kassanos D, Papadopoulos G. Implementation of universal screening for preterm delivery by mid-trimester cervical-length measurement. Ultrasound Obstet Gynecol. 2019;53(03):396-401. Doi: 10.1002/uog.19050
https://doi.org/10.1002/uog.19050...
A second assumption needed to implement a screening process is the existence of a test able to detect the high-risk population, and the TUCL satisfies this requirement. An inverse association between the TUCL and PTB, which was also observed in our study, has been widely documented.1616 Andersen HF, Nugent CE,Wanty SD, Hayashi RH. Prediction of risk for preterm delivery by ultrasonographic measurement of cervical length. Am J Obstet Gynecol. 1990;163(03):859-867. Doi: 10.1016/0002-9378(90)91084-p
https://doi.org/10.1016/0002-9378(90)910...
2121 Markham KB, Iams JD. Measuring the cervical length. Clin Obstet Gynecol. 2016;59(02):252-263. Doi: 10.1097/GRF.0000000000000204
https://doi.org/10.1097/GRF.000000000000...
2626 Barros-Silva J, Pedrosa AC, Matias A. Sonographic measurement of cervical length as a predictor of preterm delivery: a systematic review. J Perinat Med. 2014;42(03):281-293. Doi: 10.1515/jpm-2013-0115
https://doi.org/10.1515/jpm-2013-0115...
2727 Iams JD, Goldenberg RL, Meis PJ, et al; National Institute of Child Health and Human Development Maternal Fetal Medicine Unit Network. The length of the cervix and the risk of spontaneous premature delivery. N Engl J Med. 1996;334(09):567-572. Doi: 10.1056/NEJM199602293340904
https://doi.org/10.1056/NEJM199602293340...
2929 Kuusela P, Jacobsson B, Söderlund M, et al. Transvaginal sonographic evaluation of cervical length in the second trimester of asymptomatic singleton pregnancies, and the risk of preterm delivery. Acta Obstet Gynecol Scand. 2015;94(06):598-607. Doi: 10.1111/aogs.12622
https://doi.org/10.1111/aogs.12622...
3030 Souka AP, Papastefanou I, Pilalis A, Kassanos D, Papadopoulos G. Implementation of universal screening for preterm delivery by mid-trimester cervical-length measurement. Ultrasound Obstet Gynecol. 2019;53(03):396-401. Doi: 10.1002/uog.19050
https://doi.org/10.1002/uog.19050...
3131 Pedretti MK, Kazemier BM, Dickinson JE, Mol BW. Implementing universal cervical length screening in asymptomatic women with singleton pregnancies: challenges and opportunities. Aust N Z J Obstet Gynaecol. 2017;57(02):221-227. Doi: 10.1111/ajo.12586
https://doi.org/10.1111/ajo.12586...
3232 Conde-Agudelo A, Romero R. Vaginal progesterone to prevent preterm birth in pregnant women with a sonographic short cervix: clinical and public health implications. Am J Obstet Gynecol. 2016;214(02):235-242. Doi: 10.1016/j. ajog.2015.09.102 The TUCL in our cohort showed a high specificity to predict PTB, but low sensitivity and a poor AUC, results similar to those of other studies. Iams et al.2727 Iams JD, Goldenberg RL, Meis PJ, et al; National Institute of Child Health and Human Development Maternal Fetal Medicine Unit Network. The length of the cervix and the risk of spontaneous premature delivery. N Engl J Med. 1996;334(09):567-572. Doi: 10.1056/NEJM199602293340904
https://doi.org/10.1056/NEJM199602293340...
reported that TUCL ≤ 25 mm had a sensitivity of 37% and a specificity of 92%, but more recent studies obtained even lower sensitivities, such as 2.4% in the study by van der Ven et al.,3333 van der Ven J, van OsMA, Kazemier BM, et al. The capacity ofmidpregnancy cervical length to predict preterm birth in low-risk women: a national cohort study. Acta Obstet Gynecol Scand. 2015;94(11):1223-1234. Doi: 10.1111/aogs.12721
https://doi.org/10.1111/aogs.12721...
and 8.0% in the one by Esplin et al.3434 Esplin MS, Elovitz MA, Iams JD, et al; nuMoM2b Network. Predictive accuracy of serial transvaginal cervical lengths and quantitative vaginal fetal fibronectin levels for spontaneous preterm birth among nulliparous women. JAMA. 2017;317(10): 1047-1056. Doi: 10.1001/jama.2017.1373
https://doi.org/10.1001/jama.2017.1373...
Our multivariate model showed an improvement in the AUC value, highlighting that a combined screening including maternal age > 40 years, history of PTB and previous cervical surgery should be considered for screening, instead of the TUCL alone. The Society for Maternal-Fetal Medicine Publications Committee, in their 2012 guidelines, concluded that the most effective approach was to initiate treatment in low-risk women with a TUCL ≤ 20 mm, or high-risk pregnant women with a TUCL ≤ 25 mm, supporting that other risk factors should be included in the screening algorithm.3535 Society for Maternal-Fetal Medicine Publications Committee, with assistance of Vincenzo Berghella. Progesterone and preterm birth prevention: translating clinical trials data into clinical practice. Am J Obstet Gynecol. 2012;206(05):376-386. Doi:10.1016/j.ajog.2012.03.010
https://doi.org/10.1016/j.ajog.2012.03.0...
Nowadays, there is no debate that second-trimester TUCL is the most powerful screening instrument available, but the best cut-off to separate normal from short cervixes is still controversial.1616 Andersen HF, Nugent CE,Wanty SD, Hayashi RH. Prediction of risk for preterm delivery by ultrasonographic measurement of cervical length. Am J Obstet Gynecol. 1990;163(03):859-867. Doi: 10.1016/0002-9378(90)91084-p
https://doi.org/10.1016/0002-9378(90)910...
1919 van Os MA, Kleinrouweler CE, Schuit E, et al. Influence of cut-off value on prevalence of short cervical length. Ultrasound Obstet Gynecol. 2017;49(03):330-336. Doi: 10.1002/uog.15967
https://doi.org/10.1002/uog.15967...
2020 Wulff CB, Rode L, Rosthøj S, Hoseth E, Petersen OB, Tabor A. Transvaginal sonographic cervical length in first and second trimesters in a low-risk population: a prospective study. Ultrasound Obstet Gynecol. 2018;51(05):604-613. Doi: 10.1002/uog.17556
https://doi.org/10.1002/uog.17556...
2121 Markham KB, Iams JD. Measuring the cervical length. Clin Obstet Gynecol. 2016;59(02):252-263. Doi: 10.1097/GRF.0000000000000204
https://doi.org/10.1097/GRF.000000000000...
2222 Verma S, Meena BS, Pooja P, Sehra RN. A study of cervical length measured ultrasonographically in prediction of pretermdelivery. J Obstet Gynaecol. 2017;3(04):38-432323 Orzechowski KM, Nicholas SS, Baxter JK, Weiner S, Berghella V. Implementation of a universal cervical length screening program for the prevention of preterm birth. Am J Perinatol. 2014;31(12): 1057-1062. Doi: 10.1055/s-0034-1371710
https://doi.org/10.1055/s-0034-1371710...
As most parameters in medicine, there is no biological TUCL cut-off, and defining “short” is not an easy task. Lower cut-offs present good specificity but low sensitivity, but higher values (like 29 mm) lead to an increase in the false-positive rate.2727 Iams JD, Goldenberg RL, Meis PJ, et al; National Institute of Child Health and Human Development Maternal Fetal Medicine Unit Network. The length of the cervix and the risk of spontaneous premature delivery. N Engl J Med. 1996;334(09):567-572. Doi: 10.1056/NEJM199602293340904
https://doi.org/10.1056/NEJM199602293340...
3636 Taipale P, Hiilesmaa V. Sonographic measurement of uterine cervix at 18-22 weeks' gestation and the risk of preterm delivery. Obstet Gynecol. 1998;92(06):902-907. Doi: 10.1016/s0029-7844 (98)00346-9
https://doi.org/10.1016/s0029-7844...
Most guidelines recommend a 25-mm cut-off, as it corresponds to the 10th percentile in the initial published trials.77 Committee on Practice Bulletins-Obstetrics, The American College of Obstetricians and Gynecologists. Practice bulletin no. 130: prediction and prevention of preterm birth. Obstet Gynecol. 2012;120(04):964-973. Doi: 10.1097/AOG.0b013e3182723b1b
https://doi.org/10.1097/AOG.0b013e318272...
1515 McIntosh J, Feltovich H, Berghella V, Manuck TSociety for Maternal-Fetal Medicine (SMFM). Electronic address: pubs@smfm.org. The role of routine cervical length screening in selected high- and low-risk women for preterm birth prevention. Am J Obstet Gynecol. 2016;215(03):B2-B7. Doi: 10.1016/j.ajog.2016.04.027
https://doi.org/10.1016/j.ajog.2016.04.0...
1616 Andersen HF, Nugent CE,Wanty SD, Hayashi RH. Prediction of risk for preterm delivery by ultrasonographic measurement of cervical length. Am J Obstet Gynecol. 1990;163(03):859-867. Doi: 10.1016/0002-9378(90)91084-p
https://doi.org/10.1016/0002-9378(90)910...
2727 Iams JD, Goldenberg RL, Meis PJ, et al; National Institute of Child Health and Human Development Maternal Fetal Medicine Unit Network. The length of the cervix and the risk of spontaneous premature delivery. N Engl J Med. 1996;334(09):567-572. Doi: 10.1056/NEJM199602293340904
https://doi.org/10.1056/NEJM199602293340...
3636 Taipale P, Hiilesmaa V. Sonographic measurement of uterine cervix at 18-22 weeks' gestation and the risk of preterm delivery. Obstet Gynecol. 1998;92(06):902-907. Doi: 10.1016/s0029-7844 (98)00346-9
https://doi.org/10.1016/s0029-7844...
3737 Hassan SS, Romero R, Berry SM, et al. Patients with an ultrasonographic cervical length < or =15mm have nearly a 50% risk of early spontaneous preterm delivery. Am J Obstet Gynecol. 2000; 182(06):1458-1467. Doi: 10.1067/mob.2000.106851
https://doi.org/10.1067/mob.2000.106851...
3838 Romero R, Conde-Agudelo A, Da Fonseca E, et al. Vaginal progesterone for preventing preterm birth and adverse perinatal outcomes in singleton gestations with a short cervix: a meta-analysis of individual patient data. Am J Obstet Gynecol. 2018;218(02): 161-180. Doi: 10.1016/j.ajog.2017.11.576
https://doi.org/10.1016/j.ajog.2017.11.5...
3939 Fonseca EB, Celik E, Parra M, Singh M, Nicolaides KHFetal Medicine Foundation Second Trimester Screening Group. Progesterone and the risk of pretermbirth among women with a short cervix. N Engl J Med. 2007;357(05):462-469. Doi: 10.1056/NEJMoa067815
https://doi.org/10.1056/NEJMoa067815...
4040 Berghella V, Palacio M, Ness A, Alfirevic Z, Nicolaides KH, Saccone G. Cervical length screening for prevention of preterm birth in singleton pregnancy with threatened preterm labor: systematic review and meta-analysis of randomized controlled trials using individual patient-level data. Ultrasound ObstetGynecol. 2017;49 (03):322-329. Doi: 10.1002/uog.17388
https://doi.org/10.1002/uog.17388...
However, more recent studies showed a lower prevalence of short cervices defined as TUCL ≤ 25 mm, averaging 2.5%.1414 Temming LA, Durst JK, Tuuli MG, et al. Universal cervical length screening: implementation and outcomes. Am J Obstet Gynecol. 2016;214(04):523.e1-523.e8. Doi: 10.1016/j.ajog.2016.02.002
https://doi.org/10.1016/j.ajog.2016.02.0...
3333 van der Ven J, van OsMA, Kazemier BM, et al. The capacity ofmidpregnancy cervical length to predict preterm birth in low-risk women: a national cohort study. Acta Obstet Gynecol Scand. 2015;94(11):1223-1234. Doi: 10.1111/aogs.12721
https://doi.org/10.1111/aogs.12721...
3434 Esplin MS, Elovitz MA, Iams JD, et al; nuMoM2b Network. Predictive accuracy of serial transvaginal cervical lengths and quantitative vaginal fetal fibronectin levels for spontaneous preterm birth among nulliparous women. JAMA. 2017;317(10): 1047-1056. Doi: 10.1001/jama.2017.1373
https://doi.org/10.1001/jama.2017.1373...
4141 Orzechowski KM, Boelig RC, Baxter JK, Berghella V. A universal transvaginal cervical length screening program for preterm birth prevention. Obstet Gynecol. 2014;124(03):520-525. Doi: 10.1097/AOG.0000000000000428
https://doi.org/10.1097/AOG.000000000000...
4242 Son M, Grobman WA, Ayala NK, Miller ES. A universal midtrimester transvaginal cervical length screening program and its associated reduced preterm birth rate. Am J Obstet Gynecol. 2016;214(03):365.e1-365.e5. Doi: 10.1016/j.ajog.2015.12.020
https://doi.org/10.1016/j.ajog.2015.12.0...
Our results follow this new tendency, as the prevalence of TUCL ≤ 25 mm was of only 3% (134), and the 10th TUCL percentile in our cohort corresponded to 29.0 mm.
TUCL distribution can be influenced by many factors; therefore, the ideal cut-off can change in different populations. That said, we concluded that the best cut-off for our cohort was 20 mm (Fig. 3). This value enabled us to improve the prediction of the risk of experiencing PTB mainly by reducing the false-positive rate (8 women were reclassified as low probability, and only 1 (15.5%) of them experienced a PTB).
In parallel to studies on the efficacy of TUCL screening, cost-analysis studies were also conducted, which concluded that TUCL screening is cost-effective even if we assume a low incidence of short cervical length and a modest impact of the treatment with progesterone.2525 Jain S, Kilgore M, Edwards RK, Owen J. Revisiting the costeffectiveness of universal cervical length screening: importance of progesterone efficacy. AmJ Obstet Gynecol. 2016;215(01):101. e1-101.e7. Doi: 10.1016/j.ajog.2016.01.165
https://doi.org/10.1016/j.ajog.2016.01.1...
3131 Pedretti MK, Kazemier BM, Dickinson JE, Mol BW. Implementing universal cervical length screening in asymptomatic women with singleton pregnancies: challenges and opportunities. Aust N Z J Obstet Gynaecol. 2017;57(02):221-227. Doi: 10.1111/ajo.12586
https://doi.org/10.1111/ajo.12586...
4343 Crosby DA, Miletin J, Semberova J, Daly S. Is routine transvaginal cervical length measurement cost-effective in a populationwhere the risk of spontaneous pretermbirth is low? Acta Obstet Gynecol Scand. 2016;95(12):1391-1395. Doi: 10.1111/aogs.13021
https://doi.org/10.1111/aogs.13021...
4444 Einerson BD, Grobman WA, Miller ES. Cost-effectiveness of riskbased screening for cervical length to prevent pretermbirth. AmJ Obstet Gynecol. 2016;215(01):100.e1-100.e7. Doi: 10.1016/j.ajog.2016.01.192
https://doi.org/10.1016/j.ajog.2016.01.1...
4545 Werner EF, Hamel MS, Orzechowski K, Berghella V, Thung SF. Costeffectiveness of transvaginal ultrasound cervical length screening in singletons without a prior preterm birth: an update. Am J Obstet Gynecol. 2015;213(04):554.e1-554.e6. Doi: 10.1016/j.ajog.2015.06.020
https://doi.org/10.1016/j.ajog.2015.06.0...
The Federation of Gynecology and Obstetrics Working Group on Best Practices in Maternal Fetal Medicine recommended universal transvaginal cervical length screening and vaginal progesterone when TUCL< 25 mm.4646 FigoWorking Group On Best Practice In Maternal-Fetal Medicine International Federation of Gynecology and Obstetrics. Best practice in maternal-fetal medicine. Int J Gynaecol Obstet. 2015;128 (01):80-82. Doi: 10.1016/j.ijgo.2014.10.011
https://doi.org/10.1016/j.ijgo.2014.10.0...
Subsequently, studies4141 Orzechowski KM, Boelig RC, Baxter JK, Berghella V. A universal transvaginal cervical length screening program for preterm birth prevention. Obstet Gynecol. 2014;124(03):520-525. Doi: 10.1097/AOG.0000000000000428
https://doi.org/10.1097/AOG.000000000000...
4242 Son M, Grobman WA, Ayala NK, Miller ES. A universal midtrimester transvaginal cervical length screening program and its associated reduced preterm birth rate. Am J Obstet Gynecol. 2016;214(03):365.e1-365.e5. Doi: 10.1016/j.ajog.2015.12.020
https://doi.org/10.1016/j.ajog.2015.12.0...
4747 Newnham JP,White SW, Meharry S, et al. Reducing pretermbirth by a statewide multifaceted program: an implementation study. Am J Obstet Gynecol. 2017;216(05):434-442. Doi: 10.1016/j.ajog.2016.11.1037
https://doi.org/10.1016/j.ajog.2016.11.1...
using this recommendation showed a reduction in the PTB rate when universal screening was applied. Son et al.,4242 Son M, Grobman WA, Ayala NK, Miller ES. A universal midtrimester transvaginal cervical length screening program and its associated reduced preterm birth rate. Am J Obstet Gynecol. 2016;214(03):365.e1-365.e5. Doi: 10.1016/j.ajog.2015.12.020
https://doi.org/10.1016/j.ajog.2015.12.0...
for example, obtained a 20% reduction in the rate of PTBs after implementing TUCL screening, even with a very low prevalence short cervixes (TUCL ≤ 25 mm: 0.89%). The negative impact of PTB is so huge that every approach able to reduce it has a positive impact and should be considered.
Conclusion
Preterm birth represents a major health problem, and strategies to prevent are important. The present study showed an inverse association between TUCL and PTB, and emphasized that other factors like maternal age, history PTB and previous cervical surgery can improve the screening algorithm. The value that defines a short cervix can differ in each population, and, for our cohort, the best cut-off was 20 mm. Even though TUCL has a low diagnostic performance, it is the best screening method available to predict PTB, and TUCL screening has been shown to reduce the PTB rate.
References
-
1Glover AV, Manuck TA. Screening for spontaneous preterm birth and resultant therapies to reduce neonatal morbidity and mortality: A review. Semin Fetal Neonatal Med. 2018;23(02): 126-132. Doi: 10.1016/j.siny.2017.11.007
» https://doi.org/10.1016/j.siny.2017.11.007 -
2Purisch SE, Gyamfi-Bannerman C. Epidemiology of pretermbirth. Semin Perinatol. 2017;41(07):387-391. Doi: 10.1053/j.semperi. 2017.07.009
» https://doi.org/10.1053/j.semperi -
3Vogel JP, Chawanpaiboon S, Moller AB, Watananirun K, Bonet M, Lumbiganon P. The global epidemiology of preterm birth. Best Pract Res Clin Obstet Gynaecol. 2018;52:3-12. Doi: 10.1016/j. bpobgyn.2018.04.003
-
4Zeitlin J, Szamotulska K, Drewniak N, et al; Euro-Peristat Preterm Study Group. Preterm birth time trends in Europe: a study of 19 countries. BJOG. 2013;120(11):1356-1365. Doi: 10.1111/1471-0528.12281
» https://doi.org/10.1111/1471-0528.12281 -
5Frey HA, Klebanoff MA. The epidemiology, etiology, and costs of preterm birth. Semin Fetal Neonatal Med. 2016;21(02):68-73. Doi: 10.1016/j.siny.2015.12.011
» https://doi.org/10.1016/j.siny.2015.12.011 -
6Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of under-5 mortality in 2000-15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet. 2016;388(10063):3027-3035. Doi: 10.1016/S0140-6736(16)31593-8
» https://doi.org/10.1016/S0140-6736(16)31593-8 -
7Committee on Practice Bulletins-Obstetrics, The American College of Obstetricians and Gynecologists. Practice bulletin no. 130: prediction and prevention of preterm birth. Obstet Gynecol. 2012;120(04):964-973. Doi: 10.1097/AOG.0b013e3182723b1b
» https://doi.org/10.1097/AOG.0b013e3182723b1b -
8Dodd JM, Jones L, Flenady V, Cincotta R, Crowther CA. Prenatal administration of progesterone for preventing preterm birth in women considered to be at risk of pretermbirth. Cochrane Database Syst Rev. 2013;(07):CD004947. Doi: 10.1002/14651858.CD004947
» https://doi.org/10.1002/14651858.CD004947 -
9Howson CP, Kinney MV, McDougall L, Lawn JEBorn Too Soon Preterm Birth Action Group. Born too soon: preterm birth matters. Reprod Health. 2013;10(Suppl 1):S1. Doi: 10.1186/1742-4755-10-S1-S1
» https://doi.org/10.1186/1742-4755-10-S1-S1 -
10Yoshida S, Martines J, Lawn JE, et al; neonatal health research priority setting group. Setting research priorities to improve global newborn health and prevent stillbirths by 2025. J Glob Health. 2016;6(01):010508. Doi: 10.7189/jogh.06.010508
» https://doi.org/10.7189/jogh.06.010508 -
11Loureiro T, Cunha M, Montenegro N. [Sonographic measurement of cervical length and prediction of spontaneous preterm delivery: how useful is it?] Acta Med Port. 2006;19(05):395-404 Portuguese
-
12Barde DMPS, Attal DMP. Transvaginal sonographic cervical length measurement as predictor of preterm delivery. Int J Med Sci Clin Invent. 2017;4(07):3129-3132. Doi: 10.18535/ijmsci/v4i7.17
» https://doi.org/10.18535/ijmsci/v4i7.17 -
13Krupa FG, Faltin D, Cecatti JG, Surita FGC, Souza JP. Predictors of preterm birth. Int J Gynaecol Obstet. 2006;94(01):5-11. Doi: 10.1016/j.ijgo.2006.03.022
» https://doi.org/10.1016/j.ijgo.2006.03.022 -
14Temming LA, Durst JK, Tuuli MG, et al. Universal cervical length screening: implementation and outcomes. Am J Obstet Gynecol. 2016;214(04):523.e1-523.e8. Doi: 10.1016/j.ajog.2016.02.002
» https://doi.org/10.1016/j.ajog.2016.02.002 -
15McIntosh J, Feltovich H, Berghella V, Manuck TSociety for Maternal-Fetal Medicine (SMFM). Electronic address: pubs@smfm.org. The role of routine cervical length screening in selected high- and low-risk women for preterm birth prevention. Am J Obstet Gynecol. 2016;215(03):B2-B7. Doi: 10.1016/j.ajog.2016.04.027
» https://doi.org/10.1016/j.ajog.2016.04.027 -
16Andersen HF, Nugent CE,Wanty SD, Hayashi RH. Prediction of risk for preterm delivery by ultrasonographic measurement of cervical length. Am J Obstet Gynecol. 1990;163(03):859-867. Doi: 10.1016/0002-9378(90)91084-p
» https://doi.org/10.1016/0002-9378(90)91084-p -
17Leung TN, Pang MW, Leung TY, Poon CF, Wong SM, Lau TK. Cervical length at 18-22 weeks of gestation for prediction of spontaneous preterm delivery in Hong Kong Chinese women. Ultrasound Obstet Gynecol. 2005;26(07):713-717. Doi: 10.1002/uog.2617
» https://doi.org/10.1002/uog.2617 -
18Burger M, Weber-Rössler T, Willmann M. Measurement of the pregnant cervix by transvaginal sonography: an interobserver study and new standards to improve the interobserver variability. Ultrasound Obstet Gynecol. 1997;9(03):188-193. Doi: 10.1046/j.1469-0705.1997.09030188.x
» https://doi.org/10.1046/j.1469-0705.1997.09030188.x -
19van Os MA, Kleinrouweler CE, Schuit E, et al. Influence of cut-off value on prevalence of short cervical length. Ultrasound Obstet Gynecol. 2017;49(03):330-336. Doi: 10.1002/uog.15967
» https://doi.org/10.1002/uog.15967 -
20Wulff CB, Rode L, Rosthøj S, Hoseth E, Petersen OB, Tabor A. Transvaginal sonographic cervical length in first and second trimesters in a low-risk population: a prospective study. Ultrasound Obstet Gynecol. 2018;51(05):604-613. Doi: 10.1002/uog.17556
» https://doi.org/10.1002/uog.17556 -
21Markham KB, Iams JD. Measuring the cervical length. Clin Obstet Gynecol. 2016;59(02):252-263. Doi: 10.1097/GRF.0000000000000204
» https://doi.org/10.1097/GRF.0000000000000204 -
22Verma S, Meena BS, Pooja P, Sehra RN. A study of cervical length measured ultrasonographically in prediction of pretermdelivery. J Obstet Gynaecol. 2017;3(04):38-43
-
23Orzechowski KM, Nicholas SS, Baxter JK, Weiner S, Berghella V. Implementation of a universal cervical length screening program for the prevention of preterm birth. Am J Perinatol. 2014;31(12): 1057-1062. Doi: 10.1055/s-0034-1371710
» https://doi.org/10.1055/s-0034-1371710 -
24Berghella V, Baxter JK, Hendrix NW. Cervical assessment by ultrasound for preventing preterm delivery. Obstet Gynecol. 2009;114 (05):1140-1141. Doi: 10.1097/AOG.0b013e3181bdca73
» https://doi.org/10.1097/AOG.0b013e3181bdca73 -
25Jain S, Kilgore M, Edwards RK, Owen J. Revisiting the costeffectiveness of universal cervical length screening: importance of progesterone efficacy. AmJ Obstet Gynecol. 2016;215(01):101. e1-101.e7. Doi: 10.1016/j.ajog.2016.01.165
» https://doi.org/10.1016/j.ajog.2016.01.165 -
26Barros-Silva J, Pedrosa AC, Matias A. Sonographic measurement of cervical length as a predictor of preterm delivery: a systematic review. J Perinat Med. 2014;42(03):281-293. Doi: 10.1515/jpm-2013-0115
» https://doi.org/10.1515/jpm-2013-0115 -
27Iams JD, Goldenberg RL, Meis PJ, et al; National Institute of Child Health and Human Development Maternal Fetal Medicine Unit Network. The length of the cervix and the risk of spontaneous premature delivery. N Engl J Med. 1996;334(09):567-572. Doi: 10.1056/NEJM199602293340904
» https://doi.org/10.1056/NEJM199602293340904 -
28Wilson JMG, Jungner G. Principles and practice of screening for disease. Geneva: World Health Organization; 1968
-
29Kuusela P, Jacobsson B, Söderlund M, et al. Transvaginal sonographic evaluation of cervical length in the second trimester of asymptomatic singleton pregnancies, and the risk of preterm delivery. Acta Obstet Gynecol Scand. 2015;94(06):598-607. Doi: 10.1111/aogs.12622
» https://doi.org/10.1111/aogs.12622 -
30Souka AP, Papastefanou I, Pilalis A, Kassanos D, Papadopoulos G. Implementation of universal screening for preterm delivery by mid-trimester cervical-length measurement. Ultrasound Obstet Gynecol. 2019;53(03):396-401. Doi: 10.1002/uog.19050
» https://doi.org/10.1002/uog.19050 -
31Pedretti MK, Kazemier BM, Dickinson JE, Mol BW. Implementing universal cervical length screening in asymptomatic women with singleton pregnancies: challenges and opportunities. Aust N Z J Obstet Gynaecol. 2017;57(02):221-227. Doi: 10.1111/ajo.12586
» https://doi.org/10.1111/ajo.12586 -
32Conde-Agudelo A, Romero R. Vaginal progesterone to prevent preterm birth in pregnant women with a sonographic short cervix: clinical and public health implications. Am J Obstet Gynecol. 2016;214(02):235-242. Doi: 10.1016/j. ajog.2015.09.102
-
33van der Ven J, van OsMA, Kazemier BM, et al. The capacity ofmidpregnancy cervical length to predict preterm birth in low-risk women: a national cohort study. Acta Obstet Gynecol Scand. 2015;94(11):1223-1234. Doi: 10.1111/aogs.12721
» https://doi.org/10.1111/aogs.12721 -
34Esplin MS, Elovitz MA, Iams JD, et al; nuMoM2b Network. Predictive accuracy of serial transvaginal cervical lengths and quantitative vaginal fetal fibronectin levels for spontaneous preterm birth among nulliparous women. JAMA. 2017;317(10): 1047-1056. Doi: 10.1001/jama.2017.1373
» https://doi.org/10.1001/jama.2017.1373 -
35Society for Maternal-Fetal Medicine Publications Committee, with assistance of Vincenzo Berghella. Progesterone and preterm birth prevention: translating clinical trials data into clinical practice. Am J Obstet Gynecol. 2012;206(05):376-386. Doi:10.1016/j.ajog.2012.03.010
» https://doi.org/10.1016/j.ajog.2012.03.010 -
36Taipale P, Hiilesmaa V. Sonographic measurement of uterine cervix at 18-22 weeks' gestation and the risk of preterm delivery. Obstet Gynecol. 1998;92(06):902-907. Doi: 10.1016/s0029-7844 (98)00346-9
» https://doi.org/10.1016/s0029-7844 -
37Hassan SS, Romero R, Berry SM, et al. Patients with an ultrasonographic cervical length < or =15mm have nearly a 50% risk of early spontaneous preterm delivery. Am J Obstet Gynecol. 2000; 182(06):1458-1467. Doi: 10.1067/mob.2000.106851
» https://doi.org/10.1067/mob.2000.106851 -
38Romero R, Conde-Agudelo A, Da Fonseca E, et al. Vaginal progesterone for preventing preterm birth and adverse perinatal outcomes in singleton gestations with a short cervix: a meta-analysis of individual patient data. Am J Obstet Gynecol. 2018;218(02): 161-180. Doi: 10.1016/j.ajog.2017.11.576
» https://doi.org/10.1016/j.ajog.2017.11.576 -
39Fonseca EB, Celik E, Parra M, Singh M, Nicolaides KHFetal Medicine Foundation Second Trimester Screening Group. Progesterone and the risk of pretermbirth among women with a short cervix. N Engl J Med. 2007;357(05):462-469. Doi: 10.1056/NEJMoa067815
» https://doi.org/10.1056/NEJMoa067815 -
40Berghella V, Palacio M, Ness A, Alfirevic Z, Nicolaides KH, Saccone G. Cervical length screening for prevention of preterm birth in singleton pregnancy with threatened preterm labor: systematic review and meta-analysis of randomized controlled trials using individual patient-level data. Ultrasound ObstetGynecol. 2017;49 (03):322-329. Doi: 10.1002/uog.17388
» https://doi.org/10.1002/uog.17388 -
41Orzechowski KM, Boelig RC, Baxter JK, Berghella V. A universal transvaginal cervical length screening program for preterm birth prevention. Obstet Gynecol. 2014;124(03):520-525. Doi: 10.1097/AOG.0000000000000428
» https://doi.org/10.1097/AOG.0000000000000428 -
42Son M, Grobman WA, Ayala NK, Miller ES. A universal midtrimester transvaginal cervical length screening program and its associated reduced preterm birth rate. Am J Obstet Gynecol. 2016;214(03):365.e1-365.e5. Doi: 10.1016/j.ajog.2015.12.020
» https://doi.org/10.1016/j.ajog.2015.12.020 -
43Crosby DA, Miletin J, Semberova J, Daly S. Is routine transvaginal cervical length measurement cost-effective in a populationwhere the risk of spontaneous pretermbirth is low? Acta Obstet Gynecol Scand. 2016;95(12):1391-1395. Doi: 10.1111/aogs.13021
» https://doi.org/10.1111/aogs.13021 -
44Einerson BD, Grobman WA, Miller ES. Cost-effectiveness of riskbased screening for cervical length to prevent pretermbirth. AmJ Obstet Gynecol. 2016;215(01):100.e1-100.e7. Doi: 10.1016/j.ajog.2016.01.192
» https://doi.org/10.1016/j.ajog.2016.01.192 -
45Werner EF, Hamel MS, Orzechowski K, Berghella V, Thung SF. Costeffectiveness of transvaginal ultrasound cervical length screening in singletons without a prior preterm birth: an update. Am J Obstet Gynecol. 2015;213(04):554.e1-554.e6. Doi: 10.1016/j.ajog.2015.06.020
» https://doi.org/10.1016/j.ajog.2015.06.020 -
46FigoWorking Group On Best Practice In Maternal-Fetal Medicine International Federation of Gynecology and Obstetrics. Best practice in maternal-fetal medicine. Int J Gynaecol Obstet. 2015;128 (01):80-82. Doi: 10.1016/j.ijgo.2014.10.011
» https://doi.org/10.1016/j.ijgo.2014.10.011 -
47Newnham JP,White SW, Meharry S, et al. Reducing pretermbirth by a statewide multifaceted program: an implementation study. Am J Obstet Gynecol. 2017;216(05):434-442. Doi: 10.1016/j.ajog.2016.11.1037
» https://doi.org/10.1016/j.ajog.2016.11.1037
Publication Dates
-
Publication in this collection
18 June 2021 -
Date of issue
Apr 2021
History
-
Received
17 Jan 2020 -
Accepted
16 Dec 2020



