Abstract
Background:
Renal failure is common in patients with chronic heart failure, with a prevalence ranging from 20 % to 57% worldwide. It is associated with a poor prognosis and a high risk of readmission.
Objectives:
The purpose of our study is to show the epidemiological, clinical, paraclinical and therapeutic features of Moroccan patients with chronic heart failure who had developed a chronic renal failure. The endpoints were cardiac death and any cause of hospitalization.
Methods:
563 patients followed for chronic heart failure at the heart failure unit in the Department of Cardiology of the University Hospital Ibn Rushd of Casablanca in Morocco, between July 30, 2012 and July 30, 2016 were assessed. Patients were divided into two groups according to the presence or absence of cardiorenal syndrome.
Results:
Compared to patients who had no cardiorenal syndrome, patients with cardiorenal syndrome tended to be more aged, hypertensive and diabetic. Clinically more patients were at dyspnea stage III or IV. Biologically their hemoglobin was lower and their blood uric acid level was higher. Regarding echocardiography, their ejection fraction of the left ventricle was lower, with more of systolic dysfunction of the right ventricle and pulmonary hypertension in the CRS group, with a higher risk of readmission (p < 0.0001). The mortality was significantly higher in the group CRS (p < 0.0001).
Conclusion:
The deterioration of renal function in chronic renal failure is associated with poor prognosis, including a high risk of rehospitalization, cardiovascular events and death. Patients who are elderly, diabetic, with a low left ventricular ejection fraction and pulmonary hypertension are the most concerned.
Keywords:
Cardio-Renal Syndrome; Heart Failure; Renal Insufficiency Chronic / mortality; Renal Insufficiency Chronic / prognosis; Patient Readmission
Resumo
Fundamento: A insuficiência renal é comum em pacientes com insuficiência cardíaca crônica, com uma prevalência entre 20% a 57%, e está associada a um mau prognóstico e um alto risco de reinternações.
Objetivo:
O objetivo deste estudo foi apresentar características epidemiológicas, clínicas e terapêuticas de pacientes marroquinos com insuficiência cardíaca crônica que desenvolveram insuficiência renal crônica.
Métodos:
Foram avaliados 563 pacientes acompanhados por insuficiência cardíaca crônica na Unidade de Insuficiência Cardíaca do Departamento de Cardiologia do Hospital Universitário de Ibn Rushd em Casablanca, Marrocos, entre 30 de julho de 2012 e 30 de julho de 2016. Os pacientes foram divididos em dois grupos de acordo com a presença ou ausência de síndrome cardiorrenal.
Resultados:
Em comparação a pacientes que não desenvolveram síndrome cardiorrenal, os pacientes com síndrome cardiorrenal tenderam a ser mais velhos, hipertensos e diabéticos. Clinicamente, uma porcentagem mais alta dos pacientes apresentou dispneia estágio III ou IV. Biologicamente, os pacientes com SCR apresentaram níveis menores de hemoglobina e níveis plasmáticos maiores de ácido úrico. Em relação aos achados ecocardiográficos, esses pacientes também apresentaram menor FE do ventrículo esquerdo, com maior prevalência de hipertensão ventricular direita e hipertensão pulmonar, e maior risco de readmissão hospitalar (p < 0,0001).
Conclusão:
A deterioração da função renal na insuficiência renal crônica está associada com um pior prognóstico, incluindo um maior risco de readmissão hospitalar, eventos cardiovasculares, e morte. Maior atenção deve ser dada a pacientes idosos, diabéticos, com valores muito baixos de fração de ejeção do ventrículo esquerdo ou com hipertensão pulmonar.
Palavras-chave:
Síndrome Cardiorrenal; Insuficiência Cardíaca; Insuficiência Renal Crônica / mortalidade; Insuficiência Renal Crônica / prognóstico; Readmissão do Paciente
Introduction
Renal failure is common in patients with chronic heart failure, with a prevalence ranging from 20 % to 57% worldwide. It is associated with a poor prognosis and a high risk of readmission.11 de Silva R, Nikitin NP, Witte KK, Rigby AS, Goode K, Bhandari S, et al. Incidence of renal dysfunction over 6 months in patients with chronic heart failure due to left ventricular systolic dysfunction: contributing factors and relationship to prognosis. Eur Heart J. 2006;27(5):569-81. doi: 10.1093/eurheartj/ehi696.
https://doi.org/10.1093/eurheartj/ehi696...
There is a complex relationship between heart and kidney in patients with heart failure, and the exact pathophysiological mechanisms of this association remain unclear.22 Cole RT, Masoumi A, Triposkiadis F, Giamouzis G, Georgiopoulou V, Kalogeropoulos A, et al. Renal dysfunction in heart failure. Med Clin North Am. 2012;96(5):955-74. doi: 10.1016/j.mcna.2012.07.005.
https://doi.org/10.1016/j.mcna.2012.07.0...
Important pathophysiological triggers of renal disease progression include chronic increases in renal venous pressure, maladaptive activation of the renin-angiotensin -aldosterone axis and the sympathetic nervous system, as well as a chronic inflammatory state.33 Cruz DN, Schmidt-Ott KM, Vescovo G, House AA, Kellum JA, Ronco C, et al. Pathophysiology of cardiorenal syndrome type 2 in stable chronic heart failure: workgroup statements from the eleventh consensus conference of the Acute Dialysis Quality Initiative (ADQI). Contrib Nephrol. 2013;182:117-36. doi: 10.1159/000349968.
https://doi.org/10.1159/000349968...
The purpose of our study was to show epidemiological, clinical, paraclinical and therapeutic features of Moroccan patients with chronic heart failure who had developed chronic renal failure.
Methods
We conducted a monocentric, cross-sectional study on 563 patients attending the Unit of Heart Failure of the Department of Cardiology of the University Hospital Ibn Rushd of Casablanca in Morocco, during the 3-year period between July 30, 2012 and July 30, 2016.
The Unit of Heart failure is a day hospital attended only by stable patients, who are checked up every 3 or 6 months. Our patients were clinically stable and were followed up for the occurrence of cardiac events. The endpoints were cardiac death and any hospitalization due to worsening heart failure with or without an aggravation of renal function, acute coronary syndrome and severe arrhythmia. The mean follow up was 681 ± 105 days. Follow-up and events were adjudicated using medical consultations each three months and/or phone calls.
Patients were divided into two groups depending on whether they have developed a cardiorenal syndrome (CRS) or not.
Diagnosis of CRS type 2 was established based on Kidney Disease: Improving Global Outcomes (KDIGO)/Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines: albuminuria and/or GFR < 60 mL/in/1,73 m2, or a sustained decrease in GFR > 5ml/min/1,73 m2/year or > 10 ml/min/1,73 m2/5 years or sustained increase in albuminuria, along with documented or suspected appearance of congestive heart failure before the onset or progression of chronic kidney disease, and association of the event or degree of kidney disease with underlying heart disease.
Regarding echographic findings, a left ventricle was considered dilated when its diameter diastolic was above 57 mm in men and 53mm in women. The left atrium was considered dilated when its surface was greater than 15cm2 or diameter greater than 35 mm. The right ventricle was considered in systolic dysfunction if TAPSE (tricuspid annular plane systolic excursion) was less than 16mm, S-wave longitudinal velocity using DTI (Doppler tissue imaging) was less than 11.5 cm/s, or the fractional shortening was less than 30%. We defined pulmonary hypertension as any value of systolic pulmonary artery pressure, measured by the flow of tricuspid insufficiency greater than 40 mmHg.
The echocardiography was performed one month after starting treatment.
Baseline characteristics were the data recorded during the first consultation at the Heart Failure Unit. We included all patients who developed CRS at any time of the follow-up, even if it was at the first consultation.
Among the causes of readmission we selected patients who were admitted to emergency care for acute coronary syndrome, congestive heart failure or severe arrhythmia. We defined severe arrhythmia as any atrial or ventricular arrhythmia causing hemodynamic instability or requiring drug treatment.
We excluded all patients with renal failure secondary to another etiology including other CRSs, patients who did not meet the definition of CRS type 2, and hemodialysis patients.
Statistical analysis
Results are presented as the mean ± SD for continuous variables and as numbers and percentages for categorical variables. If data were not normally distributed, the Mann-Whitney U test was used. Baseline characteristics of patients in the two groups specified above were compared using the chi-square test for dichotomous variables and paired student's t-test for continuous variables. A p value < 0.05 was considered statistically significant. Significant variables selected in the univariate analysis were entered into the multivariable analysis. The cardiac event-free survival rates were calculated using the Kaplan-Meier analysis. All analyses were performed using SPSS statistical package, version 17.0(SPSS Inc, Chicago, IL).
Results
Clinical findings
Among the 563 patients analyzed, 46.5 %( 262 patients) had CRS type 2.
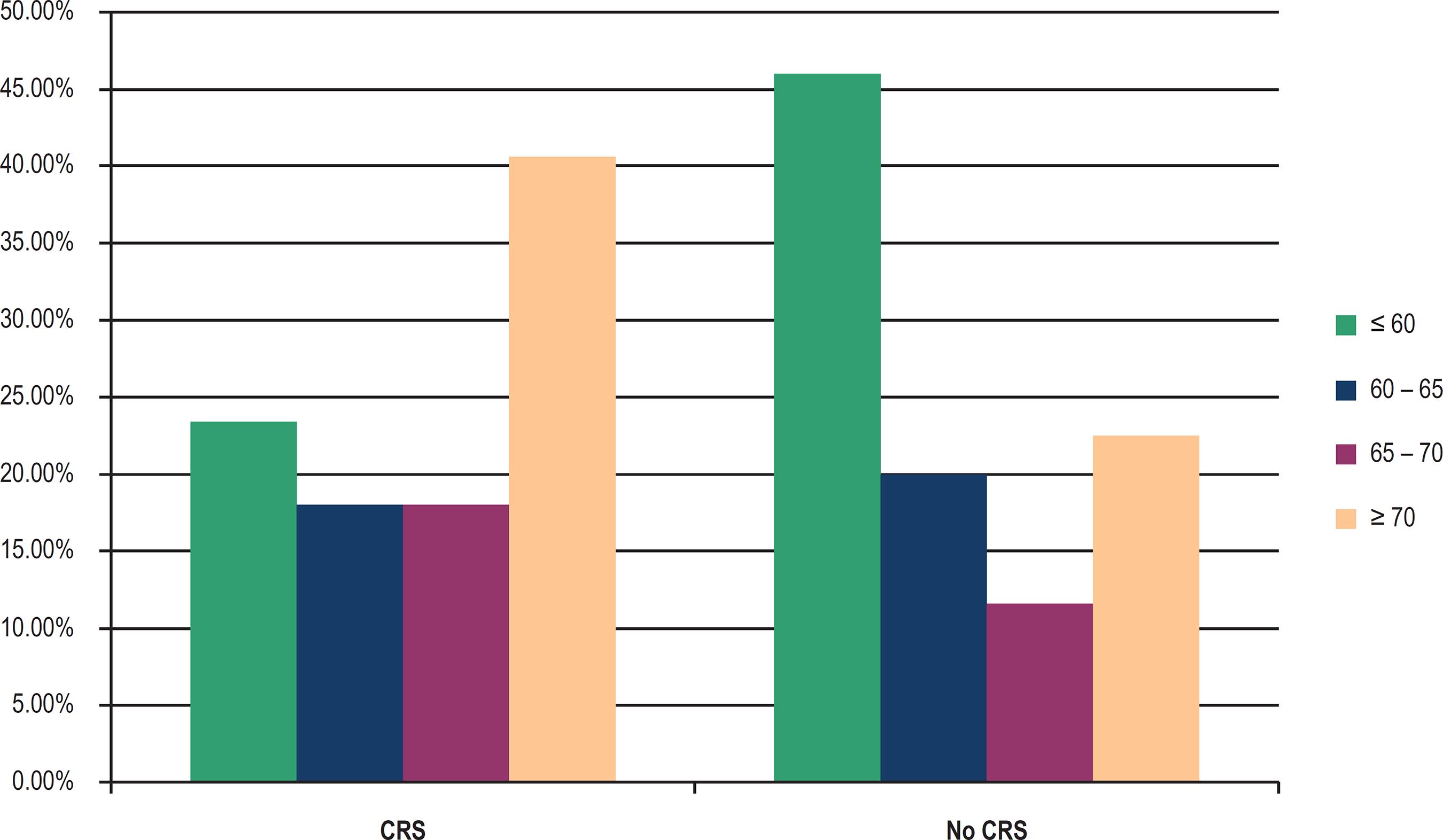
The mean age was significantly higher in the group CRS (67 years vs. 61). By dividing patients into four age brackets, CRS was more common in patients over 70 years (Figure 1).
Higher frequency of male was observed in both groups, 53.1% in the CRS group and 60.1% in the group without CRS, but the difference was not statistically significant (p = 0.105).
Concerning the risk factors, the percentage of patients with hypertension and diabetes was significantly higher in the CRS group compared to the group without CRS (55.3% and 42%, respectively, in the CRS group vs. 39.5% and 26.6%, respectively, in the group without CRS, p < 0.0001). Among hypertensive patients, the proportion of those with uncontrolled hypertension was significantly higher in the CRS group (16.8% vs. 9.3%).
No difference between the two groups was observed for other risk factors.
Clinically, New York Heart Association class III and IV was reported in 25.6% in the CRS vs. 13.3% in the group without CRS (p < 0.0001). Mean heart rate was slightly higher in the group CRS (p = 0.453).
Higher, but not significant proportion of patients with atrial fibrillation was observed in the CRS group (17.2% vs. 13%).
Table 1 summarizes all these features.
Biological findings
The mean serum levels of sodium, calcium, and hemoglobin were significantly lower in the CRS group (139.1, 91.4 and 12.3, respectively) than in the group without CRS (140.1, 93.5 and 13.05, respectively).
Inversely, mean levels of serum potassium, uric acid and C-reactive protein (CRP) were significantly higher in the CRS group (4.8, 71.4 and 24.6, respectively) than in the group without CRS (4.5, 53.3 and 11.5, respectively).
Echographic findings
Mean ejection fraction (EF), left atrial dimensions and deceleration time of mitral flow were significantly lower in the group with CRS cardiorenal syndrome (33.50%, 43.6 and 137.70 , respectively) than in the group without CRS (37.57%, 39.96, and 161.59, respectively). Systolic right ventricular function was impaired in 19.1 % of patients with CRS, and only 12% in the group without CRS (p = 0.025). Compared with the group without CRS, 56.5% of the patients who developed CRS had a pulmonary hypertension (p < 0.0001) (Table 1).
Therapy
Mean ejection fraction (EF) and deceleration time of mitral flow were significantly lower in the group with CRS (33.50% and 137.70 ms, respectively) than in the group without CRS (37.57% and 161.59 ms, respectively). Left atrial area was significantly higher in the group with CRS (21.73 cm2 vs. 18.95 cm2). Systolic right ventricular function was impaired in 19.1% of patients with CRS, and only 12% in the group without CRS (p = 0.025). Compared with the group without CRS, 56.5% of the patients who developed CRS had a pulmonary hypertension (p < 0.0001) (Table 1).
The multivariate analysis showed that age, hypertension, diabetes, low ejection fraction, pulmonary hypertension, left atrium diameter, time of deceleration of mitral flow, anemia, high CRP and hyperuricemia are independents risks factors of CRS.
Readmission
Readmission for congestive heart failure, severe arrhythmia or acute coronary event was more frequent in the group CRS, observed in 30.2% of patients vs. 5.3% (p < 0.0001) (Table 1).
Mortality and cardiac events
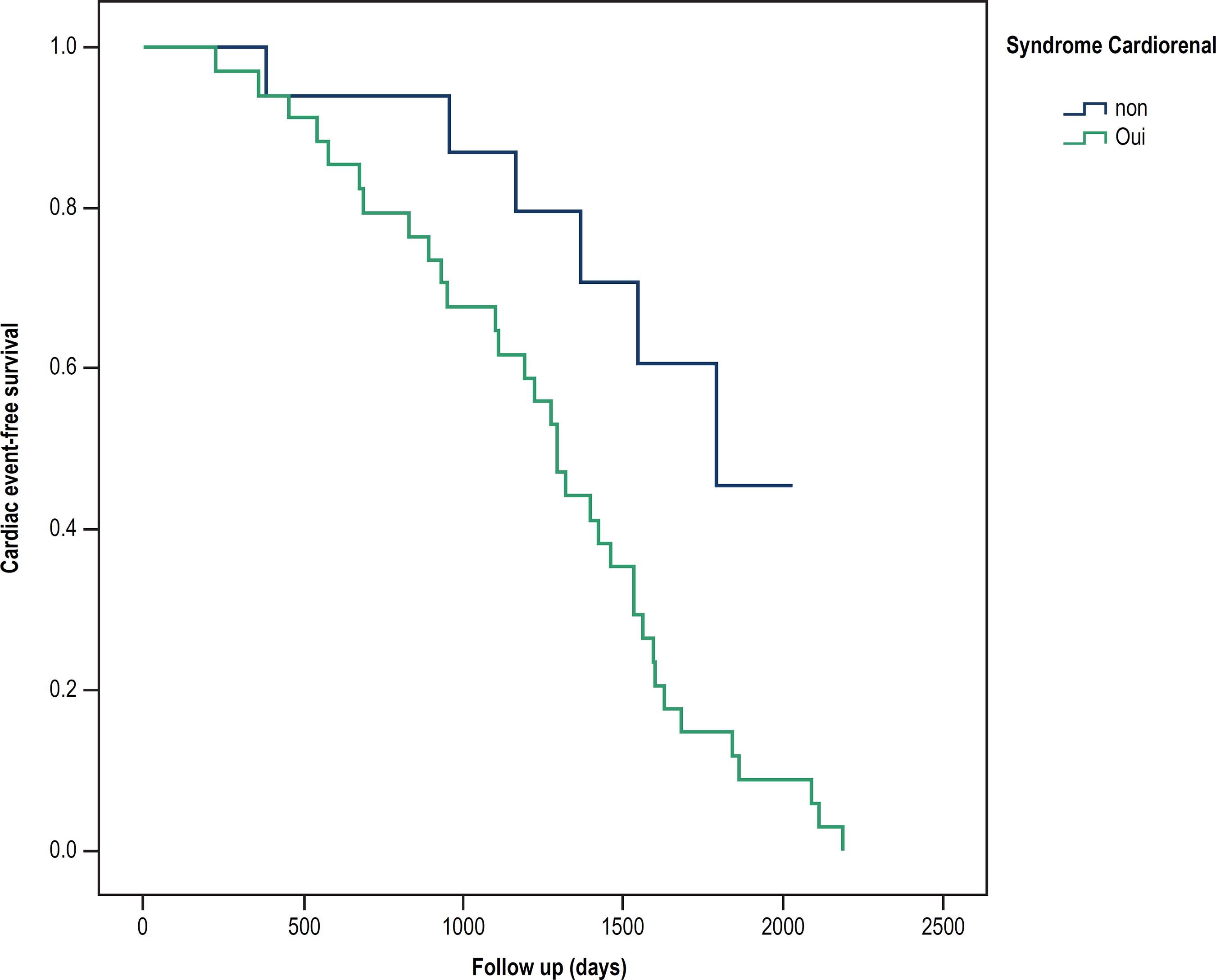
The mortality was significantly higher in the group CRS 13% vs. 2% in the group without CRS. Patients with CRS had higher rates of cardiac death and re-hospitalization due to worsening heart failure than those without CRS. This was also clearly demonstrated by Kaplan-Meier analysis (Figure 1).
Discussion
The major finding in our study was that, compared with patients without CRS, patients with CRS tended to be older, hypertensive and diabetic. Clinically, higher percentage of patients had dyspnea stage III or IV. Biologically, patients with CRS had lower hemoglobin and higher blood uric acid. Regarding echocardiographic findings, these patients also showed lower left ventricular EF, with higher prevalence of right ventricular and pulmonary hypertension, and higher risk of readmission.
The CRS is characterized by chronic abnormalities in cardiac function leading to kidney injury or dysfunction.44 Cruz DN, Gheorghiade M, Palazzuoli A, Ronco C, Bagshaw SM. Epidemiology and outcome of the cardio-renal syndrome. Heart Fail Rev. 2011;16(6):531-42. doi: 10.1007/s10741-010-9223-1. Erratum in: Heart Fail Rev. 2011;16(6):543.
https://doi.org/10.1007/s10741-010-9223-...
Worsening cardiac performance in heart failure results in renal hypoperfusion, with subsequent activation of the renin-angiotensin-aldosterone pathway and the sympathetic nervous system, which can further impair renal function. Chronic kidney disease and consequent uremia can lead to abnormal regulation of myocyte calcium homeostasis and contractile function, increased sympathetic activity, endothelial dysfunction, microvessel dysfunction and accelerated atherosclerosis.55 Jois P, Mebazaa A. Cardio-renal syndrome type 2: epidemiology, pathophysiology, and treatment. Semin Nephrol. 2012;32(1):26-30. doi: 10.1016/j.semnephrol.2011.11.004.
https://doi.org/10.1016/j.semnephrol.201...
,66 Ronco C, Haapio M, House AA, Anavekar N, Bellomo R. Cardiorenal syndrome. J Am Coll Cardiol. 2008;52(19):1527-39. doi: 10.1016/j.jacc.2008.07.051.
https://doi.org/10.1016/j.jacc.2008.07.0...
Pre-existing chronic renal failure is found in 45% of chronic heart failure patients, and is associated with a higher risk of hospitalization and death77 Heywood JT, Fonarow GC, Costanzo MR, Mathur VS, Wigneswaran JR, Wynne J; ADHERE Scientific Advisory Committee and Investigators. High prevalence of renal dysfunction and its impact on outcome in 118465 patients hospitalized with acute decompensated heart failure: a report from ADHERE Database. J Card Fail. 2007;13(6):422-30. doi: 10.1016/j.cardfail.2007.03.011.
https://doi.org/10.1016/j.cardfail.2007....
. This percentage is consistent with that of our series (46.5 % of patients with CRS).
Deterioration of renal function increases with age. In our study, patients with CRS were relatively older than patients with normal renal function. In all the studies that have been conducted, advanced age was a factor associated with the occurrence of the CRS. In the study by Lu et al.,88 Lu KJ, Kearney LG, Hare DL, Ord M, Toia D, Jones E, et al. Cardiorenal anemia syndrome as a prognosticator for death in heart failure. Am J Cardiol. 2013;111(8):1187-91. doi: 10.1016/j.amjcard.2012.12.049.
https://doi.org/10.1016/j.amjcard.2012.1...
mean age of patients with CRS was 77 ± 8 years.
In our study, diabetes and uncontrolled hypertension were the major risk factors found in patients with CRS. It has been suggested an interplay of diabetes and/or hypertension- induced and heart failure-associated renal injury with a related and mutually perpetuating pathophysiology, as it was demonstrated in the model of Kishimoto et al.99 Kishimoto T, Maekawa M, Abe Y, Yamamoto K. Intrarenal distribution of blood flow and renin release during renal venous pressure elevation. Kidney Int. 1973;4(4):259-66. PMID: 4752169.
Anemia is associated with high mortality in all patients with heart failure and reflects an advanced state of the disease. Also, it is particularly considered as an independent risk factor of morbidity and mortality in all CRSs.1010 Horwich TB, Fonarow GC, Hamilton MA, MacLellan WR, Borenstein J. Anemia is associated with worse symptoms symptoms, greater impairement in functional capacity and a significant increase in mortality in patients with advanced heart failure. J Am Coll Cardiol. 2002;39(11):1780-6. PMID: 12039491. Sato et al.1111 Sato T, Yamauchi H, Suzuki S, Yoshihisa A, Yamaki T, Sugimoto K, et al. Distinct prognostic factors in patients with chronic heart failure and chronic kidney disease. Int Heart J. 2013;54(5):311-7. PMID: 24097222. reported that peak VO2, B-type natriuretic peptide levels, anemia and uric acid levels were independent prognostic factors of type 2 CRS1111 Sato T, Yamauchi H, Suzuki S, Yoshihisa A, Yamaki T, Sugimoto K, et al. Distinct prognostic factors in patients with chronic heart failure and chronic kidney disease. Int Heart J. 2013;54(5):311-7. PMID: 24097222.. Anemia, chronic heart failure and chronic kidney disease are capable of causing or worsening each other, forming a vicious circle.1212 Silverberg D, Wexler D, Blum M, Wollman Y, Iaina A. The cardio-renal anaemia syndrome: does it exist? Nephrol Dial Transplant. 2003;18 suppl 8:viii7-12. PMID: 14607993. Recently, a new term has been used - cardiorenal anemia syndrome. In all studies on heart failure, the average hemoglobin level was lower in the group with chronic renal failure, which was associated with a risk of re-hospitalization and higher mortality rates. Lu et al.88 Lu KJ, Kearney LG, Hare DL, Ord M, Toia D, Jones E, et al. Cardiorenal anemia syndrome as a prognosticator for death in heart failure. Am J Cardiol. 2013;111(8):1187-91. doi: 10.1016/j.amjcard.2012.12.049.
https://doi.org/10.1016/j.amjcard.2012.1...
had reported a 4-year death rate of 51% in patients with cardiorenal anemia syndrome vs. 26% in those without the syndrome. Age and serum potassium were the predictive factors cardiorenal anemia syndrome progression among patients with heart failure.1313 Lu KJ, Kearney LG, Hare DL, Ord M, Toia D, Jones E, et al. Cardiorenal anemia syndrome as a prognosticator for death in heart failure. Am J Cardiol. 2013;111(8):1187-91. doi: 10.1016/j.amjcard.2012.12.049.
https://doi.org/10.1016/j.amjcard.2012.1...
More recently, it has been shown that anemia is common in diabetes mellitus, with chronic kidney disease and functional erythropoietin deficiency hypothesized as major contributing factors.1414 Thomas MC. The high prevalence of anemia in diabetes is linked to functional erythropoietin deficiency. Semin Nephrol. 2006;26:275-82. doi: 10.1016/j.semnephrol.2006.05.003.
https://doi.org/10.1016/j.semnephrol.200...
Kaplan-Meier cardiac event-free survival analysis in patients with and without cardiorenal syndrome
Recent progresses in the treatment of anemia in heart failure have focused on the use of erythropoiesis-stimulating agents and intravenous iron transfusion. A recent meta-analysis involving more than 11 studies concluded that erythropoiesis-stimulating agents help improve symptoms, reduce hospitalization, and mortality.1515 Ngo K, Kotecha D, Walters JA, Manzano L, Palazzuoli A, Van Veldhuisen DJ, et al. Erythropoiesis-stimulating agents for anemia in chronic heart failure patients. Cochrane Database Syst Rev. 2010 Jan 20;(1):CD007613. doi: 10.1002/14651858.CD007613.pub2.
https://doi.org/10.1002/14651858.CD00761...
In our study, patients with CRS were less likely to be treated with beta-blocker, and more likely to receive loop diuretics and calcium channel blockers. This is explained by a higher rate of congestive heart failure, difficulties in the control of blood pressure and symptoms, and diuretic resistance. The cause of diuretic resistance is multifactorial: inadequate dosing of diuretic, increased sodium intake, delayed intestinal absorption of drugs, decreased diuretic tubular secretion, renal underperfusion and use of non-steroidal anti-inflammatory drugs.1616 Kshatriya S, Kozman H, Siddiqui D, Bhatta L, Liu K, Salah A, et al. The cardiorenal syndrome in heart failure: an evolving paradigm. Am J Med Sci.2010;340(1):33-7. doi: 10.1097/MAJ.0b013e3181e59108.
https://doi.org/10.1097/MAJ.0b013e3181e5...
Our study had some limitations. This is an observational study and reflects the data from patients only from a single center, which is not representative of the Moroccan population. Some patients were not included, such as hemodialysis patients, who have a worse prognosis, to not create an ambiguity between all types of CRS. For this reason, a cause-consequence relationship has not been clearly established.
Conclusion
Deterioration of renal function in chronic renal failure is associated with poor prognosis, including a high risk of rehospitalization, cardiovascular events and death. More attention should be paid to elderly, diabetic patients, with a very low left ventricular EF or pulmonary hypertension.
References
-
1de Silva R, Nikitin NP, Witte KK, Rigby AS, Goode K, Bhandari S, et al. Incidence of renal dysfunction over 6 months in patients with chronic heart failure due to left ventricular systolic dysfunction: contributing factors and relationship to prognosis. Eur Heart J. 2006;27(5):569-81. doi: 10.1093/eurheartj/ehi696.
» https://doi.org/10.1093/eurheartj/ehi696 -
2Cole RT, Masoumi A, Triposkiadis F, Giamouzis G, Georgiopoulou V, Kalogeropoulos A, et al. Renal dysfunction in heart failure. Med Clin North Am. 2012;96(5):955-74. doi: 10.1016/j.mcna.2012.07.005.
» https://doi.org/10.1016/j.mcna.2012.07.005 -
3Cruz DN, Schmidt-Ott KM, Vescovo G, House AA, Kellum JA, Ronco C, et al. Pathophysiology of cardiorenal syndrome type 2 in stable chronic heart failure: workgroup statements from the eleventh consensus conference of the Acute Dialysis Quality Initiative (ADQI). Contrib Nephrol. 2013;182:117-36. doi: 10.1159/000349968.
» https://doi.org/10.1159/000349968 -
4Cruz DN, Gheorghiade M, Palazzuoli A, Ronco C, Bagshaw SM. Epidemiology and outcome of the cardio-renal syndrome. Heart Fail Rev. 2011;16(6):531-42. doi: 10.1007/s10741-010-9223-1. Erratum in: Heart Fail Rev. 2011;16(6):543.
» https://doi.org/10.1007/s10741-010-9223-1 -
5Jois P, Mebazaa A. Cardio-renal syndrome type 2: epidemiology, pathophysiology, and treatment. Semin Nephrol. 2012;32(1):26-30. doi: 10.1016/j.semnephrol.2011.11.004.
» https://doi.org/10.1016/j.semnephrol.2011.11.004 -
6Ronco C, Haapio M, House AA, Anavekar N, Bellomo R. Cardiorenal syndrome. J Am Coll Cardiol. 2008;52(19):1527-39. doi: 10.1016/j.jacc.2008.07.051.
» https://doi.org/10.1016/j.jacc.2008.07.051 -
7Heywood JT, Fonarow GC, Costanzo MR, Mathur VS, Wigneswaran JR, Wynne J; ADHERE Scientific Advisory Committee and Investigators. High prevalence of renal dysfunction and its impact on outcome in 118465 patients hospitalized with acute decompensated heart failure: a report from ADHERE Database. J Card Fail. 2007;13(6):422-30. doi: 10.1016/j.cardfail.2007.03.011.
» https://doi.org/10.1016/j.cardfail.2007.03.011 -
8Lu KJ, Kearney LG, Hare DL, Ord M, Toia D, Jones E, et al. Cardiorenal anemia syndrome as a prognosticator for death in heart failure. Am J Cardiol. 2013;111(8):1187-91. doi: 10.1016/j.amjcard.2012.12.049.
» https://doi.org/10.1016/j.amjcard.2012.12.049 -
9Kishimoto T, Maekawa M, Abe Y, Yamamoto K. Intrarenal distribution of blood flow and renin release during renal venous pressure elevation. Kidney Int. 1973;4(4):259-66. PMID: 4752169.
-
10Horwich TB, Fonarow GC, Hamilton MA, MacLellan WR, Borenstein J. Anemia is associated with worse symptoms symptoms, greater impairement in functional capacity and a significant increase in mortality in patients with advanced heart failure. J Am Coll Cardiol. 2002;39(11):1780-6. PMID: 12039491.
-
11Sato T, Yamauchi H, Suzuki S, Yoshihisa A, Yamaki T, Sugimoto K, et al. Distinct prognostic factors in patients with chronic heart failure and chronic kidney disease. Int Heart J. 2013;54(5):311-7. PMID: 24097222.
-
12Silverberg D, Wexler D, Blum M, Wollman Y, Iaina A. The cardio-renal anaemia syndrome: does it exist? Nephrol Dial Transplant. 2003;18 suppl 8:viii7-12. PMID: 14607993.
-
13Lu KJ, Kearney LG, Hare DL, Ord M, Toia D, Jones E, et al. Cardiorenal anemia syndrome as a prognosticator for death in heart failure. Am J Cardiol. 2013;111(8):1187-91. doi: 10.1016/j.amjcard.2012.12.049.
» https://doi.org/10.1016/j.amjcard.2012.12.049 -
14Thomas MC. The high prevalence of anemia in diabetes is linked to functional erythropoietin deficiency. Semin Nephrol. 2006;26:275-82. doi: 10.1016/j.semnephrol.2006.05.003.
» https://doi.org/10.1016/j.semnephrol.2006.05.003 -
15Ngo K, Kotecha D, Walters JA, Manzano L, Palazzuoli A, Van Veldhuisen DJ, et al. Erythropoiesis-stimulating agents for anemia in chronic heart failure patients. Cochrane Database Syst Rev. 2010 Jan 20;(1):CD007613. doi: 10.1002/14651858.CD007613.pub2.
» https://doi.org/10.1002/14651858.CD007613.pub2 -
16Kshatriya S, Kozman H, Siddiqui D, Bhatta L, Liu K, Salah A, et al. The cardiorenal syndrome in heart failure: an evolving paradigm. Am J Med Sci.2010;340(1):33-7. doi: 10.1097/MAJ.0b013e3181e59108.
» https://doi.org/10.1097/MAJ.0b013e3181e59108
Publication Dates
-
Publication in this collection
Sep-Oct 2017
History
-
Received
22 Oct 2016 -
Reviewed
04 Nov 2016 -
Accepted
24 Feb 2017